Peters anomaly
Reading File
Finding Sources
Searching PubMed
Peters anomaly anterior segment dysgenesis
Reading File
Finding Sources
Finding Sources
Searching Images
Peters anomaly corneal opacity anterior segment
Reading File
Loading Image
Reading File
Finding Sources
I now have comprehensive information from both Kanski and the Wills Eye Manual. Let me compile the full answer.
Peters Anomaly
Definition & Epidemiology
Peters anomaly is a rare congenital anterior segment dysgenesis characterized by a central corneal opacity (leukoma) resulting from defective neural crest cell migration during fetal development. It is bilateral in >50% of cases. Most cases are sporadic, though autosomal recessive inheritance is described.
Pathogenesis
The underlying defect is failure of the lens to completely detach from the surface ectoderm during weeks 4–7 of gestation, leading to a posterior corneal defect involving the posterior stroma, Descemet membrane, and endothelium. This results in the characteristic central corneal scar.
Classification
| Type | Features |
|---|---|
| Type I | Corneal opacity only; iris strands extend from the collarette to the posterior corneal defect; lens is clear and normally positioned |
| Type II | Corneal + lens involvement; lens may be cataractous, anteriorly displaced (shallow anterior chamber), or directly adherent to the corneal defect (keratolenticular adhesion) |
Clinical Features
- Central corneal opacity of variable density — the hallmark finding
- Posterior corneal defect involving posterior stroma, Descemet membrane, and endothelium
- Iridocorneal adhesions — iris strands extending to the posterior corneal defect
- Lenticulocorneal adhesions — in Type II
- Glaucoma in ~50% of cases due to associated angle anomaly; onset typically in infancy but can occur in childhood or later; prognosis worse than primary congenital glaucoma
- Anterior chamber shallow when lens is displaced anteriorly
Imaging
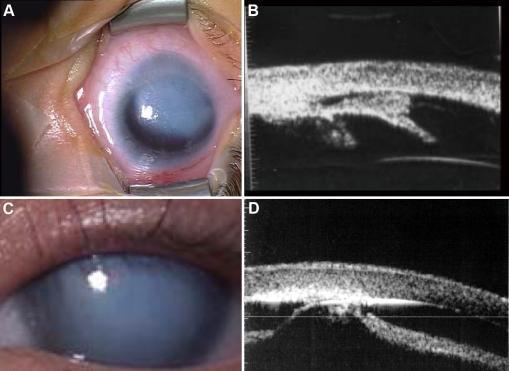
Clinical photographs and ultrasound biomicroscopy (UBM): (A) eccentric localized corneal opacity with (B) iridocorneal adhesion on UBM — Type I; (C) more central diffuse leukoma with (D) keratolenticular adhesion on UBM — Type II
Genetics
- Most cases are sporadic
- Autosomal recessive inheritance has been described
- Mutations in PAX6, PITX2, FOXC1, and CYP1B1 have been implicated in some cases
- Associated with the broader spectrum of anterior segment dysgenesis
Systemic Associations
- Craniofacial anomalies
- CNS anomalies
- Peters plus syndrome: Peters anomaly + skeletal dysplasia with short stature (more common in bilateral cases) + other systemic malformations (e.g., cleft lip/palate, developmental delay)
Differential Diagnosis of Corneal Opacification in Infancy
Peters anomaly must be distinguished from:
- Birth trauma (forceps injury)
- Infectious keratitis
- Metabolic disorders (mucopolysaccharidoses — bilateral)
- Sclerocornea
- Congenital glaucoma (corneal edema)
- Congenital hereditary endothelial/stromal dystrophy
- Corneal dermoid
Workup
- Full ophthalmic examination including gonioscopy and IOP (examination under anaesthesia may be required)
- Ultrasound biomicroscopy (UBM) — key for identifying type of posterior adhesion when the cornea is opaque; differentiates iridocorneal from keratolenticular adhesions
- AS-OCT (anterior segment OCT) — useful in post-operative monitoring
- Fundus photography and A-scan biometry for serial measurements
- Complete systemic examination by a paediatrician
- Chromosomal/genetic analysis where indicated
- Family history
Management
Visual Rehabilitation
- Correct refractive errors and treat amblyopia aggressively — even in unilateral structural anomalies, amblyopia therapy can improve visual acuity
- Penetrating keratoplasty (corneal transplant) for dense corneal opacity obscuring the visual axis — the goal is to restore visual input during the critical period for visual development
- Cataract extraction if a significant cataract is present
Glaucoma
- Medical: beta-blockers, prostaglandin analogues, carbonic anhydrase inhibitors (pilocarpine is not effective as primary therapy)
- Surgical: early surgery (goniotomy, trabeculotomy) often required given severity; prognosis is guarded
Genetics & Systemic
- Genetic counselling and testing
- Screen for Peters plus syndrome in bilateral cases
- Systemic anomalies managed by relevant paediatric specialists
Prognosis
Visual prognosis depends on:
- Laterality (bilateral cases worse)
- Type (Type II with lenticulocorneal adhesion has worse prognosis)
- Severity of glaucoma
- Success of visual rehabilitation and amblyopia treatment
- Graft survival after keratoplasty (at risk for peripheral anterior synechiae and secondary glaucoma)
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed.; The Wills Eye Manual, Office and Emergency Room Diagnosis and Treatment of Eye Disease
This is a shared conversation. Sign in to Orris to start your own chat.