Female infertility in detail post graduate level, causes Investigations and management from barek and Novak and recent guidrlines
Reading File
Finding Sources
Finding Sources
Searching PubMed
"female infertility" AND "guidelines"
Finding Sources
Searching PubMed
"infertility" AND "evaluation" AND "management" AND "ASRM"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
"infertility" AND "ovarian reserve" AND "evaluation"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Female Infertility - Postgraduate Level
Source: Berek & Novak's Gynecology (Chapter 36), supplemented by recent guidelines (ACR 2026, ESHRE 2024)
Definition and Epidemiology
Infertility is defined as failure to achieve pregnancy after 12 months of regular, unprotected intercourse (or 6 months in women >35 years). Primary infertility means no prior pregnancy; secondary infertility means prior pregnancy has occurred. Fecundability is the probability of pregnancy per menstrual cycle; fecundity is the probability of achieving a live birth.
- Prevalence in the USA: 7.4% to 15.5% of couples
- About 90% of couples should conceive within 12 months
- Spontaneous conception is less likely with: age >42, infertility duration >4 years, severe endometriosis, or severe tubal disease
Causes of Infertility - Overall Distribution (Table 36-1):
| Etiology | Prevalence |
|---|---|
| Male factor only | 17-28% |
| Male + female combined | 8-39% |
| Female factor | 33-40% |
| Unexplained | 8-28% |
Female-specific causes:
| Female Etiology | Prevalence |
|---|---|
| Ovulatory dysfunction | 21-36% |
| Tubal or peritoneal factor | 16-28% |
| Miscellaneous | 9-12% |
INITIAL ASSESSMENT
The physician's first encounter sets the tone for all subsequent evaluation. Infertility is a couple's problem, and both partners should attend the initial visit.
History from the female partner:
- Menstrual cycle regularity, cycle length, dysmenorrhea, intermenstrual bleeding
- Pelvic pain or dyspareunia (suggesting endometriosis or PID)
- Prior pregnancies and outcomes
- History of PID, STIs, pelvic or abdominal surgery
- DES intrauterine exposure
- Review of systems for thyroid, adrenal, pituitary dysfunction (galactorrhea, hirsutism, weight changes)
- Coital frequency, sexual dysfunction
- Family history: premature ovarian failure, hereditary conditions (cystic fibrosis, thalassemia, Tay-Sachs)
Physical examination of the female partner:
- Height, weight, BMI, body habitus
- Hair distribution (hirsutism)
- Thyroid palpation
- Breast exam (galactorrhea)
- Pelvic exam: uterine size, adnexal masses, uterosacral nodularity
Basic investigations before starting any treatment:
- Semen analysis
- Confirmation of ovulation
- Documentation of tubal patency
- Ovarian reserve screening
DIAGNOSTIC ALGORITHM
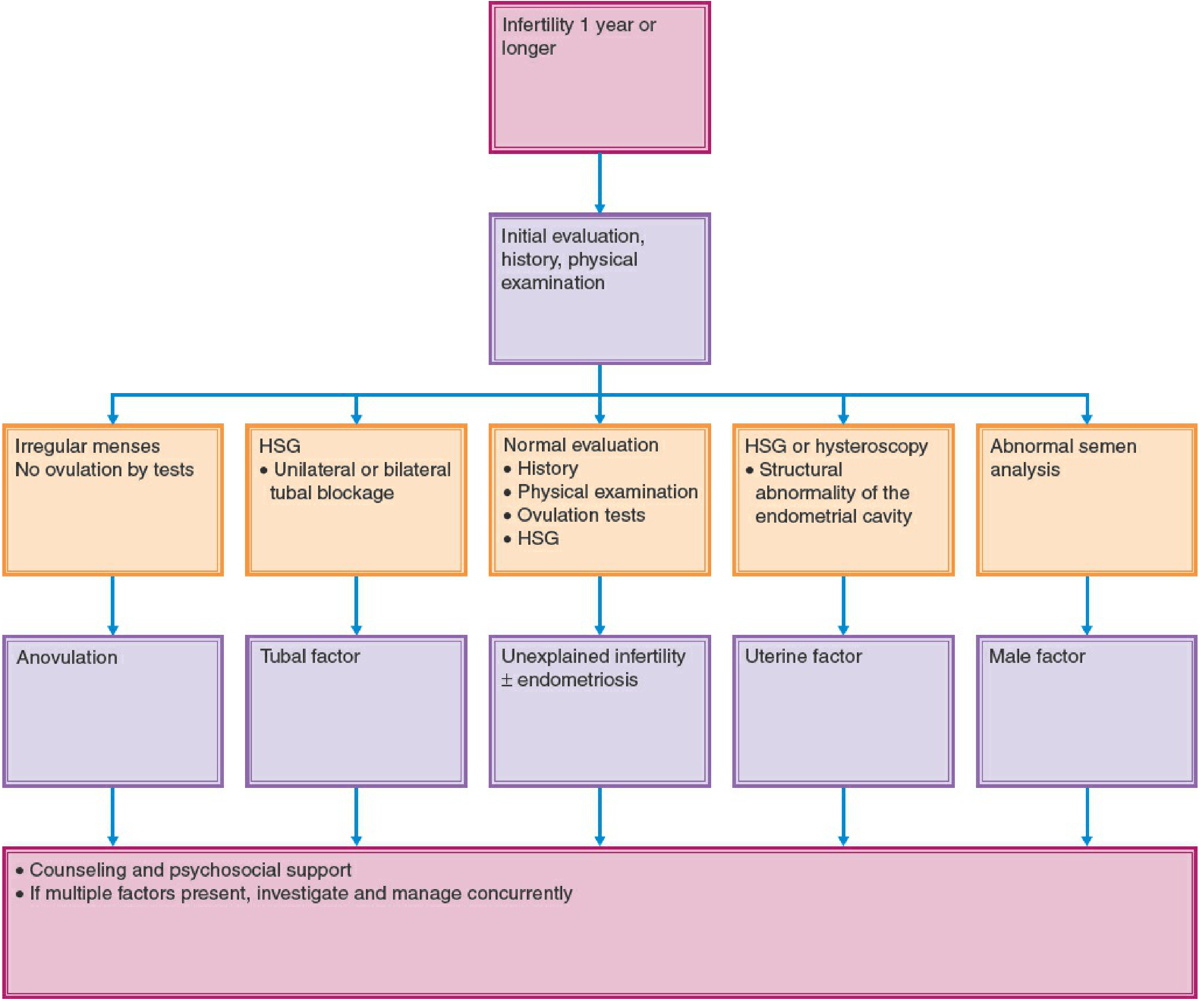
FIGURE 36-1 Diagnostic and treatment algorithm for infertility. HSG = hysterosalpingography. (Berek & Novak's Gynecology, Chapter 36)
CAUSES OF FEMALE INFERTILITY IN DETAIL
1. OVULATORY FACTOR (21-36% of female infertility)
Disorders of ovulation are among the most easily diagnosed and most treatable causes of infertility.
WHO Classification of Ovulatory Disorders:
- WHO Class I (Hypogonadotropic hypogonadism): hypothalamic/pituitary failure - low FSH, LH, E2 (e.g., hypothalamic amenorrhea, anorexia nervosa, exercise-related amenorrhea)
- WHO Class II (Normogonadotropic): normal FSH, LH - includes PCOS (most common)
- WHO Class III (Hypergonadotropic hypogonadism): elevated FSH - premature ovarian insufficiency/failure
Methods to Document Ovulation:
| Method | Details |
|---|---|
| Menstrual cycle regularity | Regular cycles (21-35 days) strongly suggest ovulation |
| LH surge detection kit | ELISA, threshold 35-50 mIU/mL; ovulation within 48 hours of surge; PPV 92%, NPV 95% |
| Midluteal progesterone | Day 21-23 of 28-day cycle; >3 ng/mL (10 nmol/L) confirms ovulation |
| Transvaginal ultrasound | Follicle size 17-19 mm (spontaneous) or 19-25 mm (clomiphene cycles) before ovulation; cul-de-sac fluid |
| Endometrial biopsy | Historically used for luteal phase defect - now largely abandoned |
| Basal body temperature | Biphasic rise of 0.3-0.5°C after ovulation - retrospective only |
Polycystic Ovarian Syndrome (PCOS) - Most Common Cause:
PCOS is the most common cause of oligo-ovulation and anovulation. Diagnosis by Rotterdam criteria (2 of 3):
- Oligo-ovulation or anovulation (oligomenorrhea/amenorrhea)
- Hyperandrogenemia (elevated androgens) or hyperandrogenism (clinical signs)
- Polycystic ovaries on ultrasound
Documentation of elevated serum LH:FSH ratio >2:1, elevated testosterone, DHEAS, and low SHBG supports the diagnosis.
2. TUBAL AND PERITONEAL FACTOR (16-28% of female infertility)
Tubal and peritoneal factors are responsible for 30-40% of cases of female infertility (Berek & Novak). Cervical factor accounts for no more than 5%.
Causes of tubal factor:
- Pelvic inflammatory disease (PID) - C. trachomatis is the most important cause
- Previous pelvic/abdominal surgery
- Ectopic pregnancy (with salpingectomy)
- Endometriosis with tubal/peritoneal involvement
- Salpingitis isthmica nodosa
- Tuberculosis (common in developing countries)
Types of tubal occlusion:
- Proximal tubal occlusion (can mimic spasm - false positive 11% on HSG)
- Distal tubal occlusion/hydrosalpinx - causal in 85% of all tubal infertility
- Peritubal adhesions
3. UTERINE FACTORS (up to 15% of couples)
Congenital anomalies:
- Müllerian anomalies: bicornuate, unicornuate, septate, didelphys uterus
- DES exposure in utero: T-shaped uterus, hypoplastic uterus
Acquired abnormalities:
- Leiomyomas: submucosal > intramural > subserosal for fertility impact. Leiomyomas have not been shown to be a direct cause of infertility; however, submucosal and cavity-distorting intramural fibroids should be removed.
- Intrauterine synechiae/Asherman syndrome: caused by trauma to the basalis layer, usually iatrogenic after uterine evacuation, myomectomy, or TB. Causes amenorrhea, menstrual irregularities, recurrent pregnancy loss.
- Endometrial polyps: incidence 6-32% in infertile women; disordered endometrial receptivity mechanism; polypectomy improves IUI pregnancy rates 2.1-fold.
- Endometritis: plasma cells in endometrium found in 56.8% of unexplained infertility patients; treat with antibiotics.
- Luteal phase defect and endometrial receptivity issues.
4. DIMINISHED OVARIAN RESERVE (DOR)
DOR is defined based on age, biochemical parameters, sonographic findings, poor follicular response to ovarian stimulation, and oocyte yield during IVF. Prevalence increased to 26% in U.S. IVF cohorts.
Fecundability declines from early 30s, accelerates after 37, and is rare after 45. Fertility peaks at age 20.
Etiologies of prematurely diminished ovarian reserve:
- Iatrogenic: chemotherapy, pelvic radiation, ovarian surgery
- Pelvic endometriosis and adhesions
- Immunologic factors
- Genetic: FMR1 premutation (fragile X), Turner syndrome mosaicism
5. ENDOMETRIOSIS AND PELVIC FACTOR
Endometriosis affects fertility through:
- Distortion of tubo-ovarian anatomy (adhesions)
- Impaired implantation (altered endometrial receptivity)
- Toxic peritoneal environment affecting gametes
- Decreased ovarian reserve (endometrioma)
- Occult mechanisms in minimal/mild disease
6. CERVICAL FACTOR
Accounts for <5% of infertility. Post-coital test is no longer routinely recommended. Cervical hostility (anti-sperm antibodies, thick mucus) can impair sperm penetration.
7. UNEXPLAINED INFERTILITY (8-28%)
Defined when standard infertility workup (semen analysis, ovulation documentation, tubal patency, ovarian reserve) is completely normal. Putative mechanisms include:
- Occult male factor (impaired sperm DNA integrity despite normal semen analysis)
- Oocyte factors (premature zona hardening, mitochondrial dysfunction, aberrant spindle formation)
- Luteinized unruptured follicle syndrome (25% in unexplained infertility vs 10% in fertile women)
- Occult endometriosis
- Undiagnosed pelvic pathology
- Immunologic factors, chronic endometritis, uterine microbiome abnormalities
INVESTIGATIONS
Ovarian Reserve Testing
| Test | Normal Values | Clinical Significance |
|---|---|---|
| Basal day 3 FSH | <10 mIU/mL (lab-dependent) | Elevated FSH = diminished reserve; predicts poor gonadotropin response |
| Basal day 3 E2 | <80 pg/mL | Elevated E2 masks FSH elevation; advanced follicular growth in aging |
| Anti-Müllerian hormone (AMH) | >1.0 ng/mL (varies by lab) | Best single marker; reflects primordial follicle pool; not cycle-day dependent |
| Antral follicle count (AFC) | >10 total (≥5 each ovary) | Transvaginal USS day 2-4; best functional marker alongside AMH |
| Clomiphene citrate challenge test (CCCT) | Normal day 3 FSH and day 10 FSH post CC | More sensitive than basal FSH alone for predicting poor response |
| Inhibin B | >45 pg/mL | Poor predictive value alone; improves when combined with CCCT |
Recent evidence (2024 systematic review, PMID 37964401): AMH has been confirmed as the best single marker for screening and predicting ovarian reserve; however it should not be used in isolation for clinical decision-making.
Tubal Patency Testing
| Test | Details |
|---|---|
| HSG (Hysterosalpingography) | First-line; evaluates tubal patency and uterine cavity; oil-soluble contrast may have therapeutic effect |
| Sonohysterography (SHG/SIS) | Assesses uterine cavity; can detect polyps, fibroids, synechiae |
| Laparoscopy + Chromopertubation | Gold standard for tubal and peritoneal disease; allows simultaneous treatment; indigo carmine dye instilled transcervically |
| Falloposcopy | Direct fiberoptic visualization of tubal ostia; limited by instrumentation availability |
| Hysteroscopy | Direct visualization of uterine cavity; diagnostic and therapeutic |
ACR Appropriateness Criteria 2026 (PMID 41706082): For initial imaging in female infertility, HSG remains the usual first-line test for tubal patency assessment. Sonohysterography is appropriate for uterine cavity evaluation. MRI pelvis is usually appropriate when Müllerian anomalies are suspected.
Hormone Panel (Ovulatory Workup)
| Hormone | Timing | Purpose |
|---|---|---|
| FSH, LH | Day 2-3 | Ovarian reserve, ovulatory function |
| Estradiol (E2) | Day 2-3 | Interpret with FSH |
| AMH | Any day | Ovarian reserve |
| Prolactin | Any day (morning, fasting) | Exclude hyperprolactinemia |
| TSH, T4 | Any day | Thyroid dysfunction |
| Total testosterone, DHEAS | Any day | Hyperandrogenism workup |
| Progesterone | Day 21-23 | Confirm ovulation (>3 ng/mL) |
| 17-OH progesterone | Day 3 | Exclude non-classical CAH |
| Fasting insulin, glucose | Any day | Metabolic assessment in PCOS |
Uterine Cavity Assessment
- SIS (saline infusion sonography): first-line for cavity
- 3D transvaginal ultrasound: Müllerian anomalies
- Hysteroscopy: gold standard for cavity pathology
- MRI: uterine anomalies, adenomyosis, fibroid mapping
Genetic Testing (Selected Cases)
- Karyotype: POI/POF, recurrent pregnancy loss
- FMR1 premutation: premature ovarian insufficiency
- Carrier testing: CF, thalassemia, fragile X (based on ethnicity and family history)
- CFTR gene: in setting of male CBAVD (female partner testing indicated)
MANAGEMENT
Diagnostic Algorithm for Anovulation
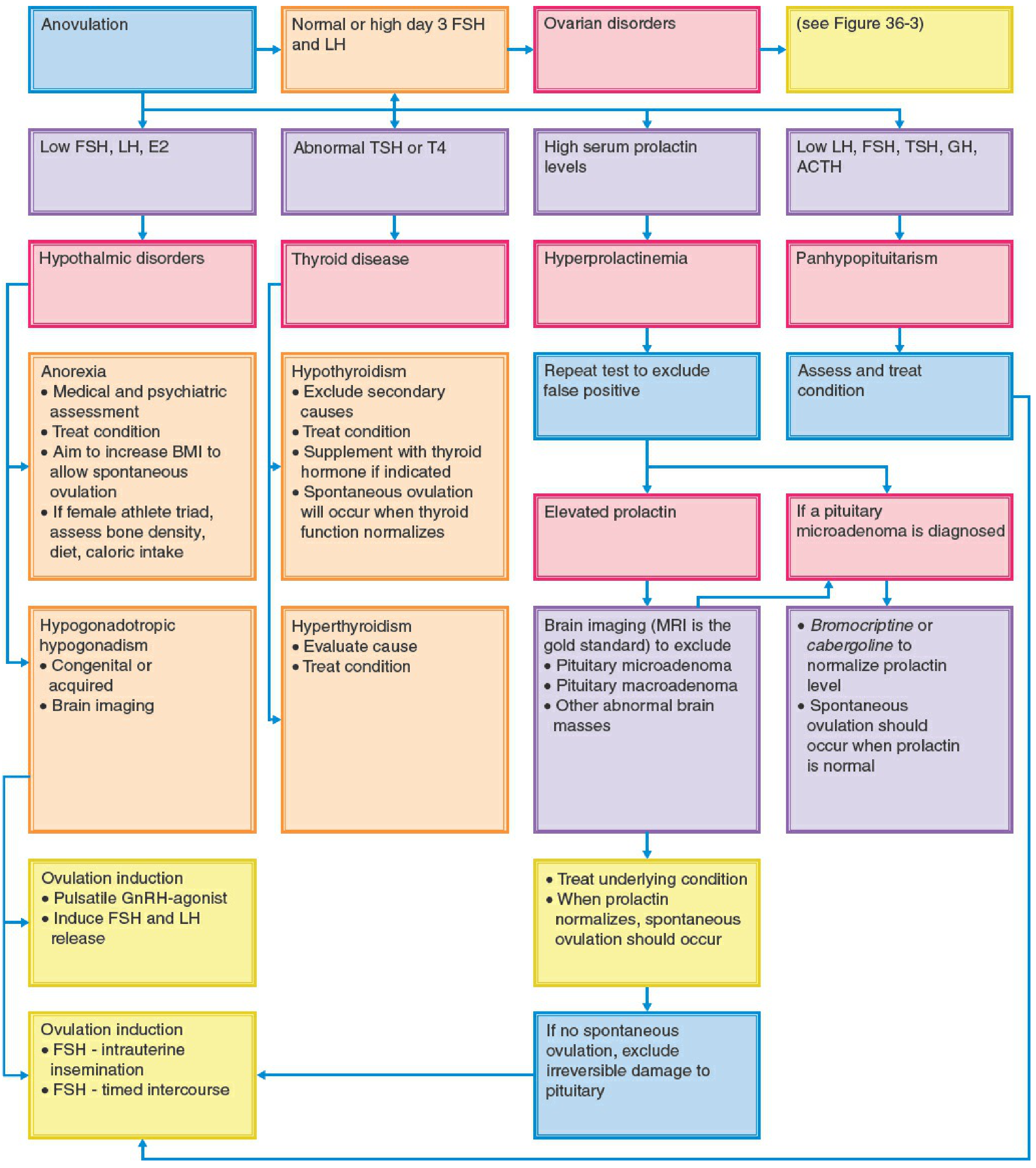
FIGURE 36-2 Diagnostic and treatment algorithm for anovulation. FSH, LH, E2, TSH, T4, GH, ACTH, BMI, MRI, GnRH. (Berek & Novak's Gynecology, Chapter 36)
A. Management of Ovulatory Dysfunction
PCOS Treatment (stepped approach)
Step 1 - Lifestyle modification:
- Weight loss in overweight/obese patients. Weight loss of ~20 pounds increases spontaneous conception rates.
- Exercise, reduced caloric intake
Step 2 - Oral ovulation induction agents:
| Agent | Mechanism | Dose | Outcomes |
|---|---|---|---|
| Letrozole (aromatase inhibitor) | Blocks estrogen synthesis → removes negative feedback on pituitary → FSH release | 2.5-7.5 mg day 3-7 | First-line per ASRM - higher live birth rates than clomiphene in PCOS (NEJM 2014) |
| Clomiphene citrate (CC) | Anti-estrogenic at hypothalamic level → FSH release | 50-150 mg day 3-7 or 5-9 | Ovulation rate 70-85%, pregnancy rate 30-40% over 6 cycles |
- Maximum 6 ovulatory cycles with CC or letrozole before stepping up
- Resistance: failure to ovulate at maximum dose
Step 3 - Gonadotropin therapy (for CC/letrozole-resistant PCOS):
- FSH injections; low initial dose 37.5-75 IU/day; step-up protocol
- Monitor with serial transvaginal USS + E2 levels
- Trigger with hCG when 1-2 follicles reach 16-18 mm; E2 150-300 pg/mL per dominant follicle
- Ovulation in 43-83%, pregnancy 21-29% (vs clomiphene-resistant population)
- Risk of OHSS and multiple gestation (36%); use GnRH agonist trigger if OHSS risk high
- Maximum dose rarely exceeds 225 IU/day
Step 4 - Surgical ovarian drilling (laparoscopic):
- Alternative to gonadotropins for CC-resistant PCOS
- 3-15 punctures per ovary by electrocautery/laser
- Within 12 months: ovulation 52%, pregnancy 26-48%, live birth 13-32%
- No multiple gestation risk
- Complications: adhesions, recurrence of anovulation, theoretical ovarian failure
Gonadotropin contraindications (Table 36-8 Berek & Novak):
- Primary ovarian failure with elevated FSH
- Uncontrolled thyroid/adrenal dysfunction
- Intracranial lesion (pituitary tumor)
- Undiagnosed abnormal uterine bleeding
- Ovarian cysts not due to PCOS
- Sex hormone-dependent tumors
- Pregnancy
Hyperprolactinemia Treatment
- MRI pituitary to exclude macroadenoma
- Dopamine agonists are first-line:
- Bromocriptine: 1.25-7.5 mg/day; normalizes prolactin and restores ovulation in 80-90%
- Cabergoline: 0.25 mg twice weekly (better tolerated, more effective)
- Spontaneous ovulation resumes when prolactin normalizes
Hypothalamic Amenorrhea
- Weight restoration, treat eating disorder, reduce exercise
- Pulsatile GnRH therapy: IV/SC administration every 60-90 min to restore pulsatile FSH/LH release
- Exogenous gonadotropins (FSH + LH/hMG): if pulsatile GnRH unavailable
- Avoid CC (ineffective in hypogonadotropic state)
Thyroid Disease
- Treat hypothyroidism with levothyroxine - spontaneous ovulation may resume
- Treat hyperthyroidism; fertility usually improves with euthyroid state
B. Management of Tubal Factor Infertility
Proximal tubal occlusion:
- Proximal tubal catheterization/cannulation via HSG or hysteroscopy: restores patency in up to 85%; reocclusion rate 30%
- Ongoing pregnancy rates 12-44%
- Microsurgical tubocoronal anastomosis: pregnancy rates up to 68% (small studies)
- If persistent occlusion or recurrence → IVF
Distal tubal occlusion / Hydrosalpinx:
- Distal disease causes 85% of all tubal infertility
- Hydrosalpinx reduces IVF success rates; salpingectomy or proximal occlusion of the hydrosalpinx before IVF is recommended
- Salpingostomy for distal occlusion in selected young patients (<35 years) with mild disease, normal tubal mucosa, minimal adhesions
- IVF for older patients, severely damaged tubes, bilateral disease
General principle: As ART success rates improve, surgical indications for tubal infertility narrow. IVF is increasingly preferred over tubal surgery.
C. Management of Uterine Factor
Fibroids:
- Submucosal and cavity-distorting intramural fibroids: remove before infertility treatment
- Non-cavity-distorting intramural fibroids: utility of removal is unknown
- Hysteroscopic myomectomy: preferred for submucosal fibroids
- Laparoscopic/open myomectomy: for intramural/subserosal
- GnRH agonists pre-operatively to shrink large (>5-6 cm) fibroids and reduce blood loss
- Uterine artery embolization: relatively contraindicated in fertility-desiring women
Asherman Syndrome:
- Hysteroscopic resection of synechiae - treatment of choice
- Post-operative estrogen therapy (1 month) ± IUD placement to prevent adhesion reformation
- TB endometritis: very poor prognosis
Endometrial Polyps:
- Hysteroscopic polypectomy: 2.1-fold improvement in pregnancy rates before IUI
- Curettage or blind avulsion also used
Müllerian Anomalies:
- Uterine septum: hysteroscopic metroplasty (most common and treatable anomaly)
- Bicornuate uterus: abdominal metroplasty (Strassman procedure) in selected cases
- DES-related anomalies: generally managed with ART
D. Management of Diminished Ovarian Reserve (DOR)
Options:
- Autologous IVF with controlled ovarian stimulation
- Stimulation protocols: microdose GnRH flare, GnRH antagonist, minimal stimulation
- Adjuncts: DHEA (25 mg TID x 2-5 months), transdermal testosterone 10-12.5 mg x 14-28 days pretreatment, CoQ10, growth hormone, vitamin D, omega-3 fatty acids (varying evidence)
- Donor oocyte IVF: live birth rates 40-60% regardless of recipient age
- Donor embryo
- Adoption
Counseling must disclose that per-cycle pregnancy rates are low in DOR, particularly in older women.
E. Endometriosis-Associated Infertility
Minimal/mild endometriosis (Stage I/II):
- Laparoscopic ablation/excision marginally improves spontaneous conception rates vs no treatment
- IUI + ovarian stimulation: empiric option
- IVF if above fails or if age-related DOR present
Severe endometriosis (Stage III/IV):
- Surgical excision of endometriosis and adhesiolysis improves fertility outcomes
- Ovarian endometrioma: cystectomy preferred over ablation (but increases DOR risk - laparoscopic hemostasis method matters per 2024 systematic review, PMID 38064608)
- ART/IVF is often first-line for Stage III/IV
F. Management of Unexplained Infertility
Historically treated with superovulation + IUI (CC/IUI, letrozole/IUI, FSH/IUI). This approach is no longer the treatment of choice based on high-quality evidence:
- FASTT trial: For age 21-39, ongoing pregnancy rates: CC/IUI 7.6%, FSH/IUI 9.8%, IVF 30.7% - IVF clearly superior with shorter time to pregnancy
- FORT-T trial: For age 38-42, IVF had higher live birth rates than CC/IUI or FSH/IUI
- Meta-analysis of 1,159 participants: CC alone or CC/IUI showed no improvement in pregnancy/live birth vs no treatment or placebo
Current evidence-based approach:
- IVF is first-line treatment for unexplained infertility based on evidence
- 2024 Australian/ESHRE guideline (PMID 39277816): recommends IVF as first-line treatment with or without ICSI for unexplained infertility
- Superovulation/IUI continues to be used in practice mainly due to lower per-cycle cost, patient preference, and insurance coverage
G. Assisted Reproductive Technology (ART)
ART techniques include:
- IVF (conventional fertilization)
- ICSI (intracytoplasmic sperm injection) - for male factor or fertilization failure
- GIFT, ZIFT (largely abandoned due to improved IVF outcomes)
- Oocyte cryopreservation (fertility preservation)
- Embryo cryopreservation
- Preimplantation genetic testing (PGT-A/PGT-M)
- Gestational carrier / surrogacy
- Donor oocyte or embryo
IVF Protocol Components:
-
Pituitary downregulation:
- GnRH agonist (long protocol): started day 21 of preceding cycle; 10-14 days to achieve suppression; continued until hCG trigger
- GnRH antagonist (flexible/fixed): started day 6 of stimulation or when leading follicle reaches 14 mm; advantages - shorter treatment, less OHSS risk
-
Controlled ovarian hyperstimulation (COH):
- FSH ± LH (hMG) injections
- Monitor with serial TVS and E2 levels (every 1-3 days after day 4-5)
-
Trigger injection:
- hCG (conventional): when 2+ follicles ≥18 mm; ovulation 34-36 hours after
- GnRH agonist trigger (leuprolide 500 mcg SC): preferred when OHSS risk high (PCOS, high E2, many follicles); requires progesterone luteal support
-
Oocyte retrieval: Transvaginal ultrasound-guided 34-36 hours after trigger
-
Fertilization: Conventional IVF or ICSI
-
Embryo transfer: Day 3 (cleavage stage) or day 5 (blastocyst)
-
Luteal phase support: Progesterone (vaginal/IM) from day of retrieval
Complications of ART:
- Ovarian Hyperstimulation Syndrome (OHSS): prevent with agonist trigger, coasting, cryopreservation all embryos, cabergoline
- Multiple gestation: serious complication; single embryo transfer policy reduces this
- Ectopic/heterotopic pregnancy
- Cycle cancellation
- Oocyte retrieval complications (bleeding, infection)
- Stress: most common reason for treatment discontinuation
ART Outcomes (SART data): Live birth rate per cycle varies by age - approximately 40% per cycle at age <35, declining to <10% by age 42+ using autologous oocytes.
H. Fertility Preservation
Indications:
- Cancer patients before chemotherapy/radiation
- Premature ovarian insufficiency risk
- Genetic conditions
- Social/elective freezing
Options:
- Oocyte cryopreservation (vitrification): established technique
- Embryo cryopreservation: most established
- Ovarian tissue cryopreservation and transplantation: experimental/established in select centers
LIFESTYLE AND MODIFIABLE FACTORS
| Factor | Evidence |
|---|---|
| Obesity (BMI >35) | Lower IVF pregnancy rates; impaired endometrial receptivity, disrupted HPO axis |
| Tobacco smoking | Lower live birth rates with all conception methods; higher IVF cycle cancellation rates |
| Alcohol: low-moderate intake (<12g/day) | Does NOT significantly impact ART outcomes |
| Caffeine (<200 mg/day) | Does NOT significantly impact ART outcomes |
| Weight loss in obese women | Improves spontaneous conception rates (not IVF rates in BMI <35) |
SUMMARY: STEPWISE MANAGEMENT FRAMEWORK
Female Infertility Workup:
├── History + Physical Exam
├── Basic workup (BOTH partners simultaneously):
│ ├── Semen analysis (male)
│ ├── Ovulation documentation (progesterone, LH kits, USS)
│ ├── Ovarian reserve (AMH, day 3 FSH/E2, AFC)
│ ├── Tubal patency (HSG)
│ └── Uterine cavity (SIS or hysteroscopy)
│
├── Anovulation identified → Letrozole first-line → CC → Gonadotropins → Drilling
│
├── Tubal factor → IVF preferred over surgery (except proximal cannulation, reversal)
│
├── Uterine factor → Hysteroscopic/surgical correction then ART if needed
│
├── DOR → Autologous IVF → Donor oocyte IVF
│
├── Endometriosis → Surgery for Stage III/IV → ART
│
└── Unexplained → IVF first-line (not CC/IUI per FASTT/FORT-T trials)
RECENT GUIDELINES UPDATE
| Guideline | Key Recommendation |
|---|---|
| ACR Appropriateness Criteria - Female Infertility (2026) [PMID 41706082] | HSG remains first-line for tubal assessment; SHG for uterine cavity; MRI for suspected Müllerian anomalies |
| ESHRE / Australian Evidence-Based Guideline - Unexplained Infertility (2024) [PMID 39277816] | IVF recommended as first-line treatment for unexplained infertility |
| AMH systematic review (2024) [PMID 37964401] | AMH is the best single marker for ovarian reserve screening and IVF prediction but should not be used in isolation |
| Endometrioma hemostasis (2024) [PMID 38064608] | Choice of hemostasis method during laparoscopic cystectomy significantly impacts ovarian reserve - bipolar coagulation causes greater DOR than suturing or hemostatic agents |
| ASRM | Letrozole replaces clomiphene as first-line ovulation induction in PCOS |
Berek & Novak's Gynecology, Chapter 36 (Reproductive Endocrinology & Infertility), authored by Aubuchon, Yao, Fujii, Burney, Schust. All tables and algorithms cited from this chapter.
This is a shared conversation. Sign in to Orris to start your own chat.