Aboral means
Aboral means "away from the mouth" or "on the opposite side of the body from the mouth."
It comes from the Latin prefix ab- (away from) + os/oris (mouth).
It is the anatomical opposite of oral (toward or near the mouth), and is commonly used in zoology and invertebrate anatomy - for example, describing the upper surface of a sea urchin or starfish, which is the side facing away from the mouth.
Define the mechanicsm of. The Hcl and factors influencing them and also about the GERD give answer for 15m
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Excellent! I have all the material needed. Here is the full 15-mark answer:
Mechanism of HCl Secretion, Factors Influencing It, and GERD
PART 1: MECHANISM OF HCl SECRETION
Site and Cell of Secretion
HCl is secreted exclusively by the parietal (oxyntic) cells of the oxyntic glands, located in the body and fundus of the stomach. Each parietal cell contains large branching intracellular canaliculi where HCl is formed and from which it is discharged into the gland lumen.
- The secreted acid has a concentration of ~160 mEq/L HCl
- pH is approximately 0.8 (extremely acidic)
- The H+ concentration is about 3 million times that of arterial blood
- This requires over 1500 calories of energy per litre of gastric juice
(Guyton and Hall Textbook of Medical Physiology)
Cellular Mechanism (Step-by-Step)
The driving force is the H⁺-K⁺ ATPase (proton pump) located on the canalicular membrane of the parietal cell.
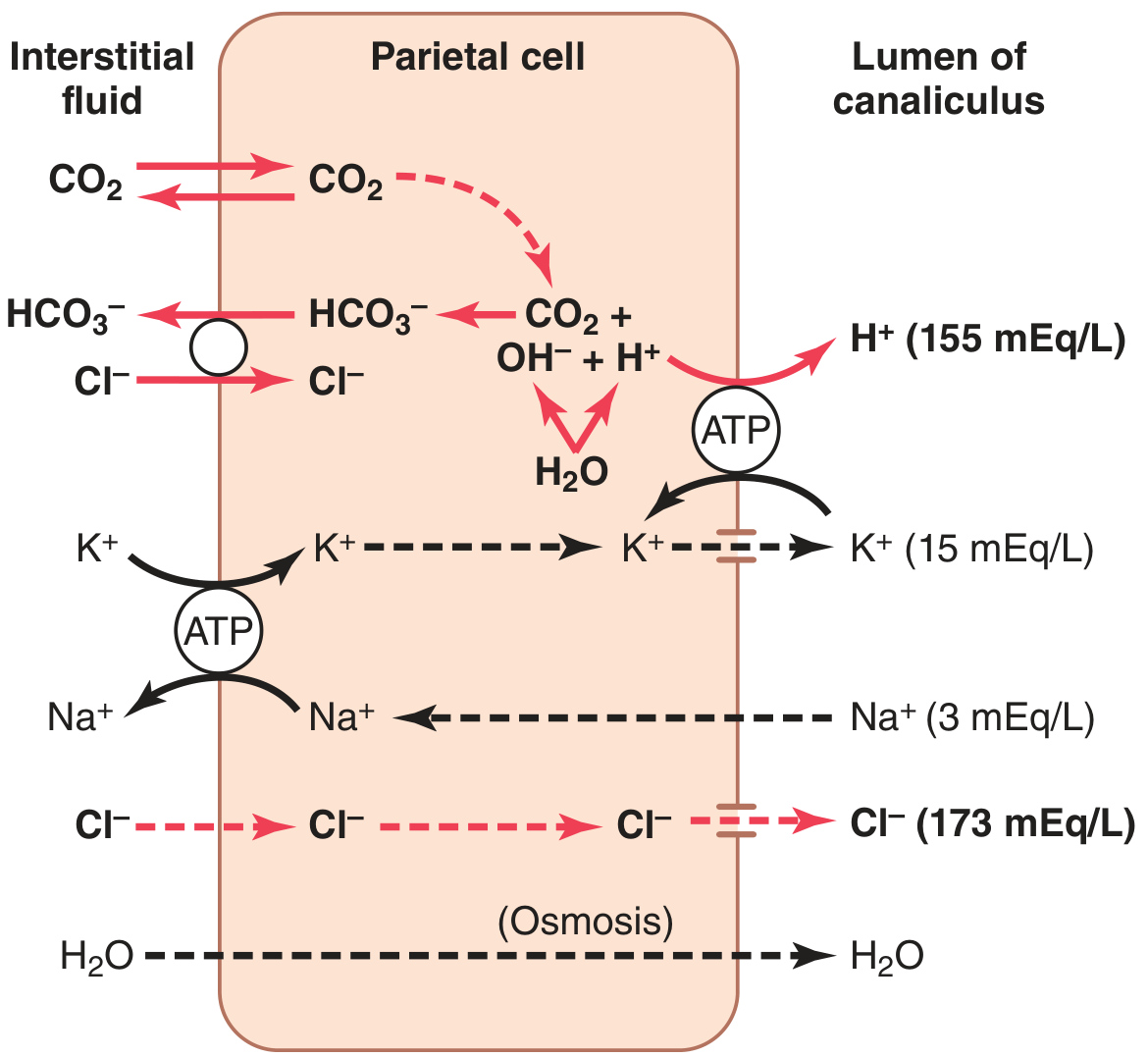
Steps:
-
Water dissociation: H₂O inside the parietal cell dissociates into H⁺ and OH⁻ in the cytoplasm.
-
H⁺ pumping: The H⁺-K⁺ ATPase actively pumps H⁺ out of the cell into the canalicular lumen in exchange for K⁺. This is the final common pathway for acid secretion.
-
HCO₃⁻ formation: The OH⁻ that accumulates combines with CO₂ (from metabolism or from blood) to form HCO₃⁻, a reaction catalyzed by carbonic anhydrase.
-
Cl⁻/HCO₃⁻ exchange: HCO₃⁻ crosses the basolateral membrane into the blood in exchange for Cl⁻ (this is the "alkaline tide" - gastric venous blood has a higher pH than arterial blood during active secretion).
-
Cl⁻ secretion: Cl⁻ enters the cell and is secreted through chloride channels into the canalicular lumen, joining the H⁺ to form HCl (~155 mEq/L H⁺, ~173 mEq/L Cl⁻, ~15 mEq/L K⁺).
-
Water: Follows by osmosis into the canaliculus.
Final secretion from the canaliculus: water, HCl (~150-160 mEq/L), KCl (~15 mEq/L), small amount of NaCl.
PART 2: FACTORS INFLUENCING HCl SECRETION
A. Stimulatory Factors
There are three primary stimulants acting on parietal cells:
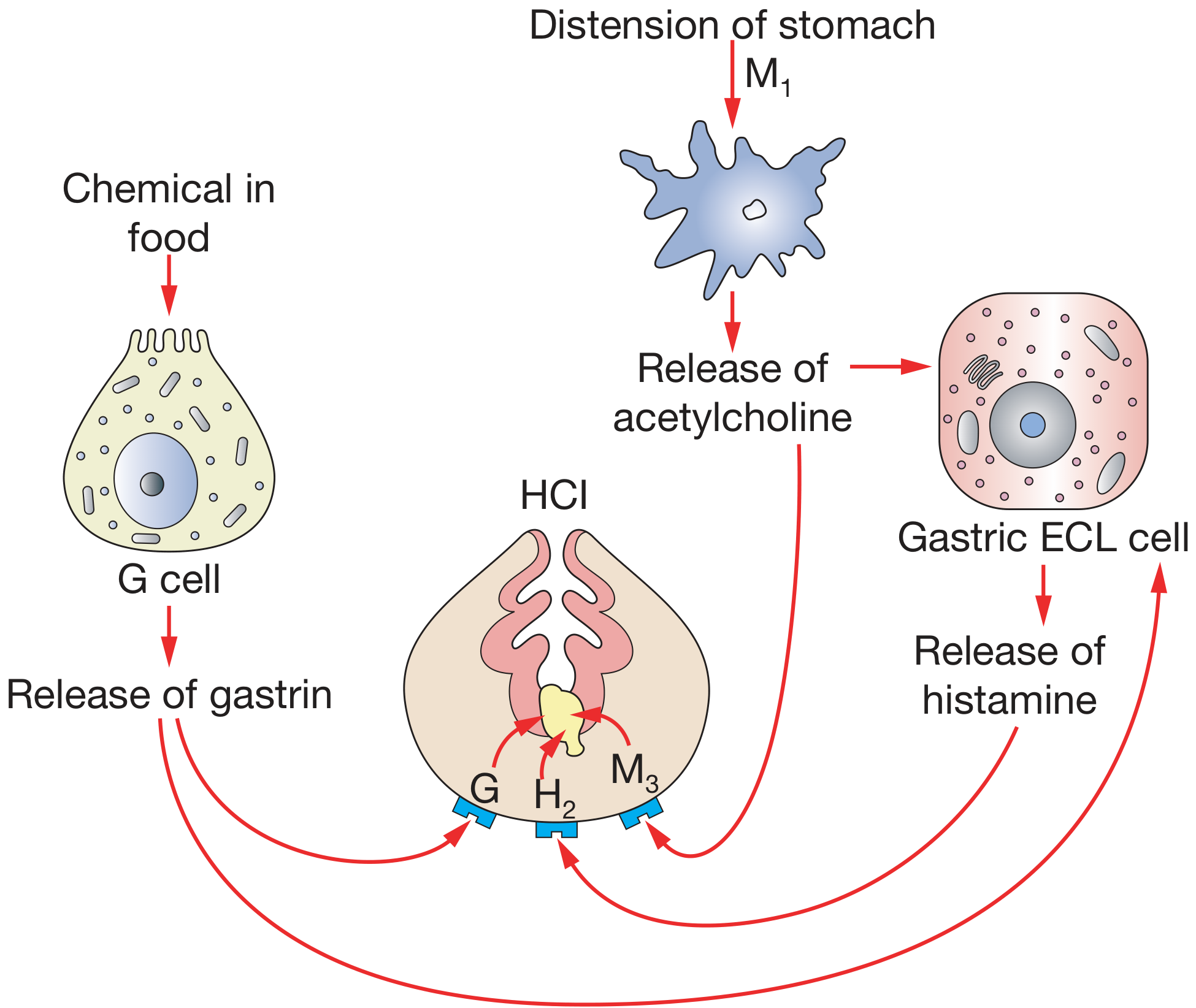
| Stimulant | Source | Receptor on Parietal Cell | Mechanism |
|---|---|---|---|
| Histamine | ECL cells (paracrine) | H₂ receptor | Increases cAMP → protein kinase A → activates H⁺-K⁺ ATPase |
| Gastrin | G cells of antrum | CCK-B/gastrin receptor | Stimulates ECL cells to release histamine; also acts directly on parietal cell |
| Acetylcholine (ACh) | Vagus nerve (parasympathetic) | M₃ (muscarinic) receptor | Increases intracellular Ca²⁺ → activates proton pump |
Histamine is the most potent direct stimulant of acid secretion. Gastrin acts mainly by releasing histamine from ECL cells. This explains why PPIs (which block the H⁺-K⁺ ATPase - the final common pathway) are more effective than H₂ blockers.
(Bailey and Love's Short Practice of Surgery, 28th Edition)
B. Three Phases of Gastric Secretion
1. Cephalic Phase (~30% of total)
- Triggered by sight, smell, taste, or thought of food
- Mediated by vagus nerve via dorsal motor nucleus
- Acetylcholine released → stimulates parietal cells and G cells
- Demonstrates conditioned reflex (Pavlov's experiments)
2. Gastric Phase (~60% of total)
- Triggered when food enters the stomach
- Three mechanisms: (a) long vagovagal reflexes, (b) local enteric reflexes, (c) gastrin mechanism
- Protein in food stimulates G cells to release gastrin → ECL cells → histamine → parietal cells
- Gastric distension is also a trigger
3. Intestinal Phase (~10% of total)
- Chyme in the duodenum stimulates small amounts of gastrin from duodenal mucosa
- Relatively minor contribution
(Guyton and Hall Textbook of Medical Physiology)
C. Inhibitory Factors
| Factor | Mechanism |
|---|---|
| Somatostatin (D cells) | Released in response to luminal acidification; inhibits G cells, ECL cells, and parietal cells directly |
| Secretin | Released by S cells of duodenum when acid enters; inhibits gastrin secretion |
| GIP (Glucose-dependent Insulinotropic Peptide) | Released from duodenum by fat; inhibits acid secretion |
| VIP (Vasoactive Intestinal Peptide) | Inhibits gastric acid secretion |
| Enterogastric reflex | Fat, acid, or hypertonic solutions in duodenum trigger this reverse reflex via sympathetic/vagal pathways |
| Low luminal pH (<2) | Negative feedback - directly inhibits G cells, stops gastrin release |
D. Other Factors Influencing Secretion
- NSAIDs and Aspirin: Damage the gastric mucosal barrier, allow acid backleak
- Alcohol: Breaks down the mucous barrier
- H. pylori infection: Disrupts the normal feedback; associated with increased gastrin and acid secretion
- Stress: Stimulates vagal pathways, increasing acid output
- Caffeine: Acts as a partial histamine-like stimulus
PART 3: GASTROESOPHAGEAL REFLUX DISEASE (GERD)
Definition
Gastroesophageal Reflux (GER) is a physiologic process by which gastric contents move retrograde from stomach to esophagus. It occurs several times a day normally and is not disease.
GERD is a spectrum of disease resulting from failure of the normal antireflux barrier, producing troublesome symptoms (heartburn, regurgitation) and/or complications (esophagitis, stricture, Barrett's esophagus). It is one of the most common GI diseases worldwide.
(Sleisenger and Fordtran's Gastrointestinal and Liver Disease)
Pathophysiology / Antireflux Mechanisms (and Their Failure)
The antireflux barrier has several components, all of which can fail in GERD:
1. Lower Esophageal Sphincter (LES) - Primary barrier
- Normal LES pressure: 10-45 mmHg
- Key factors for LES competence:
- Adequate LES length (at least 2 cm must be intra-abdominal)
- Adequate resting pressure
- Appropriate angle of His
- Transient LES relaxations (TLESRs) - most common mechanism of reflux; spontaneous LES relaxation not triggered by swallowing
- Hypotensive LES (resting pressure <6 mmHg) - allows free reflux
2. Diaphragmatic Crura (External LES)
- Acts as an extrinsic sphincter reinforcing the LES
- Disrupted by hiatal hernia - when the stomach slides into the thoracic cavity, the LES moves above the diaphragm and loses the external support
3. Angle of His
- The acute angle between esophagus and gastric fundus creates a flap valve
- Lost in large hiatal hernias
4. Esophageal Acid Clearance
- Peristalsis clears refluxed material
- Salivary bicarbonate neutralizes residual acid
- Impaired in esophageal dysmotility
- Reduced during sleep (no swallowing, less saliva)
5. Gastric Factors
- Delayed gastric emptying increases gastric volume and pressure
- Increased gastric acid production (e.g., Zollinger-Ellison syndrome)
- Obesity increases intra-abdominal pressure, overwhelming the LES
(Fischer's Mastery of Surgery, 8th Edition; Sleisenger and Fordtran's)
Risk Factors for GERD
| Category | Factors |
|---|---|
| Anatomical | Hiatal hernia, short intra-abdominal esophageal length |
| Lifestyle | Obesity (OR 1.73), high-fat diet, alcohol, smoking, caffeine |
| Medications | Calcium channel blockers, anticholinergics, theophylline, nitrates (all reduce LES tone) |
| Hormonal | Pregnancy (progesterone relaxes LES); estrogen in obesity |
| Dietary | Chocolate, peppermint, fatty foods, citrus, tomato-based foods |
| Positional | Supine position, nocturnal reflux |
| H. pylori | Decreasing H. pylori prevalence partly explains rising GERD incidence |
Central obesity is more important than BMI - visceral fat produces IL-6 and TNF-α, which modulate LES pressure and contribute to insulin resistance. (Sleisenger and Fordtran's)
Clinical Features
Typical (esophageal) symptoms:
- Heartburn - burning retrosternal discomfort, worse postprandially, bending forward, or lying down
- Regurgitation - effortless return of gastric contents into the mouth or pharynx
- Water brash - hypersalivation as a reflex response to esophageal acid
Atypical (extraesophageal) symptoms:
- Respiratory: Chronic cough, asthma (worsening), recurrent pneumonia (micro-aspiration), laryngitis
- ENT: Hoarseness, sore throat, sinusitis, otitis media
- Dental: Enamel erosion (especially palatal surfaces of maxillary teeth), temperature sensitivity
- Chest pain (non-cardiac): Can mimic angina
(Sleisenger and Fordtran's; Cummings Otolaryngology)
Diagnosis
| Investigation | Role |
|---|---|
| Clinical diagnosis / Empirical PPI trial | 4-8 weeks PPI trial; symptomatic relief = diagnostic |
| Upper GI endoscopy (OGD) | Detects esophagitis, Barrett's, peptic stricture; can biopsy |
| 24-hour pH monitoring | Gold standard - measures esophageal acid exposure time |
| Impedance-pH monitoring | Detects both acid and non-acid reflux |
| High-resolution manometry | Assesses LES pressure, esophageal motility, hiatal hernia |
| Barium swallow | Can show hiatal hernia, strictures |
Complications
- Erosive esophagitis - mucosal damage graded by Los Angeles classification (A-D)
- Peptic esophageal stricture - from repeated mucosal injury and healing
- Barrett's esophagus - intestinal metaplasia of esophageal squamous epithelium; pre-malignant
- Esophageal adenocarcinoma - complication of long-standing Barrett's (OR 2.45 in obese)
- Hemorrhage and ulceration (rare but serious)
Treatment
Step 1 - Lifestyle modifications:
- Weight loss (BMI reduction of ≥3.5 kg/m² increases odds of symptom resolution 1.5-2.4 fold)
- Elevate head of bed 15-20 cm
- Avoid late meals, alcohol, smoking, trigger foods
- Small frequent meals
Step 2 - Medical therapy:
| Drug Class | Mechanism | Example |
|---|---|---|
| Proton Pump Inhibitors (PPIs) | Irreversibly block H⁺-K⁺ ATPase - final common pathway | Omeprazole, Pantoprazole |
| H₂ Receptor Antagonists | Block histamine (H₂) receptor on parietal cell | Ranitidine, Famotidine |
| Antacids | Neutralize luminal acid | Aluminium/Magnesium hydroxide |
| Prokinetics | Improve LES tone and gastric emptying | Metoclopramide, Domperidone |
PPIs are the most effective - they act on the final common pathway (H⁺-K⁺ ATPase) and achieve acid suppression regardless of the stimulus (histamine, gastrin, or ACh).
Step 3 - Surgical therapy:
- Laparoscopic Nissen fundoplication - gold standard surgical treatment; the gastric fundus is wrapped around the lower esophagus to recreate the LES
- Indicated when medical therapy fails, patient preference, or complications
- LINX device - magnetic sphincter augmentation (newer endoscopic option)
Summary Diagram - Key Relationships
Food/vagal → G cells → Gastrin → ECL cells → Histamine → Parietal cell H⁺-K⁺ ATPase → HCl
↑
ACh (vagal, M₃ receptor)
↑
Negative feedback: somatostatin, secretin
GERD = failure of antireflux barrier:
LES dysfunction + Hiatal hernia + ↑ gastric pressure → reflux → esophageal mucosal injury
Sources: Guyton and Hall Textbook of Medical Physiology | Bailey and Love's Short Practice of Surgery, 28th Ed | Sleisenger and Fordtran's Gastrointestinal and Liver Disease | Fischer's Mastery of Surgery, 8th Ed
Important point about dietary fibres for 3m
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I have all the material needed. Here is the focused 3-mark answer on dietary fibres:
Dietary Fibres - Important Points
Definition
Dietary fibre is "the remnants of the edible part of plants and analogous carbohydrates that are resistant to digestion and absorption in the human small intestine, with complete or partial fermentation in the human large intestine."
It includes polysaccharides, oligosaccharides, lignin, and associated plant substances. Animal foods contain no dietary fibre.
(Park's Textbook of Preventive and Social Medicine)
Types
| Type | Examples | Properties |
|---|---|---|
| Soluble fibre | Pectin, gums, mucilages, some hemicellulose | Dissolves in water, forms gel, slows absorption |
| Insoluble fibre | Cellulose, lignin, most hemicellulose | Does not dissolve, adds bulk, speeds transit |
Both types are essential for health promotion. The main chemical forms are complex polysaccharides: cellulose, hemicellulose, pectin, gums, and mucilages.
Key Functions and Health Effects
1. Laxation / GI effects
- Adds bulk to faeces, softens stool
- Increases frequency and regularity of bowel movements
- Increases gut transit time - prevents constipation
- Active substrate in the large intestine for fermentation by intestinal microbes, producing butyric acid and other short-chain fatty acids
2. Cardiovascular protection
- Binds bile salts in the gut and prevents their reabsorption
- This forces the liver to use more cholesterol to make new bile salts, thereby reducing blood cholesterol levels
- Associated with reduced incidence of coronary heart disease
3. Blood glucose control (Glycaemic Index)
- Soluble fibre (especially pectin and gums) slows release and absorption of sugar from the small intestine
- Reduces post-prandial blood glucose peaks
- Foods rich in fibre are classified as low glycaemic index (GI ≤55) foods - useful in diabetes and obesity management
- Fenugreek gum (40% gum content) is particularly effective in reducing blood glucose and cholesterol
4. Cancer prevention
- Inverse relationship between dietary fibre intake and colon cancer risk
- Mechanism: dilutes intestinal carcinogens, reduces exposure time of mucosa to carcinogens (faster transit), and alters colonic microbiota
5. Gut microbiome (Prebiotic effect)
- Fermentation by intestinal microbes changes the microbial colonization pattern of the colon
- Supports growth of probiotic bacteria
Recommended Intake & Cautions
- Recommended: ~30 g/day per 2000 kcal diet
- Excess (>60 g/day): Can reduce absorption of micronutrients (calcium, magnesium, iron, zinc) and cause bowel irritation
- Modern Western/refined diets are significantly deficient in fibre - a major public health concern
Disease Associations of Fibre Deficiency
| Disease | Link to Low Fibre |
|---|---|
| Constipation | Reduced stool bulk and slow transit |
| Diverticular disease | Refined diet deficient in fibre → increased intraluminal pressure in sigmoid colon |
| Coronary heart disease | Elevated cholesterol due to less bile salt binding |
| Type 2 diabetes | Poor glycaemic control |
| Colon cancer | Increased carcinogen exposure |
| Obesity | Low satiety, high caloric density |
(Park's Textbook of Preventive and Social Medicine; Bailey and Love's Short Practice of Surgery, 28th Ed)
This is a shared conversation. Sign in to Orris to start your own chat.