Methods of cervical screening. Describe.
Reading File
Finding Sources
Searching PubMed
"cervical cancer screening" AND "methods"
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, high-quality information from multiple authoritative textbooks. Let me compile the full answer.
Methods of Cervical Screening
Cervical cancer is largely preventable because it develops from precursor lesions (CIN) over many years, giving a wide window for detection. Screening has reduced cervical cancer incidence by ~79% and mortality by ~70% since 1950. - Berek & Novak's Gynecology, p. 845
1. Conventional Cervical Cytology (Conventional Pap Smear)
The original Papanicolaou (Pap) test involves circumferentially scraping the transformation zone of the cervix with a spatula or brush, then smearing and fixing cells directly onto a glass slide for staining and microscopic examination.
Limitations:
- Only 10-20% of collected cells are transferred to the slide
- Air-drying artefact distorts cellular morphology
- Slide may be obscured by blood, mucus, or vaginal discharge
- Sensitivity for detecting CIN 2/3: 47-62%; specificity: 60-95%
- Overall false-negative rate: ~49%
- Sampling errors, preparation errors, and interpretive errors all contribute to missed cases
More than half of all invasive cervical cancer cases occur in women who were never screened or underscreened. - Berek & Novak's Gynecology, p. 845
2. Liquid-Based Cytology (LBC)
LBC was developed to overcome the limitations of conventional cytology and is now the standard in most high-income countries.
Technique:
- Cells are collected with an endocervical brush + plastic spatula, or a plastic broom
- The device is rinsed directly into a vial of liquid alcohol-based preservative (e.g., ThinPrep, SurePath)
- 80-90% of cells are transferred to the preservative (vs. 10-20% with conventional smears)
- The liquid is passed through a filter, trapping larger epithelial cells and separating them from blood and inflammatory cells
- A thin, uniform monolayer of well-preserved cells is deposited on the slide
Advantages over conventional cytology:
- Eliminates air-drying artefact
- Reduces unsatisfactory samples by 70-90%
- Residual material in the vial can be used for reflex HPV testing - no second visit required
- Berek & Novak's Gynecology, p. 845-846
3. Automated Image-Guided Slide Screening (Computer-Assisted Cytology)
An FDA-approved adjunct for primary screening and rescreening of cytology samples initially interpreted as normal.
How it works:
- An automated microscope coupled to a digital camera scans the entire slide
- Computer algorithms analyze each field of view and rank the slide by probability of containing an abnormality
- High-probability slides are then reviewed by a cytotechnologist or cytopathologist
Performance: Reduces the false-negative rate by 32% compared to unassisted cytology. - Berek & Novak's Gynecology, p. 846
4. HPV DNA/RNA Testing
Since 93-100% of squamous cell cervical cancers contain DNA from high-risk HPV strains, molecular HPV testing targets the root cause of the disease.
Characteristics:
- Higher sensitivity but lower specificity than cytology
- Not recommended as a standalone test in women under 30 (high prevalence of transient HPV infection makes results non-specific)
- HPV 16 and 18 carry the highest cancer risk and can be specifically genotyped
FDA-approved assays and their clinical roles:
| Assay | Target | Key Indications |
|---|---|---|
| Hybrid Capture 2 | DNA (genomic) | ASC-US triage, Co-test |
| Cervista | DNA (Invader Technology) | ASC-US triage, Co-test |
| Cobas HPV (PCR TaqMan) | L1 DNA | ASC-US triage, Co-test, Primary screening |
| APTIMA | E6/E7 mRNA | ASC-US triage, Co-test, Primary screening |
Berek & Novak's Gynecology, p. 846
HPV testing can be used in three clinical contexts:
- Triage of equivocal cytology (ASC-US) - to determine which women need colposcopy
- Co-testing - simultaneous cytology + HPV, particularly for women ≥30
- Primary HPV screening - standalone first-line test (Cobas/APTIMA), with reflex cytology for positives
5. Co-Testing (Cytology + HPV)
Combining Pap cytology with HPV testing provides higher sensitivity than either test alone.
- Recommended for women ≥30 years
- Women negative for both tests can extend screening interval to every 5 years
- Women with normal cytology but positive for high-risk HPV DNA should repeat cervical cytology every 6-12 months
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 926
6. Colposcopy (Diagnostic Follow-Up, Not Primary Screening)
When any screening test is abnormal, colposcopy is performed:
- The cervix is examined under magnification after applying acetic acid
- Abnormal epithelium appears as aceto-white areas
- Abnormal areas are biopsied for histological confirmation
- Robbins Pathologic Basis of Disease, p. 926
Cytological Appearances on Pap Smear
The following image illustrates the spectrum of cervical cytological changes:
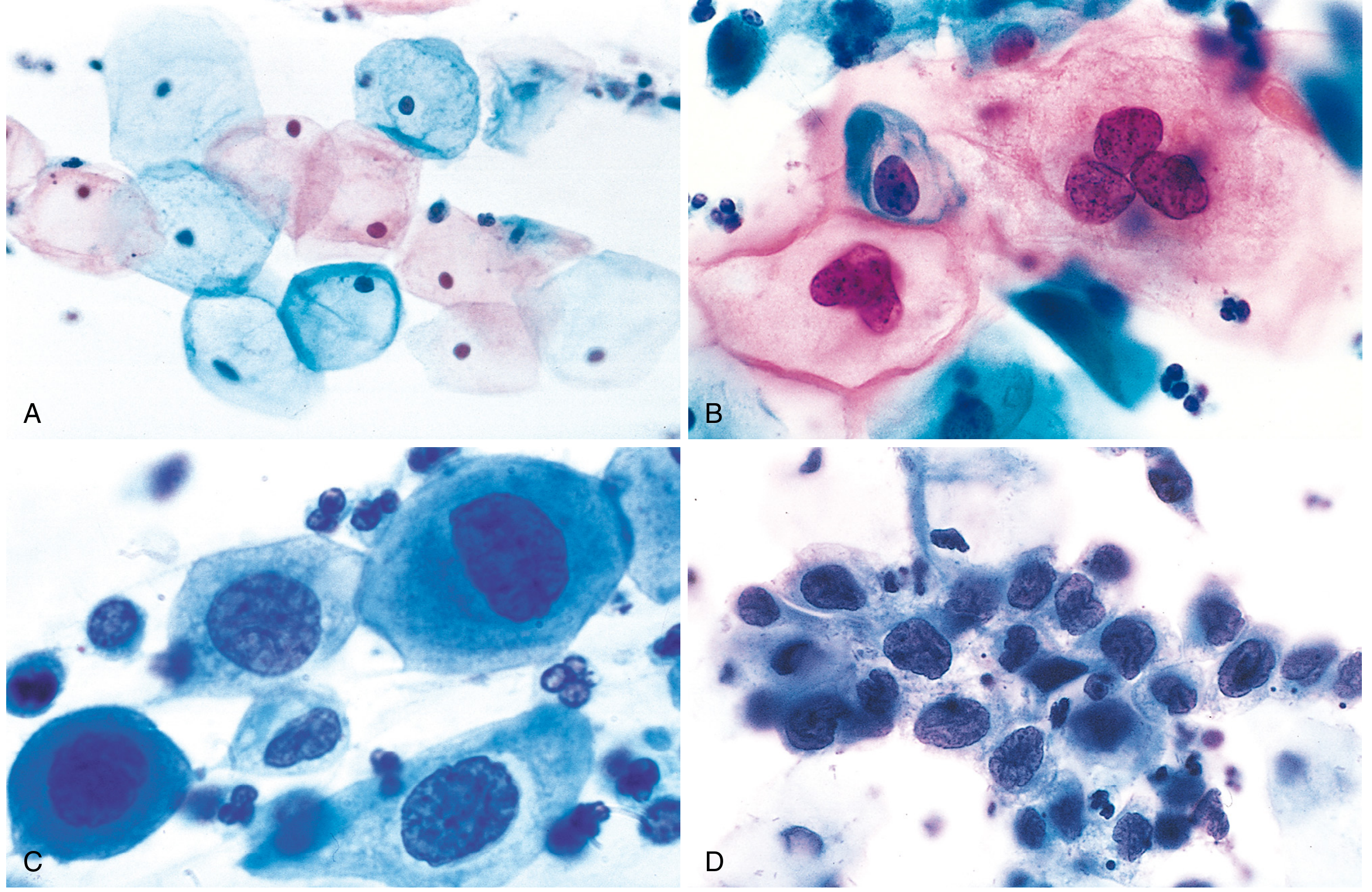
(A) Normal exfoliated superficial squamous cells - abundant cytoplasm, small regular nuclei
(B) LSIL - koilocytes (HPV cytopathic effect): large perinuclear halo, irregular nuclear membrane
(C & D) HSIL - progressive reduction in cytoplasm, increasing nucleus-to-cytoplasm ratio, nuclear hyperchromasia - reflecting loss of cellular differentiation
The Bethesda Classification of Cervical Cytology
Screening results are reported using the Bethesda System:
- NILM - Negative for intraepithelial lesion or malignancy (normal)
- Squamous cell abnormalities:
- ASC-US - Atypical squamous cells of undetermined significance
- ASC-H - Atypical squamous cells, cannot exclude HSIL
- LSIL - Low-grade squamous intraepithelial lesion
- HSIL - High-grade squamous intraepithelial lesion
- Squamous cell carcinoma
- Glandular cell abnormalities:
- AGC (Atypical glandular cells)
- AIS (Endocervical adenocarcinoma in situ)
- Adenocarcinoma
Symptom to Diagnosis: An Evidence-Based Guide, 4th Ed.
Screening Intervals (ACOG Guidelines)
| Age Group | Recommended Method | Interval |
|---|---|---|
| < 21 years | No screening | - |
| 21-29 years | Cytology alone | Every 2-3 years |
| 30-65 years | Co-testing (preferred) | Every 5 years |
| 30-65 years | Cytology alone | Every 3 years |
| > 65 years | Can discontinue if 3 consecutive normal Paps or 2 normal co-tests in 10 years | - |
| Post-hysterectomy (benign indication, no CIN history) | Discontinue | - |
More frequent screening (annually) is recommended for: HIV-positive women, immunosuppressed women, DES daughters, and those with history of CIN 2+. - Berek & Novak's Gynecology, p. 846-847
Summary Comparison
| Method | Sensitivity (CIN 2+) | Specificity | Key Role |
|---|---|---|---|
| Conventional Pap | 47-62% | 60-95% | Historical standard |
| Liquid-based cytology | Similar/slightly better | Similar | Current standard cytology |
| HPV DNA testing | Higher | Lower | Primary screen / co-test / ASC-US triage |
| Co-testing | Highest combined | Moderate | Gold standard for ≥30 years |
| Automated image analysis | Reduces FN by 32% | Improved | Adjunct to cytology |
Recent evidence note: A 2023 systematic review (PMID 37533074) examined DNA methylation as a triage marker for colposcopy referral in HPV-based screening, representing an emerging molecular approach that may refine triage of HPV-positive women beyond current genotyping strategies.
This is a shared conversation. Sign in to Orris to start your own chat.