COPD components
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive breakdown of the components of COPD, drawn from Robbins & Kumar Basic Pathology and Goldman-Cecil Medicine.
Components of COPD
COPD is an umbrella term that encompasses several distinct but overlapping patterns of lung injury, all resulting in persistent airflow limitation. The diagram below summarises their relationships:
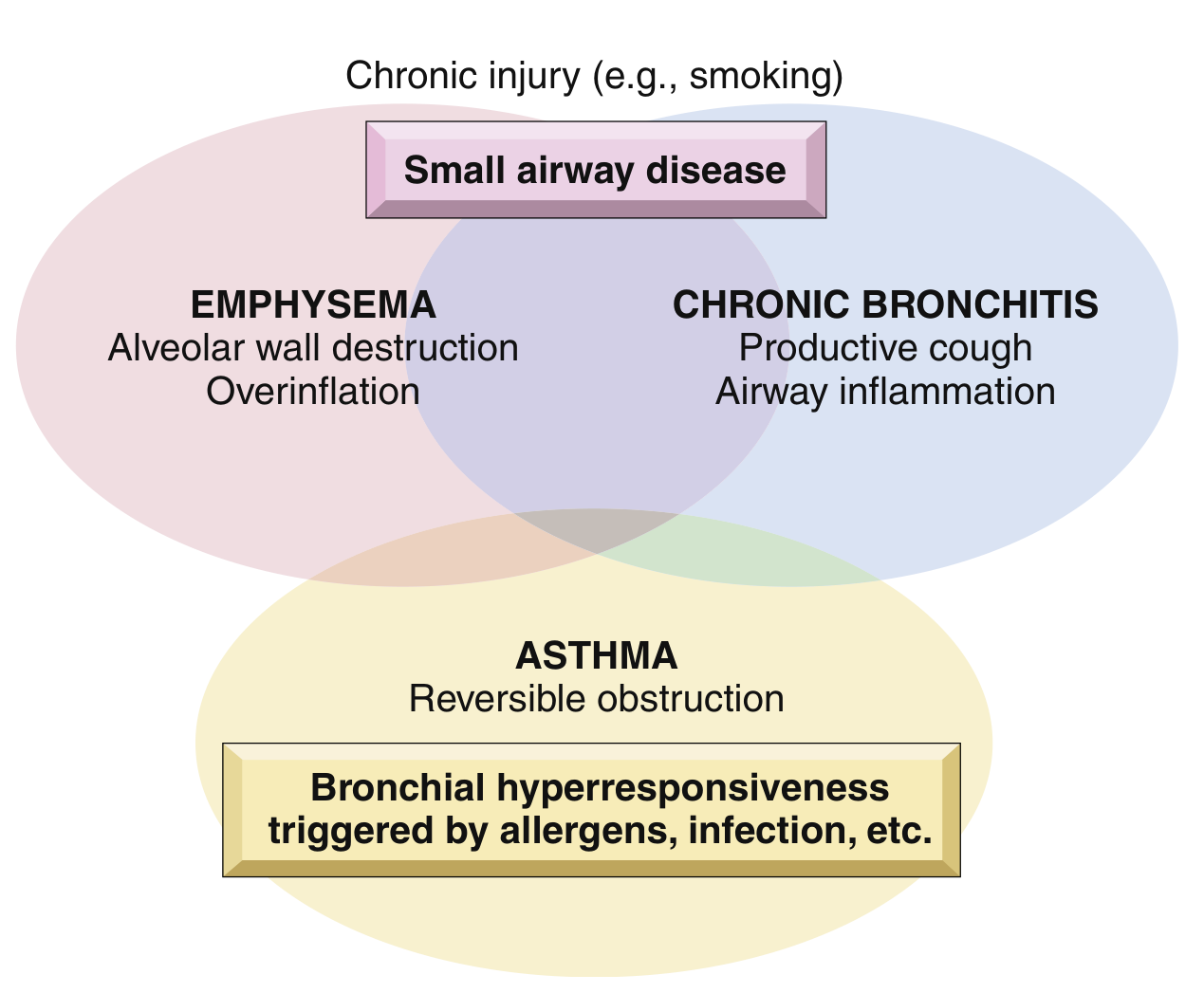
1. Emphysema
Definition: Permanent enlargement of air spaces distal to the terminal bronchioles, with destruction of alveolar walls, but without significant fibrosis.
Types (only first two cause COPD):
| Type | Distribution | Association |
|---|---|---|
| Centriacinar (centrilobular) | Central/proximal acinus; upper lobes | Cigarette smoking (~20x more common) |
| Panacinar (panlobular) | Entire acinus; lower lobes | Alpha-1 antitrypsin (AAT) deficiency |
| Distal acinar (paraseptal) | Peripheral acinus near pleura | Spontaneous pneumothorax in young adults |
| Irregular | Irregular; scar-related | Clinically insignificant |
Pathogenesis (three key mechanisms):
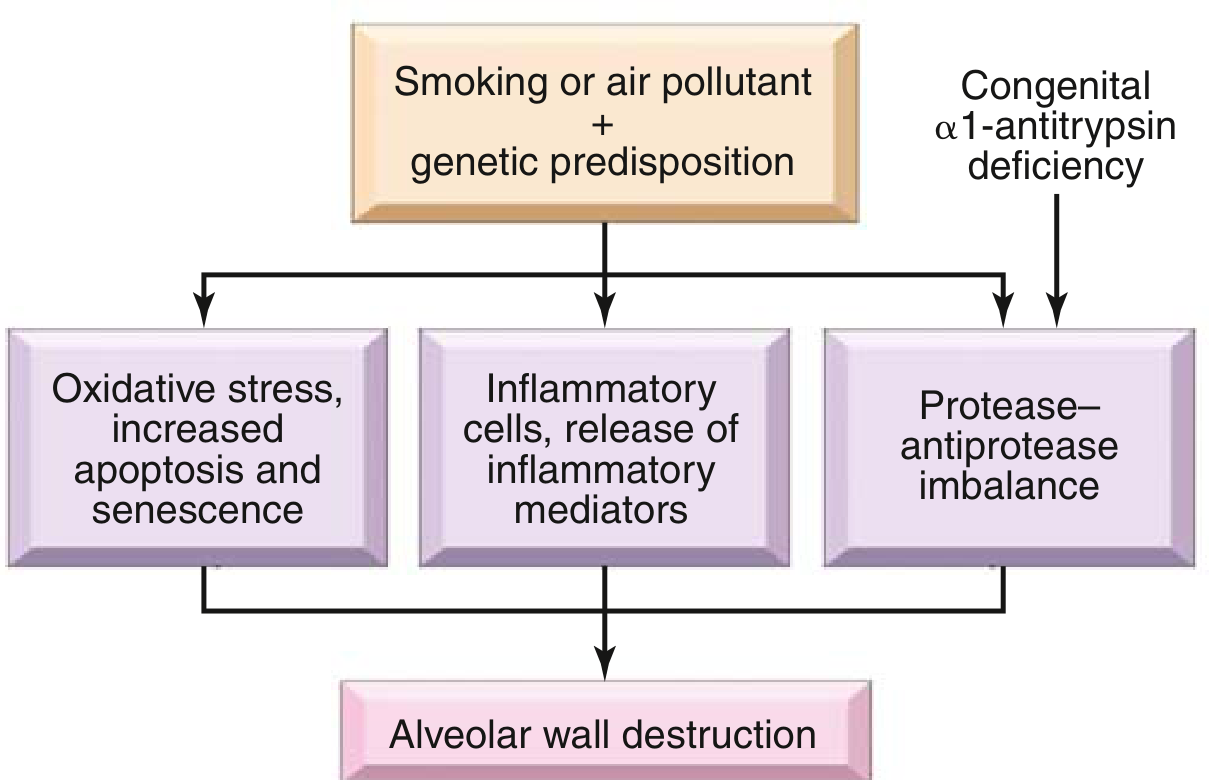
- Inflammatory cells and mediators - neutrophils, macrophages, CD4+/CD8+ T cells release LTB4, IL-8, TNF
- Protease-antiprotease imbalance - neutrophil elastase and other proteases degrade connective tissue; AAT deficiency amplifies this
- Oxidative stress - reactive oxygen species from smoke and macrophages cause direct tissue damage
Airflow obstruction mechanism: Loss of elastic tissue in alveolar walls reduces radial traction on small airways, causing respiratory bronchioles to collapse during expiration - functional obstruction without mechanical blockage.
2. Chronic Bronchitis
Definition: Persistent productive cough for at least 3 consecutive months in at least 2 consecutive years (clinical, not anatomical, definition).
Pathogenesis:
-
Irritants (especially cigarette smoke, SO2, NO2) cause:
- Hypertrophy of mucous glands in trachea/bronchi (Reid index >0.4)
- Goblet cell metaplasia in smaller bronchi and bronchioles
- Chronic inflammation - macrophages, neutrophils, lymphocytes (notably no eosinophils, unlike asthma)
-
IL-13 from T cells mediates mucin expression; neutrophil elastase is also upregulated
-
Microbial infection has a secondary role, mainly maintaining inflammation and worsening exacerbations
Airflow obstruction arises from small airway disease (chronic bronchiolitis): mucous plugging, inflammation, and submucosal fibrosis narrow bronchiolar lumens. In severe cases, complete obliteration occurs (bronchiolitis obliterans).
Reid index: ratio of submucosal gland layer thickness to total bronchial wall thickness; normally ≤0.4, elevated in chronic bronchitis.
3. Small Airway Disease (Chronic Bronchiolitis)
This is the primary site of airflow obstruction in COPD. It involves:
- Goblet cell metaplasia with mucus plugging of bronchiolar lumens
- Peribronchiolar inflammation
- Bronchiolar wall fibrosis and luminal narrowing
Small airways lack the cartilaginous support of larger airways and are more vulnerable to collapse and remodelling.
4. Pathological Inflammation
Underlying all components is a chronic inflammatory response throughout the airways and parenchyma, driven by:
- Cells: neutrophils, macrophages, CD8+ T lymphocytes (predominantly), B cells
- Mediators: LTB4, IL-8, TNF-alpha
- Pattern: distinct from asthma (eosinophil-rich); COPD inflammation is predominantly neutrophilic/macrophage-driven
The "Classic" Clinical Phenotypes
| Feature | "Pink Puffer" (Pure emphysema) | "Blue Bloater" (Chronic bronchitis dominant) |
|---|---|---|
| Build | Thin, barrel-chested | Obese/stocky |
| Cough/sputum | Minimal | Prominent, productive |
| Dyspnoea | Severe, at rest | Moderate |
| Blood gases | Near-normal (hyperventilates) | Hypoxaemia + hypercapnia |
| Cyanosis | Absent (until late) | Present |
| Cor pulmonale | Late | Earlier |
| Diffusion capacity | Low | Near-normal |
In practice, most patients have a mix of both components.
Airflow Obstruction - The Common Endpoint
Regardless of which component dominates, COPD is defined spirometrically as:
- FEV1/FVC < 0.7 (post-bronchodilator), largely irreversible
- Normal or near-normal FVC with reduced FEV1
GOLD staging classifies severity by % predicted FEV1 (GOLD 1-4).
Sources: Robbins & Kumar Basic Pathology, pp. 447-450; Goldman-Cecil Medicine, p. 890
Normal jvp
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Here is a complete breakdown of the normal JVP, sourced from Fuster & Hurst's The Heart and Harrison's Principles of Internal Medicine.
Normal JVP (Jugular Venous Pressure)
1. Normal Value and Measurement
The JVP reflects right atrial (central venous) pressure. It is measured as the vertical distance from the highest visible internal jugular venous pulsation to the angle of Louis (manubriosternal junction), which lies approximately 5 cm above the mid-right atrium regardless of patient position.
CVP = height above angle of Louis + 5 cm
| Position | Interpretation |
|---|---|
| At 45°, pulsation <3 cm above angle of Louis | Normal (<8 cmH₂O) |
| At 90° (sitting), no visible pulsation | Normal (<8 cmH₂O) |
| At 90°, pulsation at clavicle | ~10 cmH₂O |
| At 90°, pulsation at mid-neck | ~15 cmH₂O |
| At 90°, pulsation at angle of jaw | ~20 cmH₂O |
Note: cmH₂O ≠ mmHg (1.36 cmH₂O = 1 mmHg)
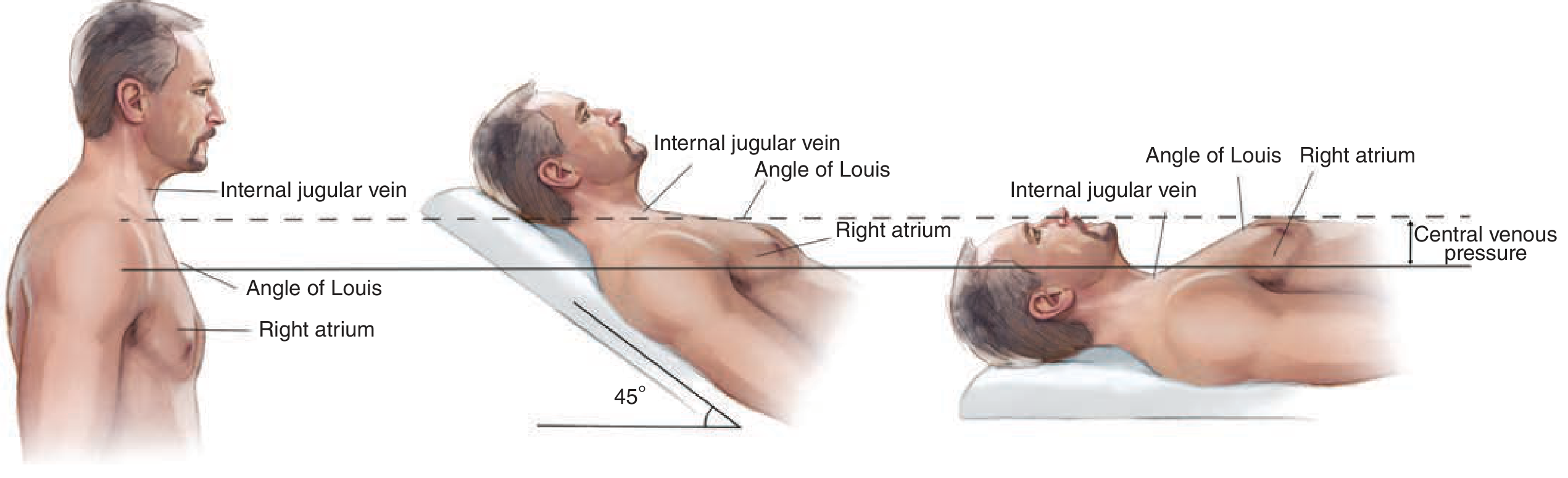
The internal jugular vein (not external) is used for assessment, as it more faithfully transmits right atrial pressure.
2. The Normal JVP Waveform
The normal venous contour has two upstrokes (a and v waves) and two downstrokes (x and y descents). A third small wave - the c wave - is seen on tracings but is rarely visible at the bedside.
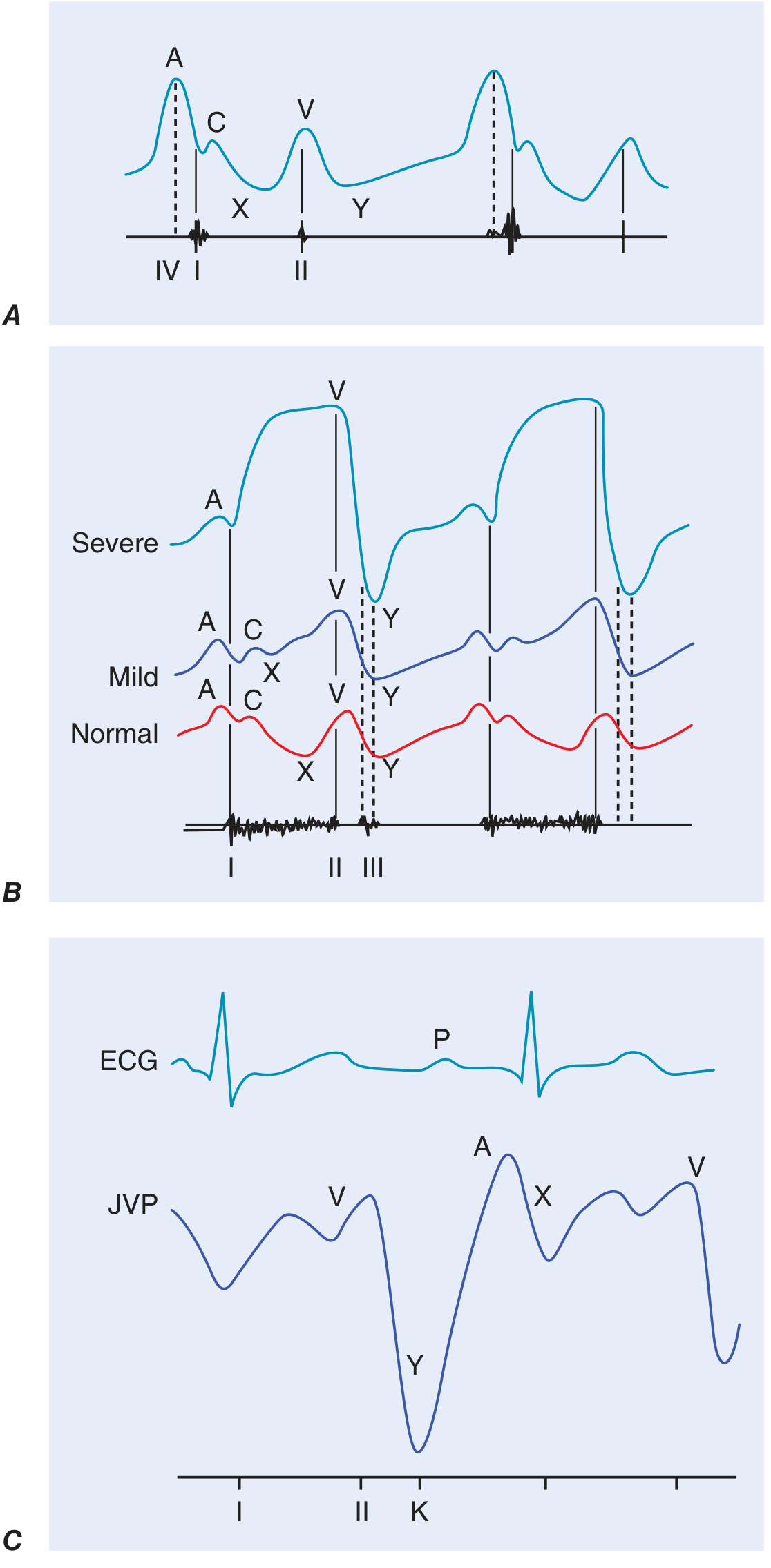
3. Components of the JVP Waveform
| Component | Timing | Mechanism | ECG Correlation |
|---|---|---|---|
| a wave | Pre-systole | Right atrial contraction | Just after P wave, before S1 |
| c wave | Early systole | Tricuspid valve bulging into RA during ventricular systole (or transmitted carotid pulsation) | After P wave |
| x descent | Systole | Atrial diastole + apical displacement of tricuspid annulus during ventricular contraction | During QRS-T |
| v wave | Late systole | Venous filling of RA while tricuspid is closed (atrial diastole) | Peaks at/after S2 |
| y descent | Early diastole | Tricuspid valve opens; RA empties into RV | After S2 |
Key normal feature: The a wave is larger than the v wave in normal persons.
4. How to Distinguish JVP from Carotid Pulse
| Feature | JVP | Carotid Pulse |
|---|---|---|
| Waveform | Biphasic (two upstrokes) | Monophasic |
| Compressibility | Obliterated by gentle pressure above clavicle | Cannot be compressed |
| Effect of posture | Changes (falls on sitting up) | No change |
| Effect of inspiration | Falls (normally) | No change |
| Palpable | No | Yes |
5. Normal Physiological Responses
- Inspiration: JVP normally falls by ≥3 mmHg within 15 seconds (negative intrathoracic pressure increases venous return to the right heart, reducing RA pressure)
- Kussmaul's sign: Failure of JVP to fall (or a rise) with inspiration - abnormal; seen in constrictive pericarditis, restrictive cardiomyopathy, RV infarction, massive PE
- Abdominojugular reflux: Normal JVP does not rise >3 cm with sustained abdominal compression; a positive test (sustained rise >3 cm) indicates volume overload
6. Abnormal Waveform Patterns (for comparison)
| Finding | Cause |
|---|---|
| Absent a wave | Atrial fibrillation |
| Prominent/large a wave | Reduced RV compliance, tricuspid stenosis, pulmonary hypertension |
| Cannon a wave | AV dissociation (RA contracts against closed tricuspid) |
| Large/dominant v wave | Tricuspid regurgitation ("ventricularzied" waveform) |
| Slow y descent | Tricuspid stenosis, cardiac tamponade |
| Rapid/deep y descent | Constrictive pericarditis (associated with pericardial knock) |
| Absent x descent | Atrial fibrillation, cardiac tamponade (x preserved, y absent) |
Sources: Fuster & Hurst's The Heart 15th Ed., pp. 84-85; Harrison's Principles of Internal Medicine 22E, p. 1904
This is a shared conversation. Sign in to Orris to start your own chat.