Infarct ?
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a complete overview of Infarct from Robbins & Kumar Basic Pathology:
Infarct
An infarct is an area of ischemic necrosis caused by occlusion of either the arterial supply or, less commonly, the venous drainage of a tissue.
Classification
Infarcts are classified by two criteria:
1. Color (amount of hemorrhage)
| Type | Also called | Mechanism | Where it occurs |
|---|---|---|---|
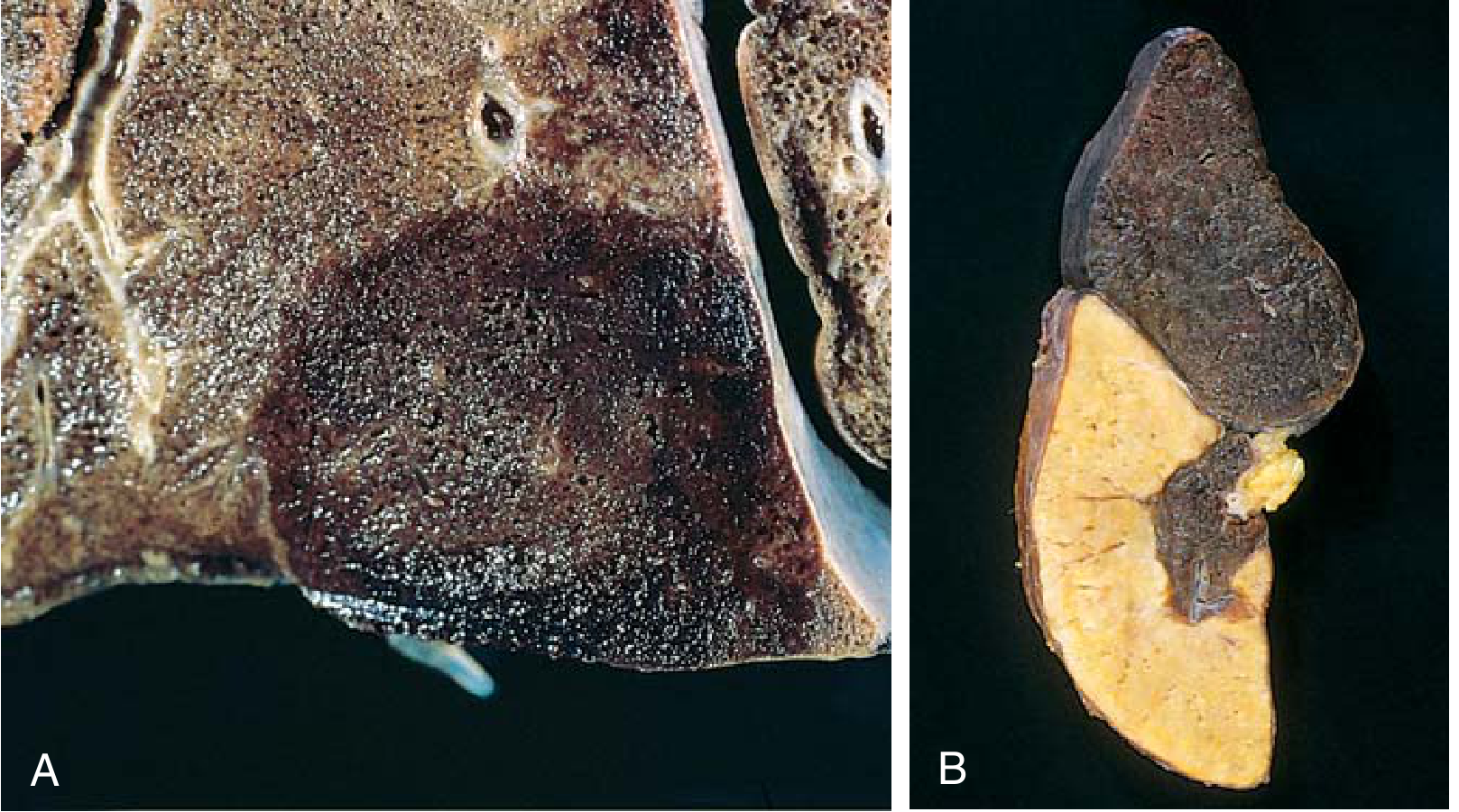
| Red (hemorrhagic) | Hemorrhagic infarct | Blood seeps into necrotic tissue | Venous occlusions (e.g., testicular torsion); tissues with dual circulation (lung, small intestine); previously congested tissues; after reperfusion of an arterial obstruction |
| White (anemic) | Pale infarct | No hemorrhage because end-arterial supply | Solid organs with end-arterial circulations - heart, spleen, kidney |
2. Presence of infection
- Bland infarct - no infection
- Septic infarct - infected cardiac valve vegetations embolize to tissue, converting the infarct into an abscess
Gross Morphology
- Infarcts tend to be wedge-shaped, with the occluded vessel at the apex and the organ periphery at the base
- When the base is a serosal surface, a fibrinous exudate forms over it
- Acute infarcts have indistinct, slightly hemorrhagic margins; over time, edges become better defined by a rim of hyperemia from inflammation
- White infarcts become progressively paler and sharper with time
- Hemorrhagic infarcts leave a firm, brown residue as extravasated RBCs are phagocytosed and heme is converted to hemosiderin
Histology
- The main finding is ischemic coagulative necrosis
- Exception: the brain undergoes liquefactive necrosis
- Inflammatory response begins at the margins within a few hours, well defined by 1-2 days
- Inflammation is followed by repair - parenchymal regeneration at periphery (if stromal architecture is spared), or replacement by scar
Factors That Influence Infarct Development
Three key variables determine whether vascular occlusion leads to infarction:
1. Anatomy of the vascular supply
The most important factor. Dual blood supply protects against infarction:
- Lung (pulmonary + bronchial arteries) - resistant, unless both are compromised
- Liver (hepatic artery + portal vein) - resistant
- Hand/forearm (radial + ulnar arteries) - resistant
- Kidney and spleen have end-arterial circulations - very susceptible
2. Rate of occlusion
- Slowly developing occlusions allow time for collateral vessel development - may prevent infarction even with complete occlusion (e.g., gradual coronary atherosclerosis allows interarteriolar anastomoses to enlarge)
- Sudden occlusion - no time for collaterals - infarction likely
3. Tissue vulnerability to hypoxia
| Cell type | Time to irreversible damage |
|---|---|
| Neurons | 3-4 minutes |
| Myocardial cells | 20-30 minutes |
| Fibroblasts | Many hours |
Common Sites and Clinical Examples
| Site | Type | Cause |
|---|---|---|
| Lung | Red (hemorrhagic) | Pulmonary embolism (especially with compromised bronchial supply) |
| Spleen | White (anemic) | Arterial embolism |
| Kidney | White (anemic) | Arterial embolism |
| Heart | White (anemic) - becomes scar | Coronary artery occlusion (atherosclerosis, thrombosis) |
| Brain | White - liquefactive | Arterial occlusion (stroke) |
| Testis | Red | Venous occlusion (torsion) |
| Small intestine | Red | Mesenteric venous thrombosis or dual arterial supply compromise |
Remote/Healed Infarct
- Ultimately replaced by fibrous scar
- Once completely healed, it is impossible to distinguish its age - an 8-week-old scar looks the same as a 10-year-old scar
Source: Robbins & Kumar Basic Pathology, Chapter 3 (Hemodynamic Disorders, Thromboembolism, and Shock)
Symptoms ?
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Since the previous question was about infarct in general (pathology), "Symptoms?" likely continues that context. Here is a full organ-by-organ breakdown from the textbooks:
Symptoms of Infarction (by site)
Symptoms depend entirely on the organ affected. There are no universal symptoms - each site produces a distinct clinical picture.
1. Myocardial Infarction (Heart)
Source: Frameworks for Internal Medicine
- Chest discomfort - pressure, tightness, squeezing; may radiate to the upper extremity, jaw (mandibular), or epigastrium
- Diaphoresis (sweating)
- Nausea / vomiting
- Syncope
- Dyspnea (shortness of breath) - an "angina equivalent"
- Fatigue
- Symptoms typically last >20 minutes and may occur at rest
- Atypical presentations are common in women, diabetics, and postoperative patients - these groups may have only dyspnea or fatigue with no chest pain
2. Pulmonary Infarction (Lung)
Source: Rosen's Emergency Medicine; Braunwald's Heart Disease
- Dyspnea - the most common symptom (75-80% of patients); may be sudden or gradual
- Pleuritic chest pain - sharp, severe, worsens with deep breathing; present in ~20% of PE cases and typically indicates peripheral infarction
- Hemoptysis - coughing up blood (minority of cases)
- Cough
- Low-grade fever (temperature >38.6°C / 101.5°F suggests infection rather than infarction)
- Tachycardia - the most common vital sign abnormality
- Unilateral leg swelling (if underlying DVT is the source)
- Syncope (rare, <5%, but when unexplained should raise suspicion)
- Severe cases: cardiovascular collapse, cardiac arrest (pulseless electrical activity)
Note: Pulmonary infarction symptoms can resemble lobar pneumonia (pleuritic pain + cough + fever). Distinguishing features: PE fever is low-grade, and productive cough for days suggests pneumonia.
3. Cerebral Infarction (Stroke)
- Sudden hemiplegia or hemiparesis (one-sided weakness)
- Aphasia (speech difficulty)
- Facial droop
- Visual disturbances (hemianopia, diplopia)
- Dysarthria (slurred speech)
- Ataxia (loss of coordination)
- Sudden confusion or altered consciousness
- A "stroke in evolution" = progressive worsening of neurological signs
4. Renal Infarction (Kidney)
- Flank pain (sudden onset)
- Hematuria (blood in urine)
- Fever
- Nausea/vomiting
- May be asymptomatic if small
5. Splenic Infarction
- Left upper quadrant pain, often radiating to the left shoulder
- Fever
- May be asymptomatic (discovered incidentally)
6. Mesenteric (Intestinal) Infarction
- Severe, diffuse abdominal pain - "pain out of proportion to physical findings" is a classic warning sign
- Nausea / vomiting
- Bloody diarrhea
- Abdominal distension
- Signs of peritonitis (guarding, rigidity) if bowel necrosis/perforation occurs
- Can progress to septic shock
7. Testicular Infarction (Torsion)
- Sudden, severe scrotal pain
- Scrotal swelling and tenderness
- Nausea / vomiting
- Absent cremasteric reflex
Summary Table
| Site | Key Symptoms |
|---|---|
| Heart | Chest pain radiating to arm/jaw, diaphoresis, nausea, dyspnea |
| Lung | Dyspnea, pleuritic chest pain, hemoptysis, low-grade fever |
| Brain | Sudden hemiplegia, aphasia, facial droop, confusion |
| Kidney | Flank pain, hematuria, fever |
| Spleen | Left upper quadrant pain, fever |
| Intestine | Severe abdominal pain out of proportion, bloody diarrhea |
| Testis | Sudden scrotal pain, swelling, absent cremasteric reflex |
The faster the occlusion and the more vulnerable the tissue (neurons > myocytes > fibroblasts), the more sudden and severe the symptoms.
This is a shared conversation. Sign in to Orris to start your own chat.