write a note on management of gout briefly ( 1 page)
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information to write the note. Let me compile it:
Management of Gout
Overview
Gout is a crystal deposition arthritis caused by monosodium urate (MSU) precipitation in joints and soft tissues, driven by sustained hyperuricemia. Management targets three goals: (1) relief of the acute attack, (2) prevention of recurrence, and (3) long-term lowering of serum urate.
1. Management of Acute Gouty Attack
NSAIDs (first-line)
Full-dose NSAIDs started as early as possible are the treatment of choice. Indomethacin (50 mg TID) is classical, but any NSAID at maximum therapeutic dose is effective. After 2 days at peak dose, taper over the next few weeks. Avoid in renal impairment, peptic ulcer disease, and in patients on anticoagulants.
Colchicine (second-line)
Colchicine inhibits neutrophil recruitment and NLRP3 inflammasome activation, reducing IL-1β release. It relieves most acute attacks within 6-12 hours. Low-dose regimen: 1.2 mg initially, then 0.6 mg 1 hour later (total 1.8 mg). High GI side effects (nausea, vomiting, diarrhea) limit its use. Contraindicated in significant hepatic or renal impairment. Interacts with CYP3A4 and P-glycoprotein inhibitors (e.g., clarithromycin, cyclosporine).
Corticosteroids (when NSAIDs/colchicine contraindicated)
- Oral: Prednisone 0.5 mg/kg/day, tapered by 5 mg/day
- Intra-articular: Triamcinolone 10-40 mg (large joints), 5-20 mg (small joints) - preferred for monoarticular attacks
- ACTH 40-80 mg IM/IV every 8-12 h can be used when all else fails
2. Prophylaxis of Recurrent Attacks
After the first attack resolves, low-dose colchicine (0.5-0.6 mg once or twice daily) or low-dose NSAIDs are used as bridging prophylaxis when initiating urate-lowering therapy (ULT), as starting ULT can precipitate a flare. Prophylaxis is continued for at least 3-6 months.
Lifestyle modification runs alongside pharmacotherapy: reduce alcohol (especially beer), avoid purine-rich foods (red meat, organ meats, shellfish), increase hydration, lose weight, and avoid fructose-containing beverages.
3. Urate-Lowering Therapy (ULT)
Indications: Two or more attacks per year, tophi, chronic gouty arthropathy, uric acid nephrolithiasis, or urate nephropathy.
Target serum uric acid: < 6 mg/dL (< 5 mg/dL in tophaceous gout).
Xanthine Oxidase Inhibitors (first-line ULT)
| Drug | Dose | Notes |
|---|---|---|
| Allopurinol | 100 mg/day initially; titrate to 300-800 mg/day | Adjust for renal function; risk of allopurinol hypersensitivity syndrome (AHS) - rare but severe (SJS/TEN); screen HLA-B*5801 in high-risk populations (Han Chinese, Korean, Thai) |
| Febuxostat | 40-80 mg/day | Non-purine analogue; preferred in allopurinol intolerance; caution in cardiovascular disease (higher CV mortality vs. allopurinol in CARES trial) |
Uricosuric Agents (second-line or add-on)
- Probenecid (500 mg BD, titrate to 1-2 g/day): blocks URAT-1 renal transporter; ineffective in renal impairment (GFR < 30); avoid in nephrolithiasis; maintain high fluid intake
- Benzbromarone: more potent uricosuric; available in some countries
Recombinant Uricases (refractory tophaceous gout)
- Pegloticase (IV infusion every 2 weeks): converts urate to allantoin; reserved for severe refractory gout; risk of infusion reactions and immunogenicity
- Rasburicase: used mainly for tumor lysis syndrome
4. Special Situations
- Transplant recipients / diuretic users: Losartan (uricosuric) and fenofibrate have off-label urate-lowering effects and can be chosen preferentially in relevant comorbidities
- Asymptomatic hyperuricemia: Treatment is generally NOT recommended due to cost and toxicity
- Renal impairment: Allopurinol dose must be adjusted; probenecid is ineffective; febuxostat may be used with caution
- Refractory / biologic therapy: Canakinumab (anti-IL-1β monoclonal antibody) is EMA-approved when conventional agents fail or are contraindicated; not FDA-approved for gout
Summary Algorithm
Acute attack
└─ NSAIDs (1st line) → Colchicine (2nd line) → Corticosteroids (3rd line)
After attack resolves + indications for ULT
└─ Start colchicine prophylaxis (0.5 mg BD)
└─ Initiate allopurinol (titrate to target uric acid < 6 mg/dL)
└─ Continue prophylaxis for 3-6 months
└─ Lifestyle modification throughout
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics; Textbook of Family Medicine 9e; Goldman-Cecil Medicine
drug profile on Semaglutide
Reading File
Finding Sources
Finding Sources
Searching PubMed
semaglutide cardiovascular outcomes obesity diabetes
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Excellent - I now have comprehensive information from multiple authoritative textbooks plus recent PubMed evidence. Let me compile the full drug profile:
Drug Profile: Semaglutide
1. Basic Classification
| Property | Detail |
|---|---|
| Drug class | Glucagon-like peptide-1 (GLP-1) receptor agonist |
| Type | Long-acting synthetic GLP-1 analog |
| Pronunciation | sem-a-GLOO-tide |
| Trade names | Ozempic (diabetes, SC), Rybelsus (diabetes, oral), Wegovy (obesity, SC) |
| FDA approvals | Type 2 diabetes mellitus; Chronic weight management (obesity); CV risk reduction in T2DM with established CVD |
2. Mechanism of Action
Semaglutide is a synthetic agonist at the GLP-1 receptor that is structurally modified to resist rapid enzymatic degradation (the major limitation of native GLP-1, which has a very short half-life). It acts via multiple complementary mechanisms:
- Glucose-dependent insulin secretion: Stimulates pancreatic beta cells to release insulin only in the presence of elevated glucose - minimal hypoglycemia risk as a monotherapy
- Glucagon suppression: Reduces postprandial glucagon secretion, limiting hepatic glucose output
- Gastric emptying delay: Slows gastric motility, blunting postprandial glucose spikes
- Satiety and appetite reduction: Acts on hypothalamic GLP-1 receptors and vagal afferents to enhance satiety signals and reduce hunger, leading to decreased caloric intake and weight loss
- Beta-cell proliferation: Promotes beta-cell growth and may preserve beta-cell mass
The incretin effect (oral glucose eliciting 60-70% more insulin than IV glucose) is markedly reduced in type 2 diabetes, and GLP-1 receptor agonists partially restore this physiological response.
3. Pharmacokinetics
| Parameter | SC Semaglutide | Oral Semaglutide |
|---|---|---|
| Route | Subcutaneous injection | Oral tablet |
| Dosing frequency | Once weekly | Once daily |
| Bioavailability | High (SC) | ~1% (enhanced with absorption enhancer SNAC) |
| Half-life | ~1 week | ~1 week |
| Protein binding | >99% (albumin) | |
| Metabolism | Proteolytic cleavage; no specific organ of elimination | Similar |
| Excretion | Urine and feces as metabolites | |
| Dose adjustment | No dose adjustment required for mild-moderate renal or hepatic impairment |
Oral semaglutide must be taken on an empty stomach with a small amount of plain water (up to 120 mL), and the patient must wait at least 30 minutes before eating or taking other medications - the absorption enhancer sodium N-(8-[2-hydroxybenzoyl]amino)caprylate (SNAC) facilitates gastric absorption.
4. Indications & Approved Doses
Type 2 Diabetes (Ozempic SC / Rybelsus oral)
- SC: Start 0.25 mg SC once weekly x 4 weeks → 0.5 mg once weekly; may increase to 1 mg or 2 mg based on glycemic response
- Oral: Start 3 mg once daily x 30 days → 7 mg once daily; may increase to 14 mg once daily
- Also reduces risk of major adverse cardiovascular events (MACE) in T2DM patients with established CVD
Obesity / Chronic Weight Management (Wegovy SC)
- Start 0.25 mg once weekly → titrate every 4 weeks: 0.5 → 1.0 → 1.7 → 2.4 mg once weekly (maintenance)
- Indicated for BMI ≥ 30 kg/m², or BMI ≥ 27 kg/m² with at least one weight-related comorbidity
Cardiovascular Risk Reduction (SELECT trial - without diabetes)
- 2.4 mg SC once weekly approved to reduce CV events in adults with obesity/overweight and established CVD but without T2DM
5. Clinical Efficacy
- HbA1c reduction: ~1.5-1.8% reduction (T2DM)
- Weight loss: 10-15% body weight reduction at 2.4 mg dose (STEP trials); up to 15-17% in STEP 1 trial
- Cardiovascular outcomes (SUSTAIN-6 trial): 26% relative risk reduction in MACE (CV death, non-fatal MI, non-fatal stroke) vs placebo in T2DM
- SELECT trial (2023): 20% reduction in MACE in obese/overweight patients without diabetes
- A 2025 systematic review and meta-analysis (PMID: 39396098) confirmed semaglutide's cardiovascular safety benefits in overweight/obese patients
6. Adverse Effects
Common (GI - most frequent, usually transient)
- Nausea, vomiting, diarrhea, constipation
- Occur mostly during dose escalation; tend to resolve over weeks
Serious / Clinically Important
| Adverse Effect | Notes |
|---|---|
| Pancreatitis | Rare; discontinue if suspected; contraindicated in history of pancreatitis |
| Gallbladder disease | Cholelithiasis, cholecystitis (rapid weight loss risk) |
| Thyroid C-cell tumors | Seen in rodents at high doses; risk in humans unknown; contraindicated in MEN2 or personal/family history of medullary thyroid carcinoma (MTC) |
| Diabetic retinopathy | Worsening reported with rapid HbA1c reduction (SUSTAIN-6); a 2025 meta-analysis (PMID: 40810985) highlighted ocular adverse events |
| Hypoglycemia | Low risk as monotherapy; risk increases with insulin or sulfonylurea combination |
| Acute kidney injury | Typically from dehydration secondary to severe GI effects |
| Tachycardia | Modest increase in resting heart rate (~2-4 bpm) |
| Suicidal ideation | Noted in prescribing information; monitor for mood changes |
7. Contraindications
- Personal or family history of medullary thyroid carcinoma (MTC)
- Multiple endocrine neoplasia type 2 (MEN2)
- History of serious hypersensitivity to semaglutide
- Pregnancy (discontinue at least 2 months before planned pregnancy)
- Chronic pancreatitis (relative contraindication)
8. Drug Interactions
| Interacting Drug | Mechanism | Clinical Significance |
|---|---|---|
| Insulin / sulfonylureas | Additive glucose lowering | Reduce insulin/SU dose; hypoglycemia risk |
| Oral medications | Delayed gastric emptying | Absorption of co-administered oral drugs may be slowed; separate timing of critical drugs (e.g., levothyroxine, oral contraceptives) |
| Warfarin | Delayed absorption of warfarin | Monitor INR closely when initiating or changing semaglutide dose |
9. Special Populations
| Population | Recommendation |
|---|---|
| Renal impairment | No dose adjustment needed; monitor for dehydration-related AKI |
| Hepatic impairment | Use with caution; limited data |
| Elderly | No dose adjustment required; greater caution for GI effects and dehydration |
| Pregnancy | Contraindicated; potential fetal harm |
| Breastfeeding | Not recommended; excretion in human milk unknown |
| Pediatrics | Ozempic approved ≥ 12 years for T2DM; Wegovy approved ≥ 12 years for obesity |
| Post-bariatric surgery | May provide additional weight loss benefit as adjuvant therapy |
10. Place in Therapy
Diabetes: After metformin (or as first-line in patients with established ASCVD, heart failure, or CKD per ADA guidelines). Preferred over DPP-4 inhibitors and SGLT2 inhibitors when weight loss is a priority.
Obesity: First-line pharmacotherapy for eligible patients (BMI ≥ 30 or ≥ 27 with comorbidities) alongside lifestyle modification. The most efficacious single-agent anti-obesity drug currently available.
Cardiovascular protection: Now indicated for CV risk reduction independent of glycemic control, representing a paradigm shift in its use beyond metabolic disease.
11. Monitoring Parameters
- HbA1c every 3 months (until stable, then every 6 months)
- Fasting blood glucose (self-monitoring)
- Body weight and BMI
- Renal function (especially if GI side effects are severe)
- Thyroid examination / calcitonin if clinically indicated
- Signs/symptoms of pancreatitis
- Ophthalmology review in diabetic patients at baseline and after rapid HbA1c drops
Sources: Lippincott Illustrated Reviews Pharmacology; Katzung's Basic & Clinical Pharmacology 16e; Goldman-Cecil Medicine; Neuroscience: Exploring the Brain 5e. Recent evidence: PMID 39396098 (Syst. Rev., Int J Obes 2025); PMID 40810985 (Meta-Analysis, JAMA Ophthalmol 2025)
note on leukemoid reaction briefly
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Excellent - I have comprehensive content from Henry's Clinical Diagnosis, Goldman-Cecil Medicine, and the peripheral blood smear image. Here is the complete note:
Leukemoid Reaction
Definition
A leukemoid reaction is an excessive leukocytic response in the peripheral blood that mimics leukemia morphologically but is due to a benign reactive cause. It is defined as a white blood cell count ≥ 50 × 10⁹/L (50,000/μL) with a pronounced left shift - the appearance of immature precursor cells in the peripheral circulation.
Peripheral Blood Smear
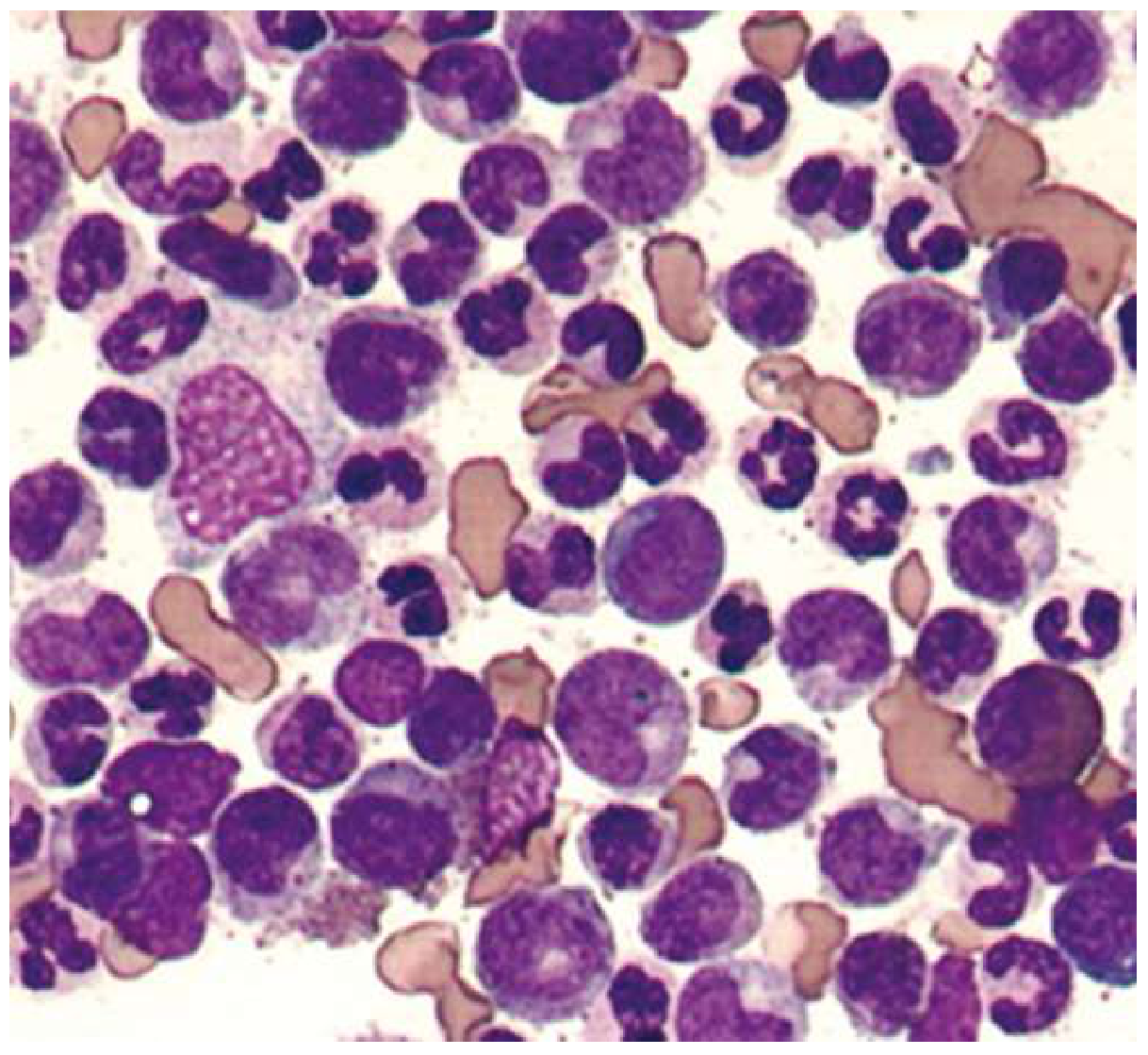
Peripheral blood smear of a leukemoid reaction - morphologically indistinguishable from CML; distinction requires BCR-ABL testing (Goldman-Cecil Medicine)
Types
Leukemoid reactions are classified by the predominant cell type:
| Type | Predominant Cell | Common Causes |
|---|---|---|
| Neutrophilic (most common) | Mature + immature neutrophils | Sepsis (TB, C. difficile), burns, hemorrhage, hemolysis, malignancy with bone marrow involvement, Hodgkin lymphoma, eclampsia, toxins |
| Lymphocytic | Lymphocytes | Infectious lymphocytosis, pertussis (whooping cough), infectious mononucleosis |
| Eosinophilic | Eosinophils | Parasitic infections (common in children) |
| Monocytic | Monocytes | Chronic infections, collagen vascular disease |
Pathophysiology
In response to severe physiological stress - infection, inflammation, tissue necrosis, malignancy, or toxins - massive cytokine release (G-CSF, GM-CSF, IL-1, IL-6, TNF-α) drives extreme marrow stimulation. The marrow releases not just mature neutrophils but also immature precursors (bands, metamyelocytes, myelocytes) into the circulation, producing the "left shift."
Blood Film Features (Neutrophilic Type)
- Leukocytosis > 50 × 10⁹/L
- Pronounced left shift: bands, metamyelocytes, myelocytes in circulation
- Toxic granulation (dark, coarse cytoplasmic granules in neutrophils)
- Döhle bodies (pale blue cytoplasmic inclusions)
- Cytoplasmic vacuoles in neutrophils
- No basophilia or eosinophilia (contrast with CML)
- No anemia or thrombocytosis as a primary finding
Leukemoid Reaction vs. CML - Key Differences
| Feature | Leukemoid Reaction | CML |
|---|---|---|
| Cause | Reactive (infection, malignancy, etc.) | Clonal myeloproliferative neoplasm |
| WBC | Often > 50 × 10⁹/L | Often > 100 × 10⁹/L |
| Left shift | Present (bands, metas, myelocytes) | Present - "myelocyte peak" characteristic |
| Basophilia | Absent | Present (hallmark feature) |
| Eosinophilia | Absent | Present |
| Panmyelosis | Absent | Present (all cell lines increased) |
| Toxic granulation / Döhle bodies | Present | Absent |
| NAP/LAP score | Normal or elevated | Decreased (key distinguishing test) |
| BCR-ABL | Negative | Positive (diagnostic) |
| Philadelphia chromosome | Absent | Present (t(9;22)) |
| Splenomegaly | Absent or mild | Common, often massive |
| Bone marrow | Reactive hyperplasia only | Hypercellular with all myeloid series |
NAP = Neutrophil Alkaline Phosphatase - the single most important bedside differentiating test before BCR-ABL is sent.
Leukoerythroblastic Reaction
A special variant where circulating normoblasts (nucleated red cells) accompany a neutrophilic leukemoid reaction. This "leukoerythroblastic picture" is seen in:
- Metastatic carcinoma infiltrating bone marrow
- Myelofibrosis
- Marrow infection or granulomatous disease
- Benign conditions: severe GI bleeding, hemolytic anemia
Diagnosis Workup
- Clinical history - look for identifiable cause (infection, malignancy, drugs, burns)
- Peripheral smear - toxic changes confirm reactive nature
- NAP/LAP score - elevated = leukemoid reaction; reduced = CML
- CRP / ESR / Procalcitonin - elevated in reactive states
- BCR-ABL by PCR or FISH - definitive exclusion of CML
- Bone marrow biopsy - if no cause identified, to exclude myeloproliferative disease, infiltration, or fibrosis
- Specific investigations based on suspected cause (blood cultures, TB workup, tumor markers, etc.)
Management
Leukemoid reaction itself requires no specific treatment. Management is directed at the underlying cause:
- Severe infections - appropriate antimicrobial therapy
- Underlying malignancy - oncology referral
- Hemolysis/hemorrhage - treat the cause
- The leukocytosis resolves once the trigger is removed
Sources: Henry's Clinical Diagnosis and Management by Laboratory Methods; Goldman-Cecil Medicine International Edition; Textbook of Family Medicine 9e
drug profile on pembrolizumab
Finding Sources
Finding Sources
Searching PubMed
pembrolizumab cancer immunotherapy outcomes
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive information from authoritative sources. Here is the full drug profile:
Drug Profile: Pembrolizumab
1. Basic Classification
| Property | Detail |
|---|---|
| Drug class | Immune checkpoint inhibitor - anti-PD-1 monoclonal antibody |
| Type | Humanized monoclonal IgG4κ antibody |
| Former names | Lambrolizumab; MK-3475 |
| Trade name | Keytruda |
| Route | Intravenous infusion only |
| Developer | Merck; first FDA approval 2014 (melanoma) |
2. Mechanism of Action
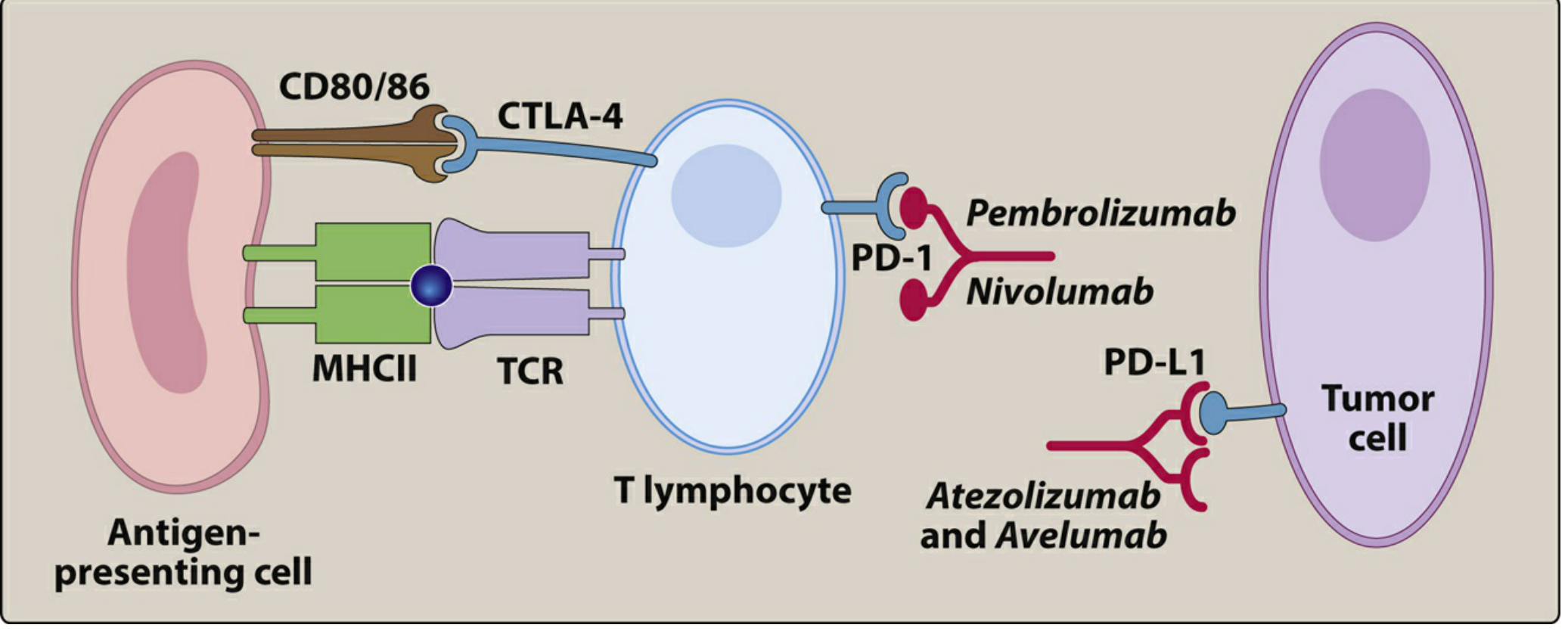
Fig: Pembrolizumab and nivolumab block PD-1 on T lymphocytes; atezolizumab/avelumab block PD-L1 on tumor cells; ipilimumab blocks CTLA-4 (Lippincott Illustrated Reviews Pharmacology)
Normal physiology: T-cell activation requires two signals - (1) TCR binding to MHC-peptide on an antigen-presenting cell, and (2) CD28 costimulatory binding to B7 proteins. After activation, T cells upregulate inhibitory receptors including PD-1 (Programmed Death-1) to prevent autoimmune collateral damage. Binding of PD-1 to its ligands PD-L1 or PD-L2 induces T-cell exhaustion and terminates the immune response.
Cancer exploitation: Tumor cells and tumor-infiltrating macrophages upregulate PD-L1, presenting it to tumor-infiltrating T cells to shield themselves from cytotoxic T-cell killing - an "immune escape" mechanism.
Pembrolizumab's action: It is a humanized antibody with a mouse variable region grafted onto a human IgG4 framework, showing high affinity for PD-1 on human and primate T cells. By blocking PD-1 from binding PD-L1/PD-L2, pembrolizumab:
- Restores and sustains T-cell antitumor cytotoxic activity
- Increases production of TNF-α, IFN-γ, and granzyme B
- Prevents T-cell exhaustion within the tumor microenvironment
- Allows immune-mediated eradication of cancer cells expressing tumor antigens
3. Pharmacokinetics
| Parameter | Detail |
|---|---|
| Administration | IV infusion over 30 minutes |
| Dosing | 200 mg every 3 weeks or 400 mg every 6 weeks (flat dosing); 2 mg/kg every 3 weeks in children |
| Elimination half-life | ~26 days |
| Metabolism | Proteolytic degradation (as with all large protein antibodies) - no hepatic CYP450 metabolism |
| Excretion | No specific organ of elimination |
| Protein binding | Binds PD-1 receptor; IgG4 does not efficiently activate complement |
| Drug interactions | No pharmacokinetic drug-drug interactions (not metabolized by CYP enzymes) |
4. FDA-Approved Indications
Pembrolizumab holds one of the broadest approval profiles of any oncology drug, currently approved for 18+ different cancers:
Solid Tumors
| Cancer Type | Setting | Biomarker Requirement |
|---|---|---|
| Melanoma | Advanced/metastatic; adjuvant (stage IIB/IIC/III/IV resected) | None required |
| NSCLC | First-line (monotherapy or + chemo); second-line post-platinum | PD-L1 TPS ≥1% for monotherapy; TPS ≥50% for 1st-line mono |
| Head & neck SCC | First-line (+ chemo) or monotherapy; recurrent/metastatic | CPS ≥1 for some indications |
| Urothelial carcinoma | First-line (cisplatin-ineligible); second-line post-platinum | PD-L1 for first-line |
| Triple-negative breast cancer | Neoadjuvant + adjuvant; locally advanced/metastatic | PD-L1 CPS ≥10 |
| Cervical cancer | Recurrent/metastatic + chemotherapy | PD-L1 CPS ≥1 |
| Endometrial carcinoma | Advanced/recurrent (+ lenvatinib) | MMR/MSI testing |
| Gastric/GEJ adenocarcinoma | First-line + chemo; second-line | PD-L1 CPS ≥1 |
| Hepatocellular carcinoma | Previously treated | None |
| Merkel cell carcinoma | Recurrent/metastatic | None |
| Renal cell carcinoma | First-line (+ axitinib or lenvatinib) | None |
| Colorectal cancer | MSI-H/dMMR, 1st-line | MSI-H or dMMR |
| Esophageal/GEJ | First-line + chemo; second-line | PD-L1 CPS ≥10 |
| TMB-High (≥10 mut/Mb) | Any solid tumor, unresectable/metastatic | TMB ≥10 mutations/megabase |
| MSI-H/dMMR | Any solid tumor (tissue-agnostic) | MSI-H or dMMR |
Hematologic
- Classical Hodgkin lymphoma - relapsed/refractory after ≥3 prior lines
- Primary mediastinal large B-cell lymphoma - relapsed/refractory
The tissue-agnostic approvals (MSI-H/dMMR and TMB-high) represent a landmark shift: pembrolizumab is the first drug approved based on a tumor's molecular profile rather than its anatomical origin.
5. Key Biomarkers for Patient Selection
| Biomarker | Test Method | Role |
|---|---|---|
| PD-L1 expression (CPS or TPS) | Immunohistochemistry | Predicts response in NSCLC, gastric, head & neck, cervical, TNBC |
| MSI-H (Microsatellite Instability-High) | PCR or NGS | Tissue-agnostic approval; strong predictor of response |
| dMMR (Mismatch Repair Deficient) | IHC for MLH1, MSH2, MSH6, PMS2 | Equivalent biomarker to MSI-H |
| TMB ≥10 mutations/Mb | Next-generation sequencing | Tissue-agnostic approval |
| BRAF mutation status | Molecular testing | Relevant for sequencing vs. targeted therapy in melanoma |
6. Adverse Effects
Pembrolizumab's adverse effects are caused by immune-related adverse events (irAEs) - uncontrolled autoreactivity resulting from PD-1 blockade. These are less frequent than with anti-CTLA-4 agents but can be severe and life-threatening.
Common (>20% of patients)
- Fatigue, nausea, decreased appetite, constipation
- Cough, dyspnea (in lung cancer patients)
- Pruritus, rash
- Arthralgia, musculoskeletal pain
- Diarrhea
Immune-Related Adverse Events (irAEs) - by organ
| System | Adverse Event | Severity |
|---|---|---|
| Pulmonary | Pneumonitis | Can be fatal; Grade 3-4 seen in ~3% |
| GI | Colitis, diarrhea | Common; risk of perforation if severe |
| Liver | Immune-mediated hepatitis | Monitor LFTs regularly |
| Endocrine | Hypothyroidism, hyperthyroidism, hypophysitis, adrenal insufficiency, type 1 DM | Often permanent (endocrinopathies) |
| Renal | Nephritis, renal dysfunction | Monitor creatinine |
| Neurological | Peripheral neuropathy, encephalitis, myasthenia gravis, Guillain-Barré | Rare but serious |
| Cardiac | Myocarditis (rare, but high mortality if missed) | Rare; check troponin if symptoms |
| Skin | Severe rash, Stevens-Johnson syndrome, toxic epidermal necrolysis | Rare |
| Musculoskeletal | Myositis, arthritis | Monitor CK and joint symptoms |
7. Management of irAEs
| Grade | Action |
|---|---|
| Grade 1 | Continue pembrolizumab; close monitoring; topical/symptomatic treatment |
| Grade 2 | Withhold pembrolizumab; start oral prednisolone 1-2 mg/kg/day; resume when grade ≤1 |
| Grade 3-4 | Permanently discontinue; IV methylprednisolone 1-2 mg/kg/day; consider infliximab for steroid-refractory colitis or hepatitis |
| Endocrinopathies | Usually require lifelong hormone replacement even after drug discontinuation |
8. Contraindications & Precautions
| Condition | Guidance |
|---|---|
| Active autoimmune disease | Relative contraindication; may exacerbate (e.g., SLE, IBD, RA) |
| Organ transplant recipients | Risk of rejection due to immune activation |
| Pregnancy | Contraindicated - IgG crosses placenta; potential fetal harm |
| Breastfeeding | Avoid during treatment and for 4 months after last dose |
| Active infections | Caution; immunostimulation may worsen certain infections |
| Prior severe irAEs | Carefully re-evaluate risk-benefit before re-challenge |
9. Special Considerations
Pseudo-progression: Tumor size may initially appear to increase on imaging due to immune cell infiltration before regression - evaluate with clinical response, not imaging alone. Use iRECIST criteria rather than standard RECIST.
Delayed and durable responses: Responses can appear weeks to months after initiation and may be durable even after discontinuation - some melanoma patients have had responses lasting > 10 years.
Combination strategies:
- + Chemotherapy: Standard in NSCLC, TNBC, gastric cancer, esophageal cancer
- + Ipilimumab (anti-CTLA-4): Synergistic; used in melanoma, NSCLC, RCC, MSI-H colorectal - but higher irAE rates
- + Targeted therapy: Pembrolizumab + lenvatinib (VEGFR inhibitor) in RCC and endometrial cancer
- + Antibody-drug conjugates: Emerging combinations in clinical trials
Immune checkpoint inhibitor class effects: Compared to anti-CTLA-4 agents (ipilimumab), PD-1 inhibitors like pembrolizumab have a more favorable safety profile with lower rates of severe irAEs, while maintaining high efficacy.
10. Monitoring Parameters
| Parameter | Frequency |
|---|---|
| LFTs (AST, ALT, bilirubin) | Before each dose |
| Thyroid function (TSH, free T4) | Every 3-6 months |
| Creatinine / renal function | Before each dose |
| Blood glucose | Periodically |
| CBC | Periodically |
| Chest imaging | As clinically indicated (monitor for pneumonitis) |
| Troponin | If cardiac symptoms arise |
| CK levels | If myositis suspected |
11. Recent Clinical Evidence
- A 2023 network meta-analysis (PMID: 37612624) confirmed pembrolizumab + chemotherapy significantly improves pathological complete response (pCR) in high-risk early-stage TNBC compared to chemo alone
- A 2024 systematic review (PMID: 38694505) in SCLC showed pembrolizumab combinations provide modest benefit with manageable toxicity in extensive-stage disease
- Tissue-agnostic expansion (TMB-high, MSI-H) continues to be validated across tumor types in real-world data
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics; Lippincott Illustrated Reviews Pharmacology; Washington Manual of Medical Therapeutics; Goldman-Cecil Medicine; Murray & Nadel's Respiratory Medicine
write briefly 1-2 pages
Based on the comprehensive information already retrieved in our previous conversation, here is the condensed 1-2 page drug profile:
Drug Profile: Pembrolizumab (Keytruda)
Basic Information
| Property | Detail |
|---|---|
| Class | Immune checkpoint inhibitor (anti-PD-1) |
| Type | Humanized monoclonal IgG4κ antibody |
| Route | IV infusion only |
| Trade name | Keytruda |
| Former name | Lambrolizumab / MK-3475 |
Mechanism of Action
Under normal physiology, activated T cells upregulate PD-1 (Programmed Death-1) receptors to prevent autoimmunity. Tumor cells exploit this by overexpressing PD-L1, which binds PD-1 on cytotoxic T cells, inducing T-cell exhaustion and immune escape.
Pembrolizumab is a humanized antibody (mouse variable region on a human IgG4 framework) that blocks PD-1 from binding PD-L1/PD-L2. This restores T-cell cytotoxic activity within the tumor microenvironment, increasing TNF-α, IFN-γ, and granzyme B production, enabling immune-mediated tumor destruction.
Pharmacokinetics
- Dose: 200 mg IV every 3 weeks or 400 mg IV every 6 weeks (30-min infusion)
- Half-life: ~26 days
- Metabolism: Proteolytic degradation - no CYP450 involvement, no pharmacokinetic drug interactions
- Elimination: No specific organ of clearance
Approved Indications
Pembrolizumab has one of the broadest approval profiles in oncology, covering 18+ cancers:
- Melanoma - advanced/metastatic; adjuvant (stage IIB-IV resected)
- NSCLC - first-line monotherapy (PD-L1 ≥50%) or + chemotherapy; second-line post-platinum
- Head & neck SCC - recurrent/metastatic ± chemotherapy
- Urothelial carcinoma - post-platinum; first-line in cisplatin-ineligible patients
- Triple-negative breast cancer - neoadjuvant + adjuvant (+ chemotherapy)
- Gastric/GEJ adenocarcinoma - first-line + chemotherapy (CPS ≥1)
- Classical Hodgkin lymphoma - relapsed/refractory
- Cervical, endometrial, esophageal, hepatocellular, Merkel cell, RCC - various lines
- MSI-H / dMMR tumors (any site) - tissue-agnostic approval
- TMB-high ≥10 mut/Mb tumors (any site) - tissue-agnostic approval
The tissue-agnostic approvals (based on molecular biomarkers, not tumor origin) were landmark firsts in oncology.
Key Biomarkers
| Biomarker | Test | Relevance |
|---|---|---|
| PD-L1 (CPS/TPS) | IHC | Required for monotherapy in NSCLC, gastric, HNSCC |
| MSI-H / dMMR | PCR / IHC | Tissue-agnostic approval; strong predictor of response |
| TMB ≥10 mut/Mb | Next-gen sequencing | Tissue-agnostic approval |
Adverse Effects
Adverse effects are immune-related adverse events (irAEs) from unbridled T-cell activation. Less frequent than anti-CTLA-4 agents but potentially severe:
| System | Event |
|---|---|
| Pulmonary | Pneumonitis (can be fatal) |
| GI | Colitis, diarrhea |
| Liver | Immune hepatitis |
| Endocrine | Hypothyroidism, hyperthyroidism, hypophysitis, adrenal insufficiency, type 1 DM |
| Renal | Nephritis |
| Neurological | Peripheral neuropathy, myasthenia gravis, encephalitis |
| Cardiac | Myocarditis (rare but high mortality) |
| Skin | Rash, pruritus, rarely SJS/TEN |
Common (>20%): Fatigue, nausea, rash, pruritus, arthralgia, diarrhea, decreased appetite.
irAE Management
| Grade | Action |
|---|---|
| Grade 1 | Continue; symptomatic treatment |
| Grade 2 | Withhold; oral prednisolone 1-2 mg/kg/day; resume when ≤ Grade 1 |
| Grade 3-4 | Permanently discontinue; IV methylprednisolone; infliximab for steroid-refractory colitis/hepatitis |
| Endocrinopathies | Often require lifelong hormone replacement |
Contraindications & Special Precautions
- Pregnancy: Contraindicated (IgG crosses placenta)
- Active autoimmune disease: Relative contraindication - risk of exacerbation
- Organ transplant recipients: Risk of allograft rejection
- Pseudo-progression: Tumors may initially enlarge on imaging due to immune infiltration before shrinking - use iRECIST criteria, not standard RECIST
- Durable responses: Some melanoma patients have responses lasting >10 years, even after drug discontinuation
- Combination use: + ipilimumab (melanoma, NSCLC, RCC) gives synergistic benefit but higher irAE rates; + lenvatinib in RCC and endometrial cancer; + chemotherapy as standard backbone in multiple cancers
Monitoring
TSH/free T4 every 3-6 months; LFTs, creatinine, blood glucose before each cycle; troponin if cardiac symptoms; chest imaging if respiratory symptoms arise.
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics; Lippincott Illustrated Reviews Pharmacology; Washington Manual of Medical Therapeutics; Goldman-Cecil Medicine
note on insulin guidelines and its caluclations
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I have all the content needed. Here is the comprehensive but concise note:
Insulin: Guidelines and Calculations
1. Types of Insulin Preparations
| Type | Examples | Onset | Peak | Duration |
|---|---|---|---|---|
| Ultra-rapid acting | Faster aspart, lispro-aabc | 5-10 min | 1-3 hr | 3-5 hr |
| Rapid-acting analogue | Lispro, Aspart, Glulisine | 10-20 min (15-30 min) | 1-3 hr | 3-5 hr |
| Short-acting (Regular) | Human Regular (U-100, U-500) | 30-60 min | 2-4 hr | 5-8 hr |
| Intermediate-acting | NPH | 2-4 hr | 6-10 hr | 16-20 hr |
| Long-acting | Glargine U100, Detemir | 1.5-2 hr | Peakless | 16-20 hr |
| Ultra-long-acting | Glargine U300, Degludec | 1.5-2 hr | Peakless | >24-42 hr |
| Premixed | 70/30 NPH/Regular, 75/25 lispro mix | Variable | Dual peak | Variable |
Prescribing safety note: Always write "units" in full - never abbreviate as "U" (risk of misinterpretation as a zero). Prescribe by full brand name including concentration number (e.g., Lantus U-100).
2. Indications for Insulin Therapy
Type 1 DM
- Mandatory for survival - all patients require exogenous insulin from diagnosis
Type 2 DM - initiate insulin when:
- Distinction between T1DM and T2DM is unclear
- HbA1c ≥ 8.5% at diagnosis
- Random blood glucose ≥ 250 mg/dL
- Presence of DKA or hyperosmolar hyperglycemic state
- Glycemic targets not met with oral agents and/or GLP-1 agonists
- Pregnancy with diabetes not controlled by lifestyle/metformin
3. Glycemic Targets
| Parameter | General Target | Modified for High-risk/Elderly |
|---|---|---|
| HbA1c | < 7.0% | < 8.0% (frail elderly, hypoglycemia-prone) |
| Fasting BG | 80-130 mg/dL | Individualized |
| Post-prandial BG (2h) | < 180 mg/dL | Individualized |
| Time in Range (CGM) | > 70% (70-180 mg/dL) | |
| Time below range | < 4% (< 70 mg/dL) |
4. Insulin Dose Calculations
Step 1 - Total Daily Dose (TDD)
| Clinical Setting | Formula |
|---|---|
| General starting dose | 0.5 units/kg/day |
| Insulin-naive T2DM (conservative) | 0.2-0.3 units/kg/day |
| Established T1DM (full replacement) | 0.5-1.0 units/kg/day |
| Severe insulin resistance / T2DM | Up to 1.0-2.0 units/kg/day |
Example: 70 kg adult → TDD = 0.5 × 70 = 35 units/day
Step 2 - Basal-Bolus Split (50:50 Rule)
| Component | Fraction of TDD | Calculation (70 kg, TDD=35) |
|---|---|---|
| Basal insulin (glargine/detemir/degludec) | 50% of TDD | 35 × 0.5 = 17-18 units once daily |
| Bolus/prandial insulin (rapid-acting) | 50% of TDD | 17 units ÷ 3 meals = ~5-6 units per meal |
If detemir is used as basal: give as BID (split 50% TDD into two doses)
Step 3 - Carbohydrate-to-Insulin Ratio (CIR)
Determines how many grams of carbohydrate are covered by 1 unit of rapid-acting insulin.
| Insulin Type | Formula | Example (TDD = 35) |
|---|---|---|
| Rapid-acting (lispro, aspart) | 500 ÷ TDD | 500 ÷ 35 = 1 unit : 14 g carb |
| Regular insulin | 450 ÷ TDD | 450 ÷ 35 = 1 unit : 13 g carb |
How to use: If a meal contains 56 g carbohydrate and CIR = 1:14 → Bolus dose = 56 ÷ 14 = 4 units
Step 4 - Correction Factor (CF) / Insulin Sensitivity Factor (ISF)
Determines how much 1 unit of rapid-acting insulin will lower blood glucose (in mg/dL).
| Insulin Type | Formula | Example (TDD = 35) |
|---|---|---|
| Rapid-acting (lispro, aspart) | 1800 ÷ TDD | 1800 ÷ 35 = ~51 mg/dL per unit |
| Regular insulin | 1500 ÷ TDD | 1500 ÷ 35 = ~43 mg/dL per unit |
How to use: If pre-meal BG = 220 mg/dL and target is 120 mg/dL: Correction dose = (220 - 120) ÷ 51 = ~2 units
Step 5 - Pre-meal Bolus Dose (Full Calculation)
$$\text{Pre-meal bolus} = \underbrace{\frac{\text{Carb grams}}{\text{CIR}}}{\text{Meal coverage}} + \underbrace{\frac{\text{Actual BG} - \text{Target BG}}{\text{CF}}}{\text{Correction dose}}$$
Worked example (TDD = 35, CIR = 1:14, CF = 51, target BG = 120 mg/dL):
- Meal: 70 g carbohydrates; Pre-meal BG = 200 mg/dL
- Meal dose = 70 ÷ 14 = 5 units
- Correction dose = (200 - 120) ÷ 51 = 1.6 units ≈ 2 units
- Total pre-meal dose = 5 + 2 = 7 units
Pediatric Dosing (Harriet Lane Reference)
| Component | Formula | Example: 24 kg child |
|---|---|---|
| TDD | 0.5-1 unit/kg/day (use 0.75 as starting) | 0.75 × 24 = 18 units/day |
| Basal (glargine) | ½ TDD once daily | ½ × 18 = 9 units daily |
| Basal (detemir) | ½ TDD ÷ BID | ½ × 18 ÷ 2 = 4.5 units BID |
| CIR (rapid-acting) | 500 ÷ TDD | 500 ÷ 18 = 1 unit : 28 g carb |
| CIR (regular) | 450 ÷ TDD | 450 ÷ 18 = 1 unit : 25 g carb |
| CF (rapid-acting) | 1800 ÷ TDD | 1800 ÷ 18 = 1 unit drops BG by 100 mg/dL |
| CF (regular) | 1500 ÷ TDD | 1500 ÷ 18 = 1 unit drops BG by 83 mg/dL |
5. Insulin Regimens
Basal-Bolus (Intensive / Preferred for T1DM and advanced T2DM)
- Long-acting insulin once daily (glargine/degludec) or twice daily (detemir) = basal
- Rapid-acting insulin before each meal = bolus
- Adjust using CIR + CF at each meal
- Gold standard for physiologic insulin replacement
Basal-Only (Initial T2DM insulin therapy)
- Start with 10 units glargine at bedtime (or 0.1-0.2 units/kg)
- Titrate by 2 units every 3 days if fasting BG > 130 mg/dL
- Simple; good first step when adding insulin to oral agents
Split-Mixed (Twice Daily)
- 70/30 premixed insulin - morning and evening
- Less flexible; not suitable for carb counting
- Used when adherence to basal-bolus is poor
Continuous Subcutaneous Insulin Infusion (CSII - Insulin Pump)
- Uses rapid-acting insulin only
- Three programmable settings:
- Basal rate - continuous background infusion (units/hr, variable throughout day)
- Bolus/meal - CIR applied at mealtime
- Correction - CF applied when BG above target
- Risk: DKA with pump malfunction (no long-acting insulin on board)
6. Titration Guidelines (T2DM Basal Insulin)
| Fasting BG (mg/dL) | Dose Adjustment |
|---|---|
| > 180 | Increase by 4 units |
| 140-180 | Increase by 2 units |
| 110-139 | Increase by 1 unit |
| 80-110 | No change (at target) |
| 70-79 | Decrease by 2 units |
| < 70 (hypoglycemia) | Decrease by 10-20% |
7. Hypoglycemia - Recognition and Treatment
| Severity | BG | Symptoms | Treatment |
|---|---|---|---|
| Mild-Moderate | 54-70 mg/dL | Sweating, tremor, palpitations, hunger | Rule of 15: 15 g fast carbs → recheck in 15 min; repeat if still low |
| Severe | < 54 mg/dL | Confusion, seizure, loss of consciousness | Glucagon IM/SC 1 mg; or IV dextrose 50% (25 mL) |
Fast-acting carbohydrate sources (15 g): 4 glucose tablets, 120 mL fruit juice, 150 mL regular soda, 3 teaspoons of sugar.
8. Special Situations
| Situation | Recommendation |
|---|---|
| Illness / surgery | Never omit basal insulin; reduce dose by 20-25%; check BG 2-hourly |
| Ramadan fasting | Reduce basal by 20-30%; shift meal bolus to Suhoor/Iftar |
| Pregnancy | Tighter targets (FBG 70-95 mg/dL, 1h post-meal <140 mg/dL); avoid oral agents in T1DM |
| CKD | Reduce insulin dose (decreased renal clearance of insulin); monitor closely |
| Perioperative | Reduce basal by 25-50% night before surgery; hold all bolus insulin; target intraoperative BG 140-180 mg/dL |
| Glucocorticoid-induced hyperglycemia | NPH insulin timed to peak of steroid action is practical; or increase TDD |
Sources: Harrison's Principles of Internal Medicine 22e; Goldman-Cecil Medicine International Edition; Harriet Lane Handbook 23e; Goodman & Gilman's Pharmacological Basis of Therapeutics
briefly 1-2 pages
Based on the content already retrieved, here is the condensed 1-2 page note:
Insulin: Guidelines and Calculations
Types of Insulin
| Type | Examples | Onset | Peak | Duration |
|---|---|---|---|---|
| Rapid-acting | Lispro, Aspart, Glulisine | 10-20 min | 1-3 hr | 3-5 hr |
| Short-acting (Regular) | Human Regular | 30-60 min | 2-4 hr | 5-8 hr |
| Intermediate | NPH | 2-4 hr | 6-10 hr | 16-20 hr |
| Long-acting | Glargine, Detemir | 1.5-2 hr | Peakless | 16-20 hr |
| Ultra-long | Degludec, Glargine U300 | 1.5-2 hr | Peakless | >24-42 hr |
Always write "units" in full - never "U" (risk of 10-fold dosing error).
Indications to Start Insulin
- T1DM - mandatory from diagnosis
- T2DM: HbA1c ≥ 8.5% at diagnosis; random BG ≥ 250 mg/dL; DKA; failure of oral agents ± GLP-1 agonist; pregnancy
Glycemic Targets
| Parameter | Target |
|---|---|
| HbA1c | < 7.0% (< 8.0% in frail/elderly) |
| Fasting BG | 80-130 mg/dL |
| 2h Post-prandial | < 180 mg/dL |
| CGM Time in Range | > 70% (70-180 mg/dL) |
Insulin Dose Calculations
Step 1 - Total Daily Dose (TDD)
| Patient | Dose |
|---|---|
| General starting dose | 0.5 units/kg/day |
| Conservative (insulin-naive T2DM) | 0.2-0.3 units/kg/day |
| Full T1DM replacement | 0.5-1.0 units/kg/day |
Example: 70 kg adult → TDD = 0.5 × 70 = 35 units/day
Step 2 - Basal : Bolus Split (50:50)
| Component | Calculation | Example (TDD = 35) |
|---|---|---|
| Basal (glargine/degludec) | 50% of TDD once daily | 17-18 units OD |
| Prandial (rapid-acting) | 50% of TDD ÷ 3 meals | ~6 units per meal |
Step 3 - Carbohydrate-to-Insulin Ratio (CIR)
How many grams of carbohydrate are covered by 1 unit of insulin
| Insulin | Formula | Example (TDD = 35) |
|---|---|---|
| Rapid-acting (lispro/aspart) | 500 ÷ TDD | 500 ÷ 35 = 1 unit : 14 g carb |
| Regular insulin | 450 ÷ TDD | 450 ÷ 35 = 1 unit : 13 g carb |
Step 4 - Correction Factor (CF) / Insulin Sensitivity Factor
How many mg/dL does 1 unit of insulin drop blood glucose
| Insulin | Formula | Example (TDD = 35) |
|---|---|---|
| Rapid-acting | 1800 ÷ TDD | 1800 ÷ 35 = ~51 mg/dL per unit |
| Regular | 1500 ÷ TDD | 1500 ÷ 35 = ~43 mg/dL per unit |
Step 5 - Full Pre-meal Bolus Formula
$$\text{Bolus} = \frac{\text{Carb grams (meal)}}{\text{CIR}} + \frac{\text{Actual BG} - \text{Target BG}}{\text{CF}}$$
Worked example (TDD=35, CIR=1:14, CF=51, Target BG=120 mg/dL):
- Meal: 70 g carbs; Pre-meal BG: 200 mg/dL
- Meal dose: 70 ÷ 14 = 5 units
- Correction: (200 - 120) ÷ 51 = 2 units
- Total = 7 units pre-meal
Pediatric Quick Reference (Harriet Lane)
| Component | Formula | Example: 24 kg child |
|---|---|---|
| TDD | 0.75 units/kg/day | 18 units/day |
| Basal (glargine) | ½ TDD once daily | 9 units OD |
| CIR (rapid-acting) | 500 ÷ TDD | 1 unit : 28 g carb |
| CF (rapid-acting) | 1800 ÷ TDD | 1 unit drops BG by 100 mg/dL |
Insulin Regimens
Basal-Only (first step in T2DM): Start glargine 10 units at bedtime → titrate by 2 units every 3 days if fasting BG > 130 mg/dL.
Basal-Bolus (T1DM and advanced T2DM): Long-acting OD + rapid-acting before each meal using CIR + CF. Most physiologic approach.
Split-Mixed Twice Daily: 70/30 premixed morning + evening - simpler but inflexible.
Insulin Pump (CSII): Rapid-acting only; programs basal rate (units/hr) + meal bolus (CIR) + correction (CF). Risk of DKA with pump failure.
Basal Insulin Titration (T2DM)
| Fasting BG | Adjustment |
|---|---|
| > 180 mg/dL | Increase by 4 units |
| 140-180 mg/dL | Increase by 2 units |
| 110-139 mg/dL | Increase by 1 unit |
| 80-110 mg/dL | No change (at target) |
| < 70 mg/dL | Decrease by 10-20% |
Hypoglycemia Management
Rule of 15: If BG < 70 mg/dL → give 15 g fast carbs (4 glucose tablets / 120 mL juice) → recheck in 15 min → repeat if still low.
Severe hypoglycemia (unconscious): Glucagon 1 mg IM/SC or IV Dextrose 50% (25 mL bolus).
Special Situations
| Situation | Key Adjustment |
|---|---|
| Surgery / illness | Never omit basal; reduce dose 20-25%; check BG 2-hourly |
| CKD | Reduce TDD - decreased renal insulin clearance |
| Pregnancy | Tighter targets: FBG 70-95 mg/dL; 1h post-meal < 140 mg/dL |
| Steroids | NPH timed to steroid peak; or increase TDD proportionally |
| Ramadan | Reduce basal 20-30%; shift bolus to Suhoor/Iftar |
Sources: Harrison's Principles of Internal Medicine 22e; Goldman-Cecil Medicine; Harriet Lane Handbook 23e
This is a shared conversation. Sign in to Orris to start your own chat.