Explain chephelosporins
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed for a thorough answer. Here is a complete explanation of cephalosporins:
Cephalosporins
Cephalosporins are beta-lactam antibiotics that share the same fundamental mechanism as penicillins - they inhibit bacterial cell wall synthesis by binding to penicillin-binding proteins (PBPs). They are classified into five generations based on their spectrum of antimicrobial activity.
Chemistry
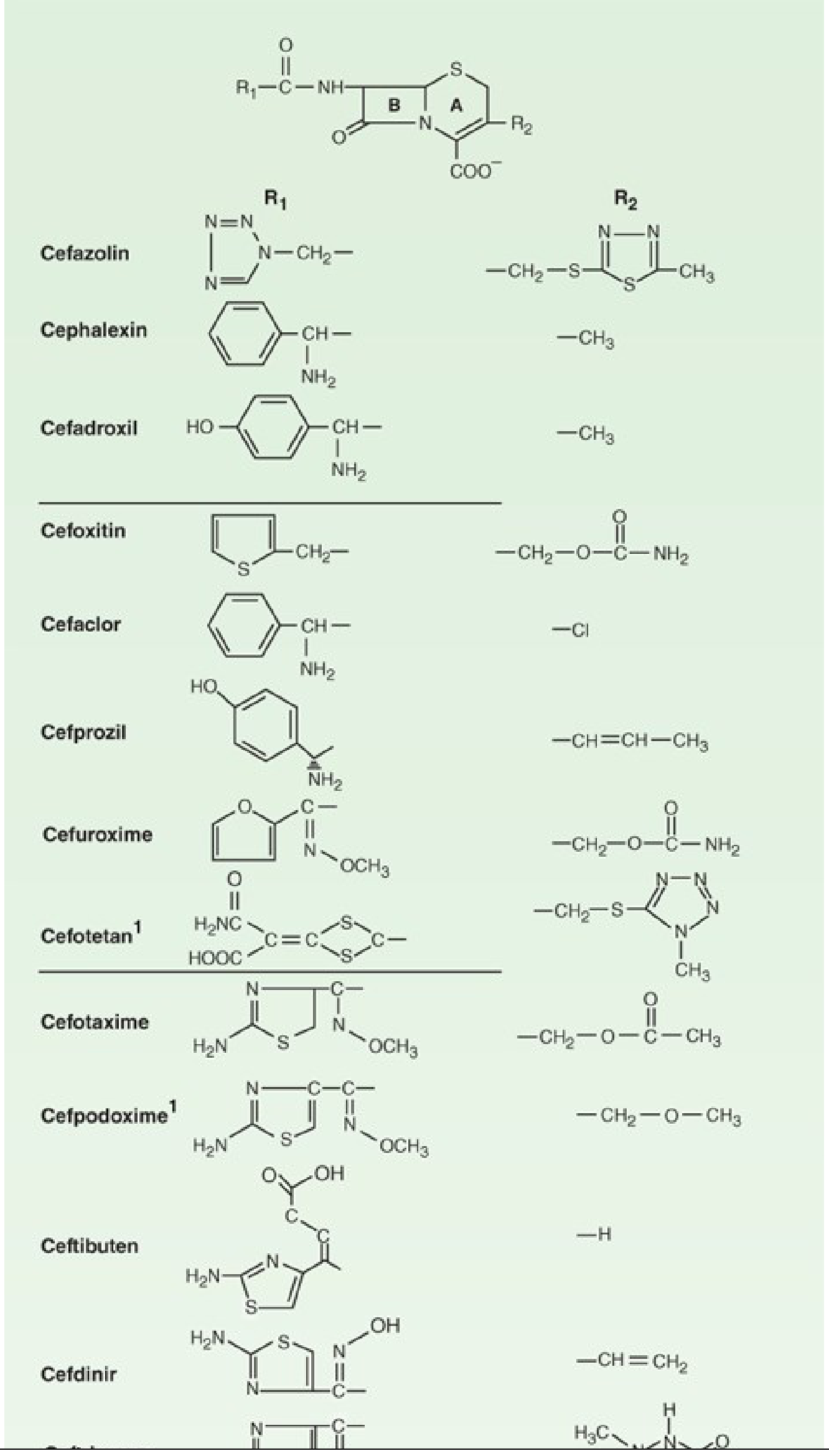
The core structure is 7-aminocephalosporanic acid (7-ACA) - a bicyclic ring system consisting of a beta-lactam ring (ring B) fused to a dihydrothiazine ring (ring A), plus a carboxylate group. This differs from penicillin's 6-aminopenicillanic acid, which has a thiazolidine ring instead.
The two attachment points, R1 (at position 7 of the beta-lactam) and R2 (at position 3 of the dihydrothiazine ring), are where different chemical groups are attached to create hundreds of compounds with varying pharmacokinetic and antibacterial profiles.
Mechanism of Action
Like all beta-lactams, cephalosporins:
- Enter the bacterial cell and bind covalently to PBPs (transpeptidases, carboxypeptidases)
- Inhibit cross-linking of peptidoglycan chains (transpeptidation step)
- Trigger autolytic enzymes that degrade the cell wall
- Cause cell lysis and death
They are bactericidal and exhibit time-dependent killing - efficacy depends on the time free drug concentration stays above the MIC (not on peak concentration).
Resistance Mechanisms
Three main mechanisms (shared with penicillins):
- Beta-lactamase production - enzymes hydrolyze the beta-lactam ring, destroying activity. This is the most clinically important mechanism. Gram-positive bacteria secrete beta-lactamases extracellularly; gram-negative bacteria do so in the periplasmic space.
- Altered PBPs - Modified PBPs with lower affinity for beta-lactams. Classic example: MRSA has mecA gene producing a modified PBP2a, conferring resistance to virtually all cephalosporins (except the newer 5th-generation agents).
- Decreased permeability / efflux pumps - Reduced penetration through outer membrane porins (especially in gram-negatives like P. aeruginosa) or active efflux of drug.
- Lippincott Illustrated Reviews: Pharmacology, p. 948
Generations
First Generation
Drugs: Cefazolin (IV), Cephalexin (oral), Cefadroxil (oral)
Spectrum:
- Excellent gram-positive coverage: streptococci, MSSA (Methicillin-sensitive Staphylococcus aureus)
- Modest gram-negative: E. coli, K. pneumoniae, Proteus mirabilis (the "3 Keps")
- Gram-positive anaerobes (peptococci, peptostreptococci)
- NOT active against: MRSA, Pseudomonas, Enterobacter, Serratia, Bacteroides fragilis
Key uses:
- Cefazolin: Surgical prophylaxis (most common antibiotic used perioperatively), skin/soft tissue infections, MSSA bacteremia
- Cephalexin: Uncomplicated skin infections, UTIs
Pharmacokinetics: Cephalexin is absorbed orally (500 mg q6h). Cefazolin is IV only; achieves excellent tissue levels. Most 1st-generation agents are excreted renally unchanged - dose reduction required in renal impairment.
- Katzung's Basic and Clinical Pharmacology, 16th Ed., p. 1247
Second Generation
Drugs: Cefuroxime, Cefaclor, Cefprozil (oral); Cefoxitin, Cefotetan (parenteral - the "cephamycins")
Spectrum:
- Greater gram-negative activity than 1st generation: H. influenzae, Klebsiella spp., Moraxella catarrhalis, Proteus spp., E. coli
- Slightly weaker gram-positive coverage than 1st generation
- Cephamycins only (cefoxitin, cefotetan): Also cover anaerobes including B. fragilis - making them unique among cephalosporins. However, increasing resistance among B. fragilis limits their use.
Key uses:
- Cefuroxime: Community-acquired pneumonia, sinusitis
- Cefoxitin/cefotetan: Intra-abdominal infections, gynecologic infections, surgical prophylaxis for bowel surgery
- Lippincott Illustrated Reviews: Pharmacology, p. 957
Third Generation
Drugs: Ceftriaxone, Cefotaxime (parenteral); Cefdinir, Cefixime, Cefpodoxime, Ceftibuten (oral); Ceftazidime (anti-pseudomonal)
Spectrum:
- Markedly expanded gram-negative coverage including Serratia marcescens, Enterobacter aerogenes, and most Enterobacteriaceae
- Less potent against MSSA compared to 1st generation
- Ceftriaxone and cefotaxime: Excellent CNS penetration - drugs of choice for bacterial meningitis
- Ceftazidime: Unique anti-Pseudomonas activity among 3rd-gen agents
Key uses:
- Ceftriaxone: Bacterial meningitis (with vancomycin), community-acquired pneumonia, gonorrhea, Lyme disease, typhoid fever, sepsis
- Cefotaxime: Meningitis, serious gram-negative infections
- Ceftazidime: Pseudomonal infections
Note: 3rd-generation cephalosporins can induce chromosomally-encoded beta-lactamases in some organisms (e.g., Enterobacter) - known as AmpC beta-lactamases.
Fourth Generation
Drug: Cefepime (IV only)
Spectrum:
- Combines the gram-positive activity of 1st-gen with the gram-negative breadth of 3rd-gen
- Anti-Pseudomonas activity (like ceftazidime)
- Greater stability against beta-lactamases (AmpC) than 3rd generation
- Does NOT cover MRSA or anaerobes
Key uses: Febrile neutropenia, hospital-acquired pneumonia, serious gram-negative infections where AmpC-producing organisms are suspected
Fifth Generation (Anti-MRSA Cephalosporins)
Drugs: Ceftaroline, Ceftobiprole
Spectrum:
- Cover MRSA (by binding to the modified PBP2a) - the defining feature of this class
- Broad gram-negative coverage similar to 3rd generation
- Does NOT cover Pseudomonas
Key uses: Complicated skin/soft tissue infections, community-acquired pneumonia (ceftaroline FDA-approved)
Siderophore Cephalosporin (Newest)
Drug: Cefiderocol
This novel agent uses a "Trojan horse" mechanism - it is conjugated to a catecholamine siderophore, allowing it to enter bacteria via iron uptake transporters (siderophore channels), bypassing usual resistance mechanisms. It has activity against carbapenem-resistant gram-negatives including Pseudomonas, Acinetobacter, and Klebsiella with carbapenemase production.
- Katzung's Basic and Clinical Pharmacology, 16th Ed., p. 1286
Summary of Coverage by Generation
| Feature | Gen 1 | Gen 2 | Gen 3 | Gen 4 | Gen 5 |
|---|---|---|---|---|---|
| Gram-positive (MSSA) | +++ | ++ | + | ++ | +++ (incl. MRSA) |
| Gram-negative (basic) | + | ++ | +++ | +++ | +++ |
| Pseudomonas | - | - | Ceftazidime only | + | - |
| Anaerobes | - | Cephamycins only | - | - | - |
| CNS penetration | Poor | Cefuroxime (moderate) | Excellent | Good | Good |
| Beta-lactamase stability | Low | Moderate | Good | Better | Best |
Adverse Effects
-
Hypersensitivity reactions - Most common. About 1-2% of patients develop reactions. Cross-reactivity with penicillin is approximately 1-2% (much lower than the historically cited 10%, which was due to shared contaminants in early manufacturing). Patients with a history of severe penicillin anaphylaxis should avoid cephalosporins.
-
GI effects - Nausea, diarrhea, particularly with oral agents. Broad-spectrum agents can cause C. difficile colitis.
-
Nephrotoxicity - Rare with modern cephalosporins; risk increased when combined with aminoglycosides.
-
Disulfiram-like reaction - Cefotetan and cefoperazone contain a methylthiotetrazole (MTT) side chain that inhibits aldehyde dehydrogenase. Patients must avoid alcohol.
-
Hypoprothrombinemia / bleeding - Also due to MTT side chains (affect vitamin K metabolism). Monitor coagulation in at-risk patients.
-
Positive Coombs test - Cephalosporins can adsorb onto red blood cells, giving a false-positive direct Coombs without clinical hemolysis.
Key Clinical Pearls
- Surgical prophylaxis: Cefazolin is the gold-standard single-dose preoperative antibiotic for most clean and clean-contaminated procedures.
- Meningitis: 3rd-gen (ceftriaxone or cefotaxime) + vancomycin is standard empiric therapy for bacterial meningitis in immunocompetent adults.
- Renal dosing: Most cephalosporins require dose adjustment in renal impairment. Ceftriaxone is the notable exception - it is primarily biliary-excreted and does not need renal dose adjustment.
- Ceftriaxone and calcium: Avoid concomitant IV calcium in neonates (risk of precipitation in lungs and kidneys).
- ESBL-producing organisms: Extended-spectrum beta-lactamases (ESBLs) hydrolyze all cephalosporins. Carbapenems are the treatment of choice for serious ESBL infections.
Sources: Katzung's Basic and Clinical Pharmacology, 16th Ed. | Lippincott Illustrated Reviews: Pharmacology
This is a shared conversation. Sign in to Orris to start your own chat.