Thyroid embryology and anatomy in detail, thyroid physiology and metabolism, Benign thyroid diseases, malignant thyroid diseases and its management in detail, and teach me all this in creative manner
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching Images
thyroid gland anatomy embryology development
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Searching Images
thyroid hormone synthesis T3 T4 iodination follicle
Reading File
Searching Images
papillary thyroid carcinoma follicular medullary anaplastic cancer histology
Reading File
Searching Images
Graves disease thyroid goiter hyperthyroidism exophthalmos
Here's your complete Thyroid Odyssey — all 8 chapters from embryo to cancer management, taught creatively with visuals, tables, mnemonics, and clinical pearls. Here's a quick roadmap of what you just learned:
📚 What Was Covered
| Chapter | Topic |
|---|---|
| 🥚 Ch. 1 | Embryology — Median/lateral anlage, descent, thyroglossal duct, anomalies |
| 🗺️ Ch. 2 | Anatomy — Blood supply, dangerous nerves (RLN, EBSLN), parathyroids |
| 🔬 Ch. 3 | Histology — Follicular units, colloid, C-cells, normal appearance |
| ⚗️ Ch. 4 | Physiology — HPT axis, 7-step synthesis, T3/T4 actions, special states |
| 🌊 Ch. 5 | Benign diseases — Hypo/hyperthyroidism, Graves', Hashimoto's, goiter, nodule workup (TI-RADS + Bethesda) |
| 🦀 Ch. 6 | Malignant diseases — PTC, FTC, MTC (RET/MEN2), ATC (BRAF breakthrough) |
| 🔪 Ch. 7 | Surgery & RAI — Indications, complications, surveillance |
| 🎓 Summary | Mnemonics, quick tables, and 10 golden clinical pearls |
The guide is built from Sabiston's Textbook of Surgery, Harrison's, Schwartz's, and Katzung's — authoritative and exam-ready. Ask if you want me to drill down further on any specific topic!
Give me this whole thing again
🦋 The Complete Thyroid Odyssey
From Embryo to Excellence — A Creative Master Guide
"The thyroid is the body's thermostat, metabolism maestro, and a butterfly-shaped powerhouse hiding beneath your larynx."
🥚 CHAPTER 1: The Origin Story — Thyroid Embryology
🎬 Scene: Week 3–4 of Gestation — The Big Bang of the Thyroid
Picture the embryo — a tiny universe just beginning. Deep in the floor of the pharynx, a patch of endodermal epithelium thickens and says, "I have a purpose." This is the median thyroid anlage — the founding father of your thyroid gland.
The Two Heroes: Median & Lateral Thyroid Anlagen
🏛️ The Median Thyroid Anlage (the Architect)
| Stage | Event |
|---|---|
| Week 3–4 | Endodermal thickening in the foregut floor of the pharynx |
| Week 4–5 | Outpouching adjacent to myocardial cells → bilobed diverticulum forms |
| Week 5 | Thyroglossal duct keeps it tethered to the tongue like an umbilical cord |
| Week 5 | Thyroglossal duct solidifies → then fragments and disappears |
| Week 7 | Thyroid descends to its final home anterior to the trachea |
| Week 10 | Follicles form → thyroid hormone synthesis begins! 🎉 |
The obliteration of the thyroglossal duct leaves two hallmark relics:
- Foramen cecum at the base of the tongue (the "scar")
- Pyramidal lobe (an upward extension of the isthmus, present in ~50% of people)
🏛️ The Lateral Thyroid Anlage (the Immigrant)
- Arises from the pharyngeal endoderm (4th pharyngeal pouch)
- Migrates medially and fuses with the median anlage
- Carries C-cells (parafollicular cells) — the calcitonin-secreting cells
- Constitutes a small portion of the final gland but a clinically vital one
📌 Mnemonic: "The Median Architect DESCENDS from the tongue; the Lateral Immigrant FUSES from the sides."
🚨 Embryological Anomalies — When Things Go Wrong
| Anomaly | Cause | Result |
|---|---|---|
| Thyroglossal duct cyst | Incomplete obliteration of thyroglossal duct | Midline neck cyst; moves with tongue protrusion and swallowing |
| Lingual thyroid | Failure of median anlage to descend | Thyroid tissue at base of tongue; may be the ONLY thyroid |
| Ectopic thyroid | Arrest anywhere along descent path | Can be sublingual, substernal, intrathoracic |
| Pyramidal lobe | Remnant of thyroglossal duct | Normal variant, clinically important in thyroidectomy |
🗺️ CHAPTER 2: The Anatomy — Geography of the Butterfly
Meet the Gland
The thyroid sits like a brown butterfly in the neck — two lobes (right and left) connected by the isthmus, which crosses the 2nd–3rd tracheal rings. In 50% of individuals, a pyramidal lobe extends upward like an antenna.
Size & Weight:
- Normal: ~20–30 grams
- Dimensions: Each lobe ~5 cm long × 3 cm wide × 2 cm thick
🩸 Blood Supply — The Thyroid's Lifelines
| Vessel | Origin | Notes |
|---|---|---|
| Superior thyroid artery | External carotid artery | First branch; supplies upper pole |
| Inferior thyroid artery | Thyrocervical trunk (subclavian) | Supplies lower pole; crosses RLN |
| Thyroid ima artery | Brachiocephalic or aortic arch | Present in ~1.5–12%; important in surgery! |
| Superior thyroid vein | Drains → internal jugular vein | |
| Middle thyroid vein | Drains → internal jugular vein | |
| Inferior thyroid vein | Drains → brachiocephalic vein |
⚠️ Surgical pearl: Ligation of the superior thyroid vessels must be done as far caudally as possible to avoid injuring the external branch of the superior laryngeal nerve (EBSLN) — the nerve that gives your voice its high notes.
🧠 Nerve Neighbors — The Dangerous Duo
1. Recurrent Laryngeal Nerve (RLN) — The Prima Donna
- Runs in the tracheoesophageal groove
- On the right: loops under the subclavian artery
- On the left: loops under the aortic arch (longer course)
- Injury → hoarseness, bilateral injury → respiratory emergency
- Non-recurrent RLN occurs in ~1% on the right (associated with aberrant subclavian artery)
2. External Branch of Superior Laryngeal Nerve (EBSLN) — The Quiet Victim
- Runs alongside the superior thyroid artery
- Innervates the cricothyroid muscle (pitch control)
- Injury → loss of high-pitched phonation (the "Amelita Galli-Curci injury")
🫘 Parathyroid Glands — The Tiny Neighbors
- Usually 4 in number (2 superior, 2 inferior)
- Superior parathyroids: arise from 4th pharyngeal pouch — more consistent in location
- Inferior parathyroids: arise from 3rd pharyngeal pouch — variable position, can be ectopic
- Accidental removal → hypocalcemia, tetany
- Blood supply: branches of inferior thyroid artery

🔊 Lymphatic Drainage
- Central compartment (Level VI): Prelaryngeal, pretracheal, paratracheal nodes — first echelon
- Lateral compartment (Levels II–V): Jugular chain nodes
- Superior mediastinum (Level VII): Advanced disease
- PTC spreads preferentially to central nodes first
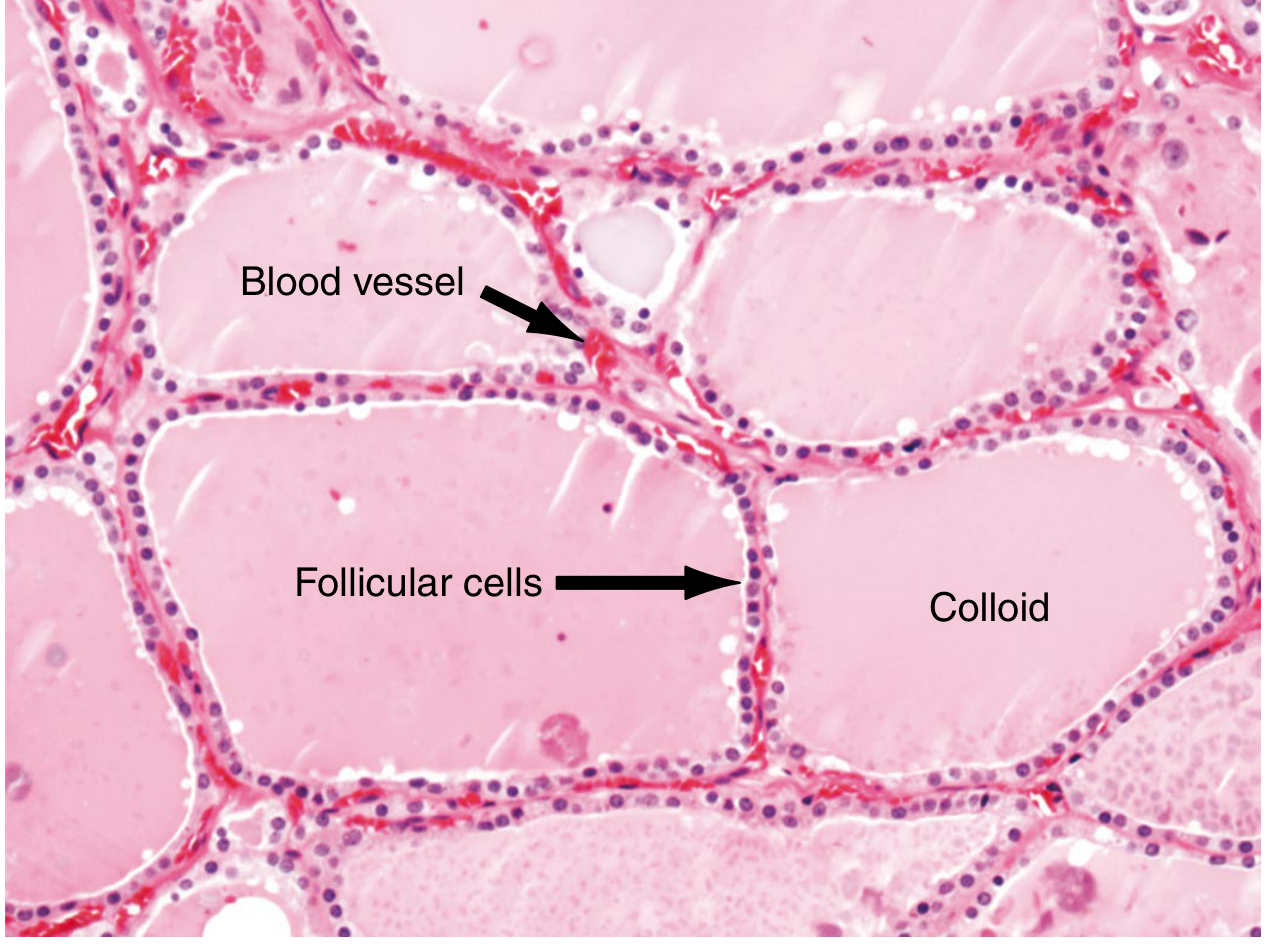
🔬 CHAPTER 3: Histology — What's Inside?
The thyroid parenchyma is built around follicles — the functional units:
Colloid (thyroglobulin storage)
↑↓ iodinated hormones
[ Follicular cells ] ← TSH-driven
↓
C-cells (parafollicular) → Calcitonin
- Follicular cells: Cuboidal epithelium; produce T4 and T3
- Colloid: Gelatinous center; the warehouse of thyroglobulin
- C-cells (parafollicular cells): Nestled between follicles; secrete calcitonin (calcium regulation)
- Stroma: Blood vessels, lymphatics, and nerves weave between follicles
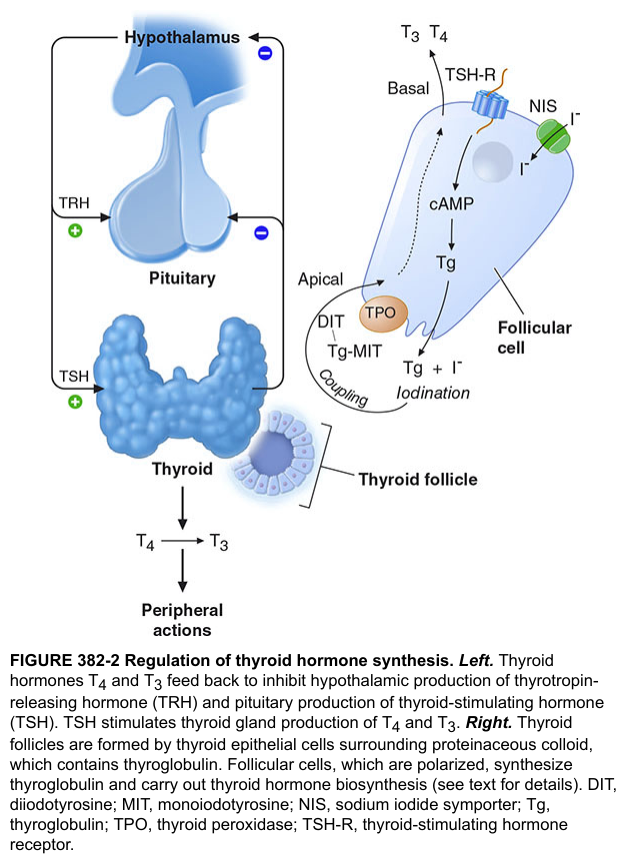
⚗️ CHAPTER 4: Physiology & Metabolism — The Hormone Factory
🏭 The HPT Axis — Command and Control
HYPOTHALAMUS
↓ TRH (Thyrotropin-Releasing Hormone)
ANTERIOR PITUITARY
↓ TSH (Thyroid-Stimulating Hormone)
THYROID GLAND
↓ T4 (Thyroxine) + T3 (Triiodothyronine)
PERIPHERAL TISSUES
↑ Negative feedback to Hypothalamus + Pituitary
🧪 The 7-Step Hormone Synthesis Factory
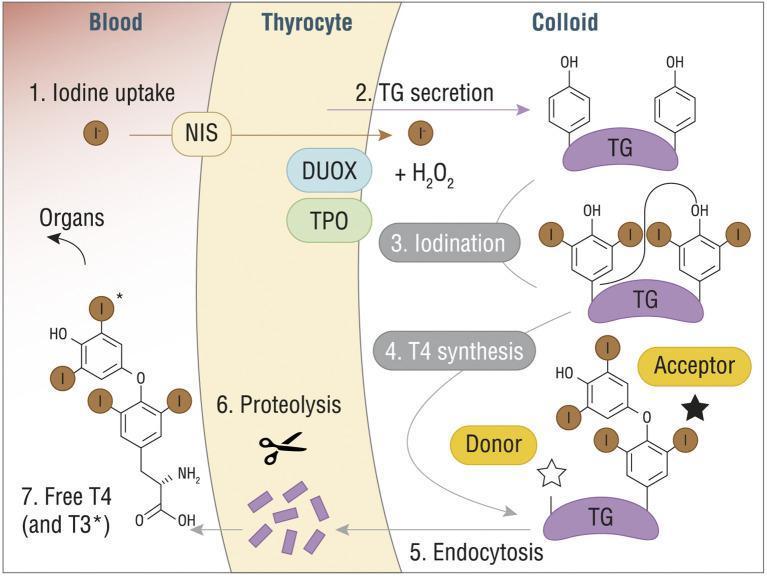
| Step | Process | Key Player |
|---|---|---|
| 1. Iodide Uptake | I⁻ actively transported into thyrocyte | NIS (Sodium-Iodide Symporter) |
| 2. TG Secretion | Thyroglobulin (TG) synthesized and secreted into colloid | Thyrocyte RER |
| 3. Organification | I⁻ oxidized → attached to tyrosine residues on TG → MIT, DIT | TPO + DUOX2 + H₂O₂ |
| 4. Coupling | MIT + DIT → T3; DIT + DIT → T4 | TPO-catalyzed coupling |
| 5. Endocytosis | Iodinated TG re-absorbed into thyrocyte | TSH-stimulated |
| 6. Proteolysis | Lysosomes cleave TG → release T3 and T4 | Lysosomal enzymes |
| 7. Secretion | Free T3 and T4 released into bloodstream | MCT8 transporter |
📌 Memory trick: "Nice Tigers Go Into Exciting Protein Stores" — NIS, TG, Organification, Iodination, Endocytosis, Proteolysis, Secretion
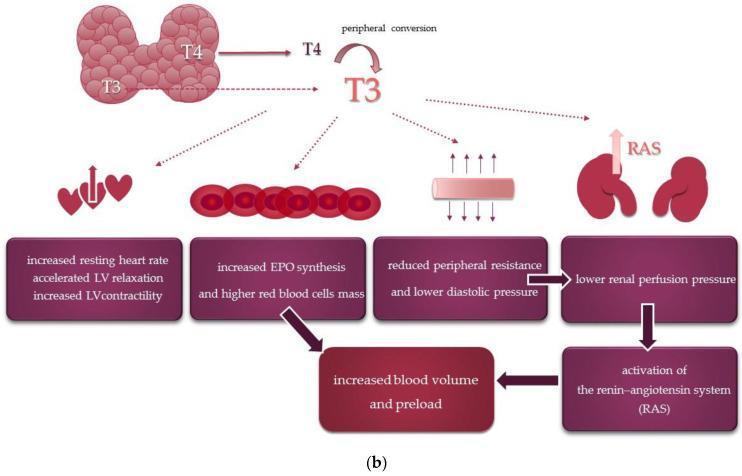
🩸 In the Bloodstream
- >99% of T4 and T3 are protein-bound (to TBG, albumin, transthyretin)
- <1% is free — the biologically active form
- T4:T3 ratio in circulation ≈ 20:1 (T4 produced more, but T3 is 4× more potent)
- Peripheral conversion: T4 → T3 via deiodinase enzymes (liver, brain, skeletal muscle)
- Average daily iodine requirement: 0.1 mg/day — entirely from diet (seafood, iodized salt)
⚡ What Thyroid Hormones Do — Actions on Every System
| System | Effect |
|---|---|
| Basal Metabolic Rate | ↑ ATP production, O₂ consumption, heat generation (calorigenic) |
| Cardiovascular | ↑ HR, ↑ contractility, ↑ cardiac output, ↓ peripheral resistance |
| CNS | Critical for fetal brain development; maintains adult cognition |
| Bone | Normal growth and ossification |
| Reproductive | Required for normal ovulation and fertility |
| GI | ↑ motility |
| Lipids | ↑ LDL clearance, ↑ lipolysis |
🤰 Special Physiological States
Pregnancy:
- Estrogen ↑ TBG → total T4 ↑ (but free T4 remains normal)
- hCG has TSH-like activity → mild TSH suppression in 1st trimester (normal)
- Iodine requirements increase by ~50%
- Fetal thyroid becomes autonomous by week 20
Euthyroid Sick Syndrome (Nonthyroidal Illness):
- Critically ill patients: ↓ T3, ↑ reverse T3 (rT3), normal/low TSH
- Body "downregulates" metabolism to conserve energy
- NOT true hypothyroidism → replacement therapy remains controversial
🌊 CHAPTER 5: Benign Thyroid Diseases
🥶 HYPOTHYROIDISM — When the Factory Slows Down
Classic symptoms: Cold intolerance · fatigue · weight gain · constipation · dry skin · myxedema (non-pitting edema) · bradycardia · "hung-up" deep tendon reflexes · menorrhagia · depression · periorbital puffiness
🔴 Hashimoto's Thyroiditis (Autoimmune Thyroiditis) — Most Common Cause
- Autoimmune destruction of follicular cells
- Anti-TPO antibodies (most sensitive, >95%) and anti-thyroglobulin antibodies
- Histology: lymphocytic infiltration with germinal center formation + Hürthle cell change
- May cause Hashitoxicosis (transient hyperthyroid phase early in disease)
- Increased risk of thyroid lymphoma (rare but important)
- Treatment: Levothyroxine (T4), titrated to TSH normalization
🟠 Subacute (de Quervain's) Thyroiditis
- Viral trigger (mumps, coxsackievirus, influenza)
- Painful thyroid, fever, markedly elevated ESR/CRP
- Classic triphasic course:
Phase 1 (Hyper, 4–8 weeks): Follicular destruction → hormone leak
↓
Phase 2 (Hypo, weeks to months): Depleted hormone stores
↓
Phase 3 (Euthyroid): Recovery in majority
- Treatment: NSAIDs (mild); steroids (severe); beta-blockers for symptoms
🟡 Riedel's Thyroiditis (Rarest)
- Fibrous replacement of thyroid → rock-hard, wood-like thyroid ("iron thyroid")
- Associated with IgG4-related systemic disease
- Can compress trachea and esophagus → stridor, dysphagia
- Treatment: Glucocorticoids, tamoxifen; surgery for decompression
⚫ Drug-Induced Hypothyroidism
| Drug | Mechanism |
|---|---|
| Amiodarone | Wolff-Chaikoff effect + cytotoxic thyroiditis + inhibits deiodinase |
| Lithium | Inhibits cAMP-dependent thyroid hormone formation |
| Methimazole / PTU | Directly inhibit T4/T3 synthesis (PTU also blocks peripheral T4→T3) |
| Sunitinib / Vandetanib (TKIs) | Destructive thyroiditis + ↓ VEGF-related vasculature + ↓ iodine uptake |
| Ipilimumab / Nivolumab / Pembrolizumab | Immune dysregulation → thyroiditis |
| Iodinated IV contrast / Amiodarone | Excess iodine load |
🔥 HYPERTHYROIDISM — When the Factory Overproduces
Classic symptoms: Heat intolerance · weight loss despite good appetite · palpitations · tremor · anxiety · diarrhea · atrial fibrillation · oligomenorrhea · exophthalmos (Graves' only) · pretibial myxedema (Graves' only)
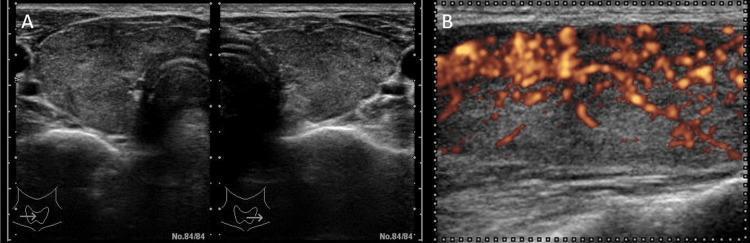
🔵 Graves' Disease — The Autoimmune Thyrotoxicosis
- Most common cause of hyperthyroidism (60–80%)
- TSH receptor antibodies (TRAb / TSI) stimulate TSH-R → uncontrolled T4/T3 production
- Classic triad: Hyperthyroidism + Exophthalmos + Pretibial myxedema
- Ultrasound: diffuse goiter with "thyroid inferno" pattern (intense hypervascularity on Doppler)
- F:M ratio ≈ 10:1; peak age 20–40

Management options for Graves':
| Modality | Details |
|---|---|
| Antithyroid drugs | Methimazole (1st line, except 1st trimester); PTU (1st trimester, thyroid storm) |
| Radioactive Iodine (RAI, I-131) | Destroys follicular cells; contraindicated in pregnancy; may worsen ophthalmopathy |
| Total thyroidectomy | Fastest cure; preferred in large goiters, pregnancy failure, suspicious nodules, severe ophthalmopathy |
| Beta-blockers | Propranolol — rapid symptom relief (palpitations, tremor); blocks T4→T3 conversion |
🟠 Toxic Multinodular Goiter (Plummer's Disease)
- Older patients; multiple autonomously functioning nodules
- Low TSH, elevated T4/T3
- Hot nodules on RAI scan
- Treatment: RAI preferred, or surgery if large/compressive
🟡 Solitary Toxic Adenoma
- Single hyperfunctioning nodule suppressing the rest of gland
- "Hot" nodule on scan; rest of gland "cold" (suppressed)
- Treatment: RAI or surgery (hemithyroidectomy)
⚡ Thyroid Storm (Thyrotoxic Crisis) — Medical Emergency
- Life-threatening exacerbation of hyperthyroidism
- Triggers: Surgery, infection, iodine load, trauma, childbirth
- Burch-Wartofsky score guides diagnosis (temp, CNS effects, GI, HR, CHF, precipitant)
- Treatment (the SSKI rule):
1. PTU (blocks synthesis + blocks T4→T3 conversion)
2. Iodine (Lugol's solution) — give 1 HOUR after PTU to avoid fueling synthesis
3. Steroids (dexamethasone — blocks T4→T3, treats adrenal insufficiency)
4. Beta-blockers (propranolol — controls HR, blocks T4→T3)
5. Cooling blankets, supportive ICU care
🏔️ GOITER — The Enlarged Thyroid
| Type | Features | Management |
|---|---|---|
| Endemic (diffuse) | Iodine deficiency; most preventable cause worldwide | Iodized salt |
| Nontoxic MNG | Multiple nodules, euthyroid; most common thyroid disease globally | Observe if asymptomatic; FNA suspicious nodules |
| Substernal goiter | Extends below thoracic inlet; may cause tracheal compression, SVC syndrome, Pemberton's sign | Surgery (sternotomy may be needed) |
🔍 THYROID NODULE — The Bump That Demands Attention
- Found in ~5% on palpation; up to 68% on ultrasound
- Majority (~95%) are benign
- Goal: identify the malignant ~5%
Workup Algorithm:
TSH
├── Low TSH → RAI scan
│ ├── Hot nodule → benign (Toxic adenoma) → treat hyperthyroidism
│ └── Cold nodule → 15–20% malignancy risk → FNA
└── Normal/High TSH → Ultrasound → TI-RADS score → FNA if indicated
ACR TI-RADS Scoring:
| Feature | Points |
|---|---|
| Composition (solid = most points) | 0–2 pts |
| Echogenicity (very hypoechoic = highest) | 0–3 pts |
| Shape (taller-than-wide) | +3 pts |
| Margin (lobulated/irregular/extrathyroidal) | 0–3 pts |
| Echogenic foci (punctate calcifications) | 0–3 pts |
→ TR1 (benign, 0 pts) through TR5 (high suspicion, ≥7 pts) → FNA threshold based on TR level and nodule size
Bethesda System for FNA Cytology Reporting:
| Category | Malignancy Risk | Management |
|---|---|---|
| I – Nondiagnostic | 1–4% | Repeat FNA with US guidance |
| II – Benign | 0–3% | Ultrasound follow-up |
| III – Atypia of undetermined significance (AUS) | 10–30% | Repeat FNA or molecular testing |
| IV – Follicular neoplasm | 25–40% | Diagnostic hemithyroidectomy |
| V – Suspicious for malignancy | 50–75% | Near-total or total thyroidectomy |
| VI – Malignant | 97–99% | Total thyroidectomy |
📌 Molecular testing (ThyroSeq v3, Afirma Gene Expression Classifier) reclassifies indeterminate Bethesda III/IV nodules — reducing unnecessary surgeries.
🦀 CHAPTER 6: Malignant Thyroid Diseases — The Dark Side
The Thyroid Cancer Family Tree
Thyroid Cancers
├── Differentiated (90–95%)
│ ├── Papillary (PTC) — 80–85%
│ └── Follicular (FTC) — 10–15%
│ └── Hürthle cell carcinoma (oxyphilic variant)
├── Medullary (MTC) — 3–5% [from C-cells, NOT follicular cells]
└── Anaplastic (ATC) — <2% [most lethal cancer in the body]

📌 1. PAPILLARY THYROID CARCINOMA (PTC) — The "Good" Cancer
Epidemiology: 80–85% of thyroid cancers; peak age 30–50; F:M = 3:1; rising globally
Key features:
- Arises from follicular epithelial cells
- Spreads via lymphatics → cervical lymph nodes (common, but doesn't significantly worsen prognosis)
- BRAF V600E mutation in ~60% (most common driver mutation)
- RET/PTC rearrangements — especially after radiation exposure (e.g., Chernobyl)
- Excellent prognosis: 10-year survival >95%
Histological Hallmarks — The "Nuclear Signatures":
| Feature | Description |
|---|---|
| Orphan Annie eye nuclei | Large, optically clear/ground-glass nuclei |
| Nuclear grooves | "Coffee bean" appearance |
| Intranuclear inclusions | Eosinophilic cytoplasmic invaginations |
| Psammoma bodies | Calcified concentric lamellations — pathognomonic for PTC |
| Papillary architecture | Fibrovascular cores lined by tumor cells |
📌 Mnemonic for PTC nuclei: "GOI-P" — Grooves, Orphan Annie eyes, Inclusions, Psammoma bodies
Important PTC Variants:
| Variant | Behavior |
|---|---|
| Classic PTC | Best prognosis |
| Follicular variant (FVPTC) | Follicular architecture, PTC nuclei; encapsulated variant = excellent prognosis |
| Tall cell variant (>30% tall cells) | Aggressive; BRAF+ common; worse prognosis |
| Columnar cell variant | Very aggressive; distant mets common |
| Diffuse sclerosing variant | Young patients; extensive lymph node spread |
| Papillary microcarcinoma (<1 cm) | Often incidental; active surveillance possible |
Risk Stratification & Management of PTC:
| Risk Category | Features | Surgery | RAI | TSH Target |
|---|---|---|---|---|
| Low | T1–T2, no ETE, no mets, favorable histology | Hemi- or total thyroidectomy | Not routinely recommended | 0.5–2 mU/L |
| Intermediate | Microscopic ETE, vascular invasion, multifocal | Total thyroidectomy | Consider (30–100 mCi) | 0.1–0.5 mU/L |
| High | T4, M1, aggressive histology, incomplete resection | Total thyroidectomy + neck dissection | Yes (100–200 mCi) | <0.1 mU/L |
📌 2. FOLLICULAR THYROID CARCINOMA (FTC)
Key features:
- 2nd most common; peak age 40–60; F:M = 3:1
- RAS mutations most common; PAX8-PPARγ fusion in 30–40%
- Spreads hematogenously → lung ("cannonball" mets), bone (osteolytic)
- Unlike PTC, lymph node spread is uncommon
- Cannot be diagnosed on FNA — requires histological evidence of capsular or vascular invasion
Diagnosis dilemma:
FNA → Bethesda IV (follicular neoplasm)
↓
Diagnostic hemithyroidectomy
↓
Histology: capsular/vascular invasion = FTC
No invasion = Follicular adenoma (benign)
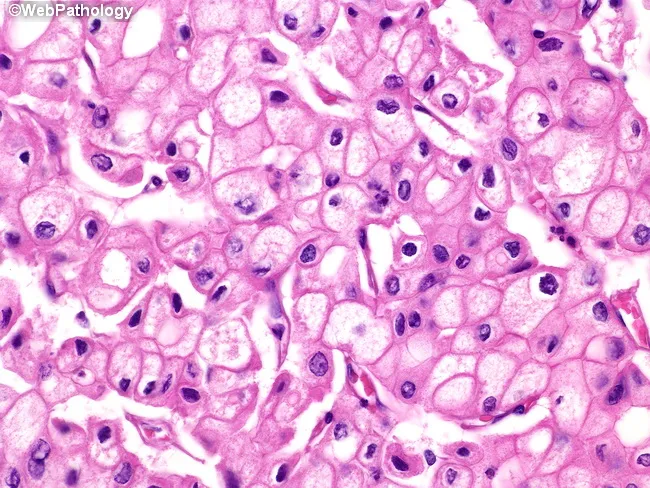
Hürthle Cell (Oncocytic) Carcinoma:
- Variant with oxyphilic/granular cytoplasm
- More aggressive; poor RAI uptake (less iodine-avid)
- Higher rates of lymph node and distant metastases
- Treat similarly to FTC but systemic therapy often needed earlier
Management: Total thyroidectomy → RAI if intermediate/high risk → TSH suppression → Tg surveillance
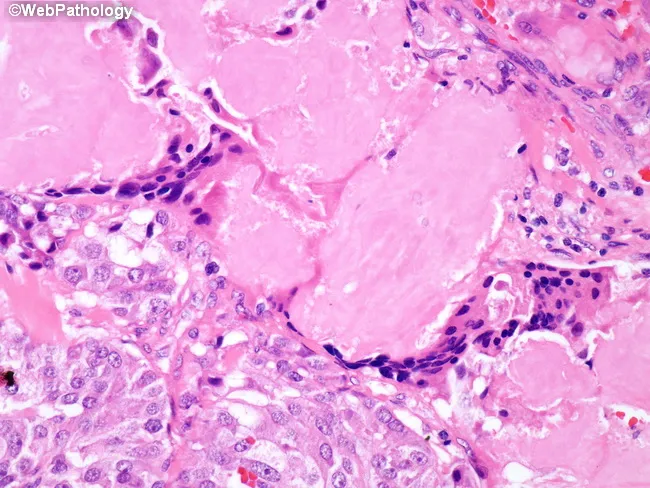
📌 3. MEDULLARY THYROID CARCINOMA (MTC) — The C-Cell Rebel
Origin: Parafollicular C-cells → secretes calcitonin (NOT T3/T4)
Epidemiology: 3–5% of thyroid cancers
- 75% sporadic (single focus, no family history)
- 25% hereditary (autosomal dominant — RET proto-oncogene mutation)
Hereditary MTC Syndromes:
| Syndrome | Components | RET Codon |
|---|---|---|
| MEN2A (most common) | MTC + Pheochromocytoma + Hyperparathyroidism | Codon 634 (most common) |
| MEN2B | MTC + Pheo + Marfanoid habitus + Mucosal neuromas + Megacolon | Codon 918 (most aggressive) |
| Familial MTC (FMTC) | MTC only; best prognosis | Various codons |
⚠️ Critical rule: ALWAYS screen for pheochromocytoma (plasma metanephrines) BEFORE thyroid surgery in MEN2 — operating without this can precipitate a fatal hypertensive crisis!
Tumor markers:
- Serum calcitonin — most sensitive diagnostic and surveillance marker
- CEA — correlates with tumor burden; rising CEA with stable calcitonin suggests dedifferentiation
Histology: Sheets/nests of polygonal cells with amyloid stroma (calcitonin-derived; Congo red positive → apple-green birefringence under polarized light)
Management of MTC:
| Situation | Action |
|---|---|
| All MTC patients | RET genetic testing + family screening |
| Sporadic/hereditary MTC | Total thyroidectomy + central neck dissection (Level VI) |
| Hereditary RET mutation carrier (prophylactic) | Thyroidectomy age based on mutation risk: MEN2B (age <6 months!), codon 634 (<5 yrs), others (<10 yrs) |
| Locally advanced / unresectable | Surgery + vandetanib or cabozantinib (RET kinase inhibitors) |
| Distant metastases | Selpercatinib or pralsetinib (highly selective RET inhibitors; dramatic response rates) |
| Post-op surveillance | Calcitonin + CEA every 6 months; structural imaging if rising |
📌 4. ANAPLASTIC THYROID CARCINOMA (ATC) — The Monster
Epidemiology: <2% of thyroid cancers but ~50% of thyroid cancer deaths
Key features:
- Peak age >60; median survival 3–6 months from diagnosis
- Often arises from dedifferentiation of pre-existing PTC or FTC (p53 loss + BRAF mutations)
- Presents with rapidly enlarging, fixed, hard neck mass
- Symptoms at presentation: stridor, dysphagia, hoarseness, SVC syndrome
Histology: Undifferentiated — giant cells, spindle cells, squamoid cells; necrosis, high mitotic index
Staging: All ATC = Stage IV by definition (IVA = intrathyroidal, IVB = extrathyroidal, IVC = distant mets)
Management (multimodal and time-sensitive):
| Modality | Role |
|---|---|
| BRAF V600E testing | First step! Present in ~25–45% of ATC |
| Dabrafenib + Trametinib (BRAF+MEK inhibitors) | BRAF V600E+ ATC — response rates up to 69%, some durable remissions — game-changer! |
| Surgery | R0 resection if technically feasible in Stage IVA only |
| External beam radiation (EBRT) | Accelerated hyperfractionation; often combined with chemotherapy |
| Chemotherapy | Doxorubicin + cisplatin (modest benefit) |
| Immunotherapy | Pembrolizumab (PD-L1 positive tumors) showing promise |
| Lenvatinib | VEGFR inhibitor for progressive disease |
| Multidisciplinary team | Endocrine surgery + oncology + radiation oncology + palliative care from day 1 |
🔪 CHAPTER 7: Thyroid Surgery — The Grand Finale
Surgical Procedures & Indications
| Procedure | Indication |
|---|---|
| Hemithyroidectomy (lobectomy + isthmusectomy) | Bethesda IV, solitary low-risk PTC ≤4 cm, diagnostic |
| Total thyroidectomy | Graves', compressive MNG, PTC ≥4 cm, bilateral disease, MTC |
| Central neck dissection (Level VI) | MTC (always), PTC with clinically positive central nodes |
| Lateral neck dissection (Levels II–V) | Biopsy-proven lateral node metastases |
| Completion thyroidectomy | When hemithyroidectomy reveals cancer requiring total removal |
⚠️ Complications of Thyroidectomy
| Complication | Structure | Timing | Management |
|---|---|---|---|
| Hoarseness | RLN (unilateral injury) | Immediate | Monitor; most temporary; voice therapy |
| Bilateral vocal cord paralysis | RLN (bilateral injury) | Immediate | Re-intubation, tracheostomy |
| Hypocalcemia / Tetany | Parathyroids removed/devascularized | 24–48 hrs post-op | IV calcium gluconate → oral Ca²⁺ + Vit D |
| Post-op hematoma | Thyroid vessels | First 6–12 hrs | Airway emergency; return to OR immediately |
| High-pitched voice loss | EBSLN | Immediate | Often permanent; dysphonia |
| Hypothyroidism | Total thyroidectomy | Weeks | Lifelong levothyroxine |
☢️ Radioactive Iodine (RAI / I-131) Therapy
Mechanism: I-131 is avidly concentrated in thyroid follicular cells → emits β-radiation → destroys thyroid tissue
Indications post-thyroidectomy:
- High-risk DTC (T4, M1, aggressive histology)
- Intermediate-risk (multifocal disease, microscopic vascular invasion)
Pre-RAI preparation:
- Raise TSH to >30 mU/L (either thyroid hormone withdrawal for 4–6 weeks OR rhTSH — Thyrogen injection — much better tolerated)
- Low-iodine diet for 2 weeks prior (maximizes uptake)
- Avoid iodinated contrast within 6–8 weeks
Post-RAI surveillance:
- Thyroglobulin (Tg): Tumor marker for DTC; should become undetectable after successful ablation
- Rising Tg → structural recurrence workup (neck ultrasound → CT/PET-CT)
- Anti-TG antibodies interfere with Tg measurement — monitor trend
💊 Systemic Targeted Therapies for Advanced Thyroid Cancer
| Drug | Target | Cancer |
|---|---|---|
| Lenvatinib | VEGFR 1–3, FGFR, PDGFR | Radioiodine-refractory DTC (1st line) |
| Sorafenib | VEGFR, RAF | Radioiodine-refractory DTC (alternative) |
| Vandetanib | RET, VEGFR, EGFR | MTC |
| Cabozantinib | RET, MET, VEGFR | MTC (2nd line) |
| Selpercatinib | RET (highly selective) | RET-mutant MTC + PTC |
| Pralsetinib | RET (highly selective) | RET-mutant MTC |
| Dabrafenib + Trametinib | BRAF V600E + MEK | BRAF+ ATC (breakthrough) |
📊 CHAPTER 8: Thyroid Biomarkers — The Laboratory Compass
| Marker | Interpretation |
|---|---|
| TSH | Master regulator; best screening test; ↓ in hyper, ↑ in hypo |
| Free T4 | Confirms thyroid status; use alongside TSH |
| Free T3 | Useful in T3-toxicosis (elevated T3, normal T4) |
| Anti-TPO antibodies | Hashimoto's marker (>95% sensitive) |
| Anti-thyroglobulin antibodies | Hashimoto's; interferes with Tg measurement! |
| TSI / TRAb | Graves' disease marker (>95% sensitivity for active disease) |
| Thyroglobulin (Tg) | Post-thyroidectomy tumor marker for DTC surveillance |
| Calcitonin | MTC diagnostic + surveillance marker; extremely sensitive |
| CEA | Correlates with MTC tumor burden; prognostic value |
🎓 QUICK RECALL MNEMONICS
| Topic | Mnemonic |
|---|---|
| Thyroid hormone synthesis steps | "Nice Tigers Go Into Exciting Protein Stores" → NIS · TG · Organification · Iodination · Endocytosis · Proteolysis · Secretion |
| PTC nuclear features | "GOI-P" → Grooves · Orphan Annie eyes · Inclusions · Psammoma bodies |
| MEN2A triad | "MTC + Pheo + Parathyroid" |
| RLN danger area | "Recurrent Lies Near" the inferior thyroid artery crossing |
| Embryology timeline | "3 thickens · 5 solidifies · 7 descends · 10 functions" |
| Bethesda → Management | "No · Benign · Atypia · Follicular · Suspicious · Malignant" → Watch · Watch · Repeat · Hemi · Total · Total |
| Thyroid storm treatment | "PTU first, then iodine 1 hour LATER, Steroids, Beta-blockers" |
| C-cell tumors | "MTC = Calcitonin + Amyloid + RET + MEN2" |
🎯 MASTER COMPARISON TABLE: All 4 Thyroid Cancers
| Feature | PTC | FTC | MTC | ATC |
|---|---|---|---|---|
| Frequency | 80–85% | 10–15% | 3–5% | <2% |
| Cell of origin | Follicular cell | Follicular cell | C-cell (parafollicular) | Undifferentiated |
| Key mutation | BRAF V600E | RAS, PAX8-PPARγ | RET | BRAF/p53 |
| Spread route | Lymphatic | Hematogenous | Both | Both (aggressive) |
| Tumor marker | Thyroglobulin | Thyroglobulin | Calcitonin + CEA | None reliable |
| FNA diagnosis? | Yes | No (needs histology) | Yes | Yes |
| RAI uptake | Yes | Yes | No | No |
| 10-year survival | >95% | ~85% | ~75% | <10% |
| Key treatment | Surgery ± RAI | Surgery ± RAI | Surgery + RET inhibitors | Surgery + Dabrafenib/Trametinib |
🏆 The 10 Golden Clinical Pearls
- 🥇 TSH is the single best thyroid screening test — always start here before any other test
- 🥇 A "cold" thyroid nodule on RAI scan carries 15–20% malignancy risk → needs FNA
- 🥇 FNA cannot diagnose follicular carcinoma — you need histology showing capsular/vascular invasion
- 🥇 All MTC patients need RET gene testing → screen family members if positive
- 🥇 Always rule out pheochromocytoma before thyroid surgery in MEN2 — hypertensive crisis can be fatal
- 🥇 Lingual thyroid may be the patient's only thyroid — confirm with RAI scan before any removal
- 🥇 Anti-TPO antibodies + hypothyroid symptoms = Hashimoto's — no biopsy needed
- 🥇 Thyroglossal duct cyst moves on tongue protrusion and swallowing — pathognomonic sign
- 🥇 Rising Tg after thyroidectomy = recurrence until proven otherwise — investigate immediately
- 🥇 BRAF V600E in ATC = test immediately; dabrafenib + trametinib can be life-saving
Sources: Sabiston Textbook of Surgery, 21st Edition · Schwartz's Principles of Surgery, 11th Edition · Harrison's Principles of Internal Medicine, 21st Edition · Katzung's Basic and Clinical Pharmacology, 16th Edition · Mulholland & Greenfield's Surgery, 7th Edition
This is a shared conversation. Sign in to Orris to start your own chat.