Management of parapharyngeal abscess
Reading File
Finding Sources
Finding Sources
Searching PubMed
parapharyngeal abscess management treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the complete answer.
Management of Parapharyngeal Abscess
Anatomy and Significance
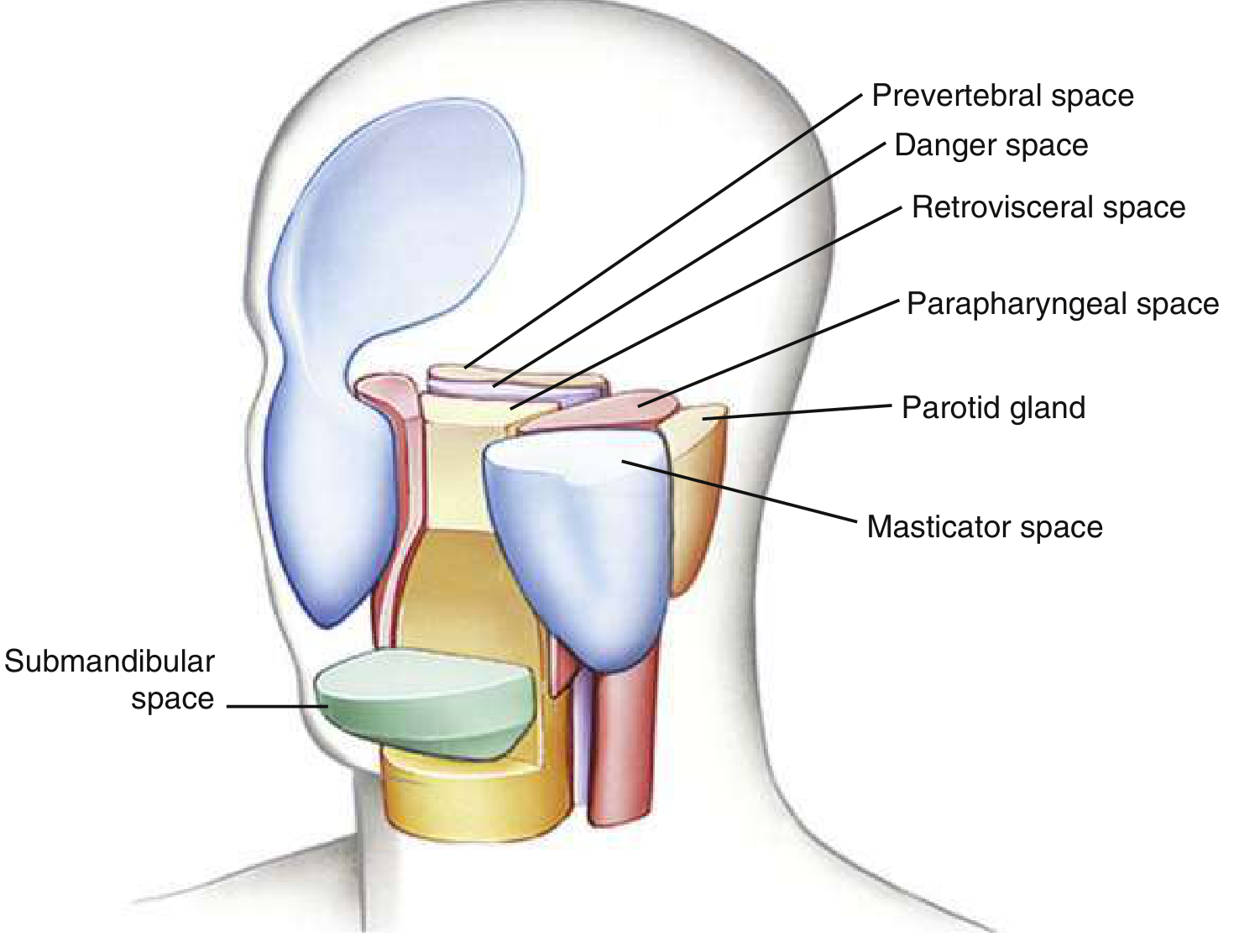
The parapharyngeal space (PPS) lies on either side of the neck, extending from the skull base to the styloglossus muscle at the angle of the mandible. It has two important sub-compartments:
- Anterior PPS (prestyloid): Contains fat - prone to liquefaction and abscess formation; requires aggressive surgical drainage
- Posterior PPS (poststyloid/retrostyloid): Contains the carotid sheath (carotid artery, internal jugular vein, sympathetic chain, CN IX-XII), lymph nodes; more often causes lymphadenitis and may be managed more conservatively
The posterior aspect is separated from the retropharyngeal and "danger space" by a fascial plane, creating a direct pathway to the mediastinum.
- Scott-Brown's Otorhinolaryngology, p. 671
- Rosen's Emergency Medicine, p. 965
Aetiology and Microbiology
Common sources include:
- Peritonsillar or retropharyngeal abscess (direct spread)
- Dental infection / mandibular molar periapical abscess
- Suppurative cervical lymphadenitis
- Parotitis
- Penetrating trauma, nerve blocks, or surgical procedures (iatrogenic)
- IV drug abuse
Organisms are typically polymicrobial - gram-positive cocci (streptococci, staphylococci), gram-negative rods, and anaerobes (Fusobacterium, Bacteroides, Peptostreptococcus).
Clinical Features
| Feature | Details |
|---|---|
| Neck pain and swelling | Lateral neck mass, often obscured by SCM |
| Trismus | Involvement of pterygoid muscles - key distinguishing sign vs. peritonsillar abscess |
| Odynophagia / dysphagia | Edema and pharyngeal displacement |
| Torticollis | If SCM is involved |
| Fever and systemic sepsis | Tachycardia, rigors |
| Medial tonsillar displacement | In anterior compartment infections |
| Voice change / muffled voice | Pharyngeal edema |
| Airway compromise | Dyspnea, stridor, inability to manage secretions - emergency |
Note: Unlike peritonsillar abscess, the maximal swelling is behind the posterior faucial pillar with little or no oedema of the soft palate. - Bailey & Love's Surgery, p. 480
Complications (Life-threatening - must anticipate)
- Airway obstruction - edema, abscess mass effect
- Descending mediastinitis - via retropharyngeal/danger space communication (crude mortality up to 2%)
- Lemierre syndrome - septic thrombophlebitis of the internal jugular vein; suspect when sore throat + sepsis + multisystem involvement
- Carotid artery erosion, aneurysm, or rupture - any signs of bleeding warrant CT/MR angiography urgently
- Horner syndrome - sympathetic chain involvement (CN IX-XII neuropathies)
- Cavernous sinus thrombosis - proptosis, impaired EOM, pupillary changes
- Aspiration pneumonia / lung abscess / empyema - from abscess rupture into airway
- Retroperitoneal sepsis - rare but described
Investigations
Imaging is mandatory (unless airway is immediately at risk - secure airway first):
- Contrast-enhanced CT of neck + chest - gold standard; demonstrates rim-enhancing abscess, extent of infection, and any mediastinal involvement. Always include the mediastinum in the scan field. Cellulitis appears as fat stranding along fascial planes; abscesses show characteristic ring enhancement
- MRI - comparable to CT for delineating extent; useful when radiation is to be minimized
- Ultrasound - may assess whether abscess has sufficiently liquefied and can guide needle aspiration, but limited in deep spaces
- CT or MR angiography - when vascular complications suspected
- Orthopantomogram (OPG) - if dental origin suspected
- Fibreoptic nasendoscopy - assess upper aerodigestive tract and airway patency simultaneously (performed cautiously to avoid triggering gag reflex)
Scott-Brown's ORL, p. 671; Rosen's Emergency Medicine, p. 965
Management: Step-by-Step
Step 1 - Airway Assessment and Securing (Priority Zero)
This is the pre-eminent step before any other intervention.
- Assess for: dyspnea, tachypnea, stridor, inability to manage secretions, agitation, drooling
- Conventional laryngoscopy is often impossible due to trismus, reduced neck extension, laryngopharyngeal edema, and friable mucosa
- Do NOT paralyze before securing airway
- Preferred method: awake fibreoptic nasotracheal or orotracheal intubation with adequate topicalization
- Have emergency tracheostomy prepared and set up before commencing anaesthesia; pre-infiltrate with 2% lignocaine + 1:80,000 adrenaline at tracheostomy site
- Transfer to operating theatre with anaesthetic and surgical teams experienced in difficult airway management
- Supine positioning for CT is only safe once airway is deemed stable
Scott-Brown's ORL, p. 673; Rosen's Emergency Medicine, p. 965
Step 2 - Intravenous Antibiotics (Immediate, Do Not Delay for Cultures)
Start broad-spectrum empiric IV antibiotics without delay:
| Scenario | Regimen |
|---|---|
| Community-acquired (first-line) | Ampicillin-sulbactam 1.5-3.0 g IV every 6 hours |
| Penicillin allergy | Clindamycin 600-900 mg IV every 8 hours |
| Eikenella suspected (dental origin) | Add moxifloxacin 400 mg QD |
| MRSA suspected | Clindamycin + vancomycin 1 g IV every 12 hours |
| Immunocompromised / nosocomial | Piperacillin-tazobactam 3 g IV every 6 h OR imipenem-cilastatin 500 mg IV every 6 h |
| Necrotizing fasciitis | Ceftriaxone 2 g + clindamycin 600-900 mg + metronidazole 500 mg IV every 6 h |
| Actinomyces | Penicillin G 10-20 MU/day for 4 weeks, then oral penicillin V for 4-6 months |
- Alternatively: amoxicillin-clavulanate, or 2nd/3rd generation cephalosporins with metronidazole
- Review all antibiotic choices once culture and sensitivity results are available
- Note rising resistance: clindamycin 11-18%, erythromycin 14%, penicillins 7-8%
- In children under 2: clindamycin preferred as first line due to MRSA rates
KJ Lee's Essential Otolaryngology, p. 710; Scott-Brown's ORL, p. 671
Step 3 - Corticosteroids (Adjunctive)
- Dexamethasone 0.6 mg/kg IV/IM (maximum 10 mg) given with antibiotics
- Associated with decreased need for surgical drainage in select cases
- Reduces pharyngeal edema and systemic inflammation
Rosen's Emergency Medicine, p. 965
Step 4 - Surgical Drainage (Decision)
Indications for surgery:
- Confirmed abscess on CT with liquefaction
- Failure to respond to conservative treatment after 24-48 hours (persistent pyrexia, worsening pain)
- Airway compromise from the abscess
- Vascular complications
Conservative (non-surgical) management may be appropriate if:
- Intranodal abscess or phlegmon (cellulitis without pus collection)
- Abscess size <2.5 cm contained within a single neck space
- Most pediatric cases (especially posterior PPS / phlegmon)
- Patient is responding clinically to antibiotics within 24-48 hours
Approximately 80% of patients ultimately require surgical drainage, though this varies widely by center (range 10-100%). - Scott-Brown's ORL, p. 672
Step 5 - Surgical Approach Options
A. Transcervical (external) approach - standard for most parapharyngeal abscesses
- Incision anterior to SCM, dissecting along the great vessels
- Approach anterior and medial to the carotid sheath
- Curette abscess wall; break down loculations
- Insert drain (usually corrugated or suction drain)
B. Intraoral drainage - only if abscess clearly points into the oropharynx
- Blunt instrument drainage through the oropharynx (medial to the pterygomandibular raphe)
- Risk of inadequate drainage; limited visualization
C. Ultrasound-guided needle aspiration
-
Shown in a prospective RCT to reduce hospital stay from 5.2 to 3.1 days and reduce cost by 41%, with no difference in efficacy or complications
-
Better for microbiological sampling (increases anaerobe isolation)
-
Useful when abscess is superficially accessible
-
Scott-Brown's ORL, p. 672; Bailey & Love's Surgery, p. 480
Repeat imaging and/or surgical re-intervention is indicated if there is no improvement after 48-72 hours of therapy.
Step 6 - ICU Admission and Monitoring
- Admit to ICU if airway or vascular compromise is present
- Monitor for septic complications, mediastinal spread, vascular involvement
- Patients with stable airways may be admitted to a high-dependency floor bed
- IV fluid resuscitation; nutritional support (NG or parenteral if swallowing compromised)
- Serial clinical and radiological reassessment
Special Considerations
Tuberculosis / fungal infection: In immunosuppressed patients or endemic regions with insidious onset, consider TB. Seek infectious disease + ENT consultation. Dedicated cervical spine imaging if ligamentous/osseous destruction is suspected.
Lemierre syndrome: If sore throat followed by sepsis + multisystem involvement - antibiotics for 6 weeks (penicillin + metronidazole or co-amoxiclav). Consider anticoagulation if spreading thrombophlebitis. - Scott-Brown's ORL, p. 480
Children: The majority of cases; often younger children; posterior PPS infections (lymphadenitis) more common and frequently managed conservatively with antibiotics alone. Use clindamycin as first-line in children under 2.
Recent Evidence
A 2023 systematic review on deep neck space infections (Sheikh Z et al., Clin Otolaryngol 2023) is the most current high-level evidence on assessment and management, supporting the multi-modal approach described above. A 2024 review (Wang X et al., PMID 38029535) specifically examined adjuvant corticosteroids in pediatric retropharyngeal and parapharyngeal abscess, supporting dexamethasone use to reduce the need for surgical drainage.
Summary Algorithm
Parapharyngeal Abscess
|
v
Airway Compromise? ──YES──> Awake fiberoptic intubation
| (+ prepare emergency tracheostomy)
NO
|
v
Contrast-enhanced CT Neck + Chest
|
_____|_____
| |
Cellulitis/ Abscess
Phlegmon confirmed
| |
IV Abx IV Abx + Dexamethasone
+ Dex + Otolaryngology consult
| |
Reassess Failure to respond ──> Surgical drainage
at 24-48h at 24-48 hours (transcervical / US-guided)
References:
- Rosen's Emergency Medicine - Concepts and Clinical Practice, pp. 964-966
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Vol 2), pp. 671-674
- Bailey & Love's Short Practice of Surgery (28th ed.), p. 480
- KJ Lee's Essential Otolaryngology, pp. 709-711
- Sheikh Z et al. (2023). Systematic review of deep neck space infections. Clin Otolaryngol. PMID 37147934
This is a shared conversation. Sign in to Orris to start your own chat.