STEMI
Reading File
Finding Sources
Searching PubMed
"ST-elevation myocardial infarction"[MeSH Terms] AND "reperfusion"[MeSH Terms]
Searching Images
STEMI ECG ST elevation myocardial infarction
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Excellent — I have comprehensive content. Now let me compile the full STEMI overview:
ST-Elevation Myocardial Infarction (STEMI)
Definition & Pathophysiology
STEMI results from abrupt, complete thrombotic occlusion of an epicardial coronary artery, most commonly triggered by atherosclerotic plaque rupture with subsequent platelet aggregation and fibrin deposition. Unlike NSTEMI (which involves partial occlusion), STEMI produces transmural ischemia of the territory distal to the occlusion, causing full-thickness myocardial necrosis if not rapidly reperfused.
- Incidence: ~50–133/100,000/year (declining in the US/Europe with improved prevention)
- Average age at first MI: 65.6 years (males), 72.0 years (females)
- More common in men; female incidence rises post-menopause
- Estimated ~500,000 STEMI events annually in the United States
The final infarct size is the primary determinant of prognosis and is determined by two processes: the ischemic injury itself, and reperfusion injury (paradoxical damage upon restoration of flow). Depending on territory size, LV systolic function may be severely impaired, leading to post-infarction heart failure.
ECG Diagnosis
ECG must be obtained within 10 minutes of ED arrival. If initial ECG is non-diagnostic but symptoms persist, repeat every 5–10 minutes.
Diagnostic Criteria (ST Elevation)
- ≥2 contiguous leads with ST elevation ≥1 mm (≥2 mm in V1–V3 in men; ≥1.5 mm in women)
- New LBBB with ischemic symptoms (treated as STEMI equivalent)
ECG Localization of Culprit Artery
| Territory | Leads with ST Elevation | Culprit Artery |
|---|---|---|
| Anterior | V1–V4 | LAD (proximal) |
| Anterolateral | V1–V6, I, aVL | Proximal LAD or left main |
| Lateral | I, aVL, V5–V6 | LCx or diagonal |
| Inferior | II, III, aVF | RCA (80%) or LCx |
| Posterior | ST depression V1–V3 + ST elevation V7–V9 | RCA or LCx |
| Right ventricular | ST elevation V1, V3R–V4R | Proximal RCA |
Key ECG features: convex ("tombstone") ST elevation, hyperacute T-waves (earliest sign), reciprocal ST depression in opposing leads, eventual Q-wave development indicating transmural necrosis.
ECG examples showing classic STEMI patterns:

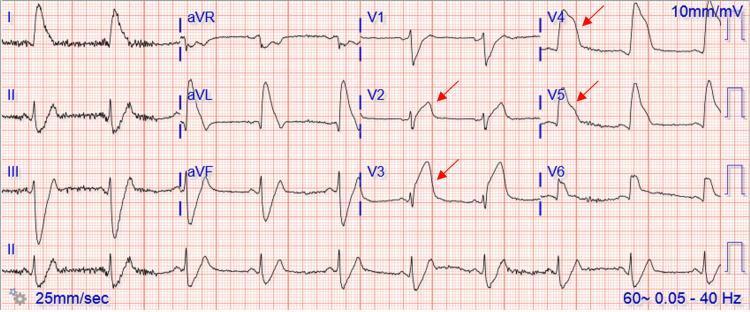
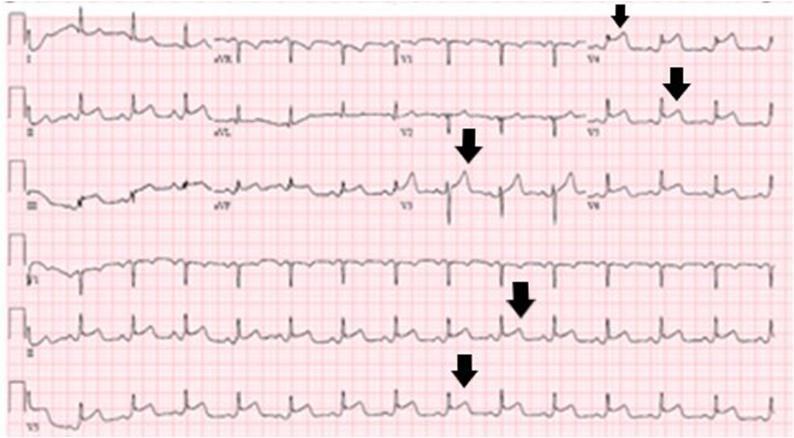
Tip: ST depression in anterior leads V1–V3 with early precordial transition may indicate posterior wall MI, especially if associated with inferior ST elevation (inferoposterior MI). Right-sided leads (V3R–V4R) are essential when inferior STEMI is suspected — to detect right ventricular involvement.
Management Overview
Time-Sensitive Goals
| Strategy | Time Target |
|---|---|
| ECG from door | ≤10 minutes |
| First medical contact to device (PCI center) | ≤90 minutes |
| First medical contact to device (transfer required) | ≤120 minutes |
| Door-in, door-out (non-PCI hospital transfer) | ≤30 minutes |
| Fibrinolysis from diagnosis (if PCI not achievable in time) | ≤10 minutes |
Reperfusion Strategy
Primary PCI (pPCI) is preferred over fibrinolysis when it can be performed by an experienced team within the time window. A large meta-analysis of 23 RCTs confirmed pPCI reduces death, reinfarction, and stroke compared to thrombolysis (Fuster and Hurst's The Heart, 15th ed.).
Fibrinolysis is indicated when:
- PCI cannot be achieved within 120 minutes of first medical contact
- No contraindications exist
- Symptom onset <12 hours
After successful fibrinolysis, patients should be transferred to a PCI-capable center; early elective PCI at 3–24 hours post-lysis is currently recommended. Patients who fail fibrinolysis should receive rescue PCI.
Patients with cardiogenic shock: pPCI is strongly preferred regardless of time delay. Fibrinolysis is not recommended in cardiogenic shock except when PCI/CABG is impossible.
Fibrinolytic Agents
- Clot-specific (preferred in US): Alteplase (tPA), reteplase (rPA), tenecteplase (TNK-tPA)
- Non-clot-specific: Streptokinase, urokinase — act via systemic fibrinogenolysis
Absolute Contraindications to Fibrinolysis
- Prior intracranial hemorrhage (any time) or stroke of unknown origin
- Ischemic stroke within 6 months (or 3 months per some guidelines)
- Known intracranial neoplasm or vascular lesion
- Active or suspected aortic dissection
- Active bleeding or known bleeding disorder (excluding menses)
- Significant head/facial trauma within 3 months
Relative Contraindications
- Uncontrolled severe hypertension (>180/110 mmHg)
- Prolonged CPR (>10 min), recent surgery (<3 weeks), noncompressible puncture
- Pregnancy; active peptic ulcer; high INR on anticoagulation
- Prior streptokinase use (if re-using SK — allergic reaction risk)
Pharmacological Therapy (Acute Phase)
Antiplatelets
| Drug | Dose |
|---|---|
| Aspirin | 162–325 mg (chew if not previously on ASA) |
| Clopidogrel | 600 mg loading dose, then 75 mg/day (no load if >75 yo + fibrinolysis) |
| Prasugrel | 60 mg load at time of PCI (after coronary anatomy defined); 10 mg/day |
| Ticagrelor | 180 mg load, then 90 mg twice daily |
Prasugrel and ticagrelor are preferred P2Y12 inhibitors over clopidogrel for PCI-treated STEMI (more rapid and potent platelet inhibition).
Anticoagulants (Antithrombins)
| Drug | Regimen |
|---|---|
| Unfractionated heparin (UFH) | 60 units/kg IV bolus (max 4,000 U), then 12 units/kg/h (max 1,000 U/h), titrate to aPTT |
| Enoxaparin (LMWH) | 1 mg/kg SC q12h (adjust for renal function/age) |
| Bivalirudin | Direct thrombin inhibitor; option especially if HIT risk |
| Fondaparinux | Option in some settings (not with primary PCI as sole anticoagulant) |
Glycoprotein IIb/IIIa Inhibitors
- Abciximab, eptifibatide, tirofiban — adjunct to PCI, especially in high-thrombus burden
- No dose adjustment needed for CKD with abciximab
β-Blockers
- Oral β-blockers within 24 hours of STEMI (if no contraindications: HR <60, SBP <100, signs of HF, >1st-degree AVB, active bronchospasm)
- IV β-blockers reserved for severe hypertension or ongoing ischemia
- Contraindications: PR >0.24 sec, 2nd/3rd-degree heart block, active asthma, cardiogenic shock risk factors
ACE Inhibitors / ARBs
- Start as soon as possible post-STEMI, especially:
- LVEF <40%
- Anterior MI
- Clinical heart failure
- ARB if ACE inhibitor-intolerant
Aldosterone Antagonist (e.g., Eplerenone)
- Indicated when: already on ACE inhibitor + β-blocker AND LVEF <40% AND HF symptoms or diabetes
Statins
- High-intensity statin (atorvastatin 40–80 mg or rosuvastatin 20–40 mg) initiated acutely
Multivessel Disease in STEMI
- Culprit-only PCI at time of primary PCI is standard
- Complete revascularization of non-culprit vessels: recommended during the index hospitalization or staged early (within days to weeks) for hemodynamically stable patients — trials (COMPLETE, PRAMI, CvLPRIT) demonstrate reduction in major adverse CV events
- Exception: Cardiogenic shock — routine multivessel PCI at index procedure is NOT recommended (CULPRIT-SHOCK trial showed harm)
Dual Antiplatelet Therapy (DAPT) Duration
| Phase | Recommendation |
|---|---|
| Acute/subacute (to 1 year) | DAPT with aspirin + potent P2Y12 (ticagrelor or prasugrel preferred) |
| Shortening | May consider 3–6 months in high bleeding risk |
| De-escalation | Switch from prasugrel/ticagrelor to clopidogrel if bleeding risk high |
| Beyond 1 year | Dual pathway inhibition (ASA + low-dose rivaroxaban 2.5 mg BID — COMPASS trial) in selected patients |
Ticagrelor vs. prasugrel: Head-to-head data (ISAR-REACT 5) showed prasugrel superior in STEMI patients undergoing PCI.
Complications of STEMI
Electrical
- Ventricular fibrillation/tachycardia (highest risk first 24–48 hours)
- Accelerated idioventricular rhythm (reperfusion arrhythmia — usually benign)
- Heart block (especially with inferior MI — RCA supplies AV node in 90%)
- Atrial fibrillation
Mechanical
- Papillary muscle rupture → acute mitral regurgitation (harsh systolic murmur, flash pulmonary edema, 2–7 days post-MI)
- Free wall rupture → cardiac tamponade (rapid hemodynamic collapse, usually fatal without surgery)
- Ventricular septal defect (VSD) → new harsh pansystolic murmur + right heart failure (2–5 days post-MI)
- LV aneurysm → persistent ST elevation, thrombus, refractory HF, arrhythmia (weeks to months)
- LV pseudoaneurysm → contained free wall rupture — urgent surgical repair needed
Pericarditis (Dressler Syndrome)
- Early (1–3 days): pericarditis from transmural necrosis
- Late (Dressler, weeks–months): autoimmune pericarditis
- Treatment: high-dose aspirin preferred; colchicine or narcotic analgesics if not tolerated. Avoid NSAIDs and glucocorticoids (impair myocardial healing)
Cardiogenic Shock
- Occurs in ~5–10% of STEMI
- Defined by hypotension + signs of organ hypoperfusion
- Mortality remains ~40–50% despite modern therapy
- Immediate pPCI is lifesaving; IABP does not reduce mortality (IABP-SHOCK II); consider Impella or ECMO in refractory cases
Post-STEMI Secondary Prevention
| Intervention | Target |
|---|---|
| High-intensity statin | LDL <70 mg/dL (or <55 mg/dL in very high risk) |
| ACE inhibitor or ARB | All patients with LVEF <40%; consider all |
| β-blocker | All patients with LVEF <40%; continue ≥1–3 years |
| Aldosterone antagonist | LVEF <40% + HF or diabetes |
| DAPT | 12 months minimum post-PCI |
| Cardiac rehabilitation | All patients |
| Smoking cessation, BP/DM control | Lifestyle and risk factor modification |
Infarct Size & Prognosis
Infarct size is the strongest independent predictor of post-STEMI mortality and HF. Measured by cardiac MRI (late gadolinium enhancement) or peak troponin/CK-MB. Factors that limit infarct size:
- Rapid reperfusion (every 30-minute delay increases mortality)
- Ischemic preconditioning
- Cardioprotective adjuncts (under investigation: cyclosporine, hypothermia — results mixed)
Recent evidence note: A 2025 systematic review/meta-analysis (PMID 40854299) examined the impact of smartphone apps on reperfusion times in STEMI, suggesting digital health tools may help reduce door-to-balloon times — an emerging area of evidence.
Sources: Fuster and Hurst's The Heart, 15th Ed. · Braunwald's Heart Disease, 10th Ed. · Tintinalli's Emergency Medicine · Textbook of Family Medicine, 9th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.