HCG harmone
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Excellent - I have comprehensive information from multiple authoritative textbooks. Here is a complete overview of HCG:
Human Chorionic Gonadotropin (hCG)
Structure
hCG is a glycoprotein hormone with a molecular weight of ~39,000 Da. It contains galactose and hexosamine sugar residues, and consists of two non-covalently linked subunits held together by disulfide bonds:
- Alpha (α) subunit (MW ~18,000): identical to the α subunits of LH, FSH, and TSH - this is why hCG cross-reacts with LH receptors
- Beta (β) subunit (MW ~28,000): unique to hCG - gives it its specificity; used as the target in pregnancy tests
Trophoblast cells can also produce "nicked" hCG (hCGn) - a partially degraded form missing peptide bonds between amino acids 44-45 or 47-48 - as well as free α and β subunits separately.
Source: Synthesized and secreted by the syncytial trophoblast cells of the placenta.
- Guyton and Hall Textbook of Medical Physiology, p. 1037
- Ganong's Review of Medical Physiology, 26th Ed.
Secretion Pattern in Pregnancy
hCG can first be measured in the blood 8-9 days after ovulation, shortly after blastocyst implantation. The exponential rise after implantation has a doubling time of approximately 30.9 ± 3.7 hours.
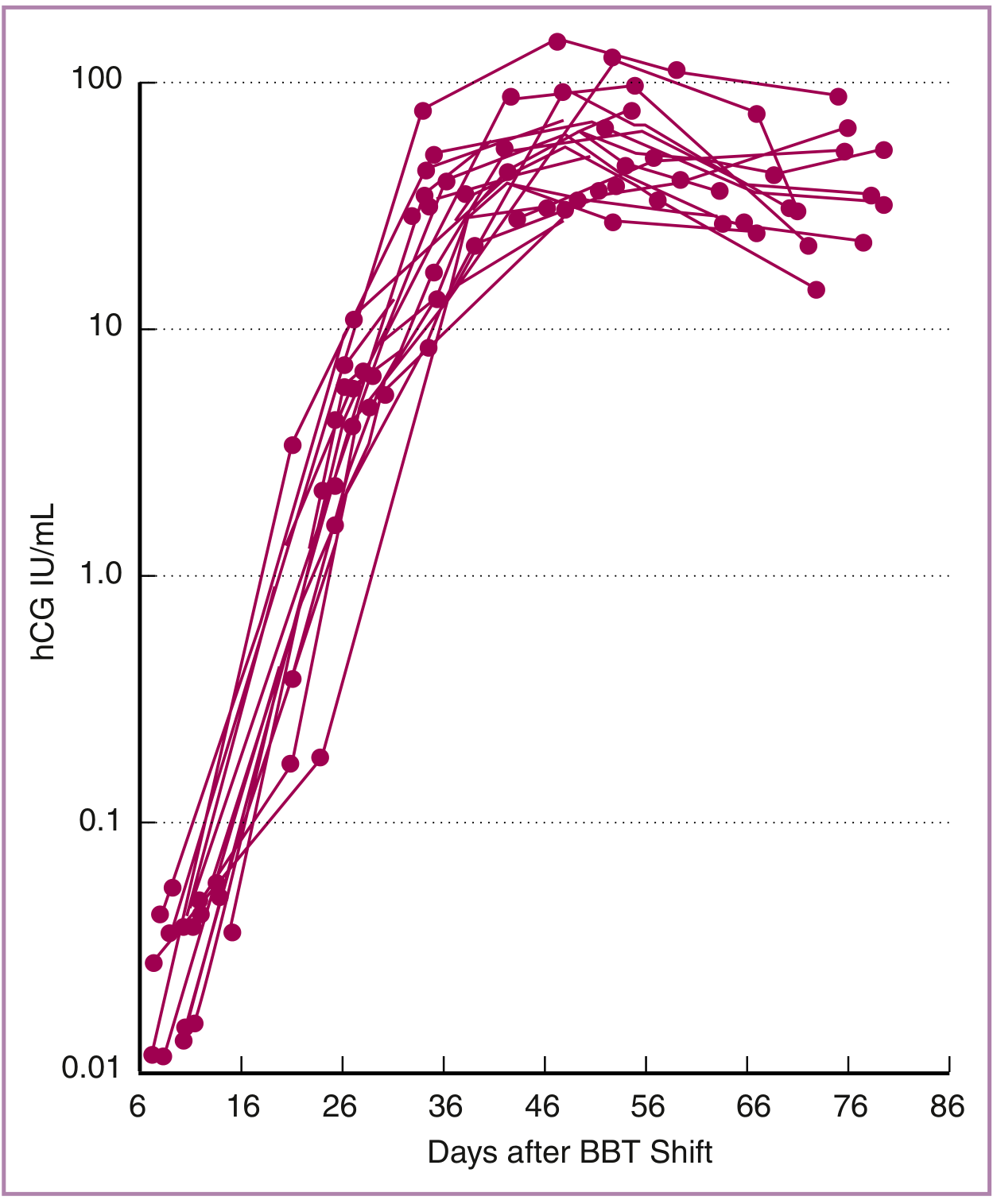
Figure: Levels of hCG (IU/mL) after implantation - rise is exponential in the first trimester, plateauing between 11-12 weeks' gestation. (From Creasy & Resnik's Maternal-Fetal Medicine)
| Timepoint | hCG Level |
|---|---|
| 8-9 days post-ovulation | First detectable in blood |
| 14 days post-conception | May be detectable in urine |
| 10-12 weeks | Peak level |
| 16-20 weeks | Declines to lower plateau |
| Remainder of pregnancy | Maintained at lower level |
- Creasy & Resnik's Maternal-Fetal Medicine
- Guyton and Hall Textbook of Medical Physiology, p. 1037
Functions
1. Corpus Luteum Rescue (Primary Function)
The most critical role: hCG prevents involution of the corpus luteum at the end of the monthly female sexual cycle. Instead, it causes the corpus luteum to:
- Grow to ~twice its initial size within the first month
- Secrete larger quantities of progesterone and estrogens for the next several months
- These hormones maintain the decidual endometrium and prevent menstruation
If the corpus luteum is removed before ~7 weeks of pregnancy, spontaneous abortion almost always occurs. After ~13-17 weeks, the placenta takes over progesterone/estrogen production and the corpus luteum involutes.
2. Maintenance of Early Pregnancy
hCG rescues the corpus luteum from premature demise (luteolysis) while maintaining progesterone production. Immunoneutralization of hCG results in early pregnancy loss.
3. Fetal Testicular Stimulation (Male Fetuses)
hCG exerts an interstitial (Leydig) cell-stimulating effect on the fetal testes, causing testosterone production in male fetuses until birth. This testosterone:
- Drives development of male sex organs (instead of female)
- Near term, causes testicular descent into the scrotum
4. Thyroid Stimulation
Due to structural similarity with TSH, very high hCG levels can mildly stimulate the thyroid - explaining the gestational hyperthyroidism sometimes seen in hyperemesis gravidarum or molar pregnancies.
- Guyton and Hall Textbook of Medical Physiology, p. 1037-1038
- Color Atlas of Human Anatomy, Vol. 2, p. 610
Relationship to LH
hCG is primarily luteinizing and luteotropic with little FSH activity. It acts on the same receptor as LH (LH/hCG receptor). This shared receptor explains why:
- hCG can substitute for LH in triggering ovulation in ART protocols
- hCG has a longer half-life than LH, making it preferred clinically
Clinical Applications
Diagnostic Uses
| Use | Basis |
|---|---|
| Pregnancy testing | hCG detected in urine/serum (urine-based OTC kits target the unique β subunit) |
| Ectopic pregnancy | hCG doubling every ~48h in normal pregnancy; slower rise or plateau suggests ectopic; failure to see intrauterine gestational sac when hCG ≥1,100-1,500 mU/mL is suspicious |
| Molar pregnancy | Higher than normal hCG levels |
| Down syndrome screening | Elevated hCG (part of double/triple/quad marker screen combined with AFP, uE3) |
| Tumor marker | Elevated in choriocarcinoma, testicular germ cell tumors, and some GI/pancreatic tumors |
Therapeutic Uses
-
Ovulation induction in ART (acts as the LH surge trigger)
-
Hypogonadism - stimulates testosterone production in males
-
Preparations: urine-derived (IM only due to local reactions) or recombinant hCG (choriogonadotropin alfa) - the predominant clinical preparation today
-
Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 954
hCG as a Tumor Marker
| Tumor Type | hCG Elevation Pattern |
|---|---|
| Choriocarcinoma / Trophoblastic tumors | Intact hCG markedly elevated |
| Nonseminomatous germ cell tumors (NSGCT) | >60% have elevated free β-hCG |
| Seminoma | 10-30% elevated; contains both intact hCG and free β or free α subunits equally |
| Other cancers (e.g., urothelial) | ~30% show ectopic free β-hCG production |
| Pancreatic endocrine tumors | Ectopic α-hCG is a marker of malignancy |
The free β subunit is particularly useful for detecting recurrence/metastasis of choriocarcinoma when intact hCG remains normal.
- Henry's Clinical Diagnosis and Management by Laboratory Methods
Summary Table
| Property | Detail |
|---|---|
| Type | Glycoprotein |
| Produced by | Syncytial trophoblast (placenta) |
| Structure | α + β heterodimer (α shared with LH/FSH/TSH) |
| MW | ~39,000 Da |
| Receptor | Same as LH (LH/hCG receptor) |
| Peak in pregnancy | 10-12 weeks gestation |
| First detectable | 8-9 days post-ovulation (blood); ~14 days (urine) |
| Primary function | Corpus luteum rescue / progesterone maintenance |
| Key clinical use | Pregnancy test, ovulation trigger, tumor marker |
This is a shared conversation. Sign in to Orris to start your own chat.