Pathology of lupus nephritis
Reading File
Finding Sources
Finding Sources
Searching Images
lupus nephritis histology pathology
Searching PubMed
"lupus nephritis"[MeSH Terms] AND classification AND pathology
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive material to write a detailed, well-illustrated answer. Let me compile the full pathology of lupus nephritis.
Pathology of Lupus Nephritis
Lupus nephritis (LN) is the renal manifestation of systemic lupus erythematosus (SLE), which is the prototype of a human systemic immune complex (type III hypersensitivity) disease. Immune complexes composed of nuclear antigens and specific autoantibodies deposit in glomeruli, triggering complement activation and inflammatory cascade. Renal disease produces the greatest risk of morbidity and mortality in lupus patients. It is most common in Black females between 15–45 years of age, and in Asian populations where it accounts for >50% of secondary glomerular diseases in countries such as China, Korea, and Japan.
Pathogenesis
The central mechanism involves loss of tolerance to nuclear antigens. Key autoantibodies include:
- Anti-dsDNA (most specific)
- Anti-histone, anti-RNP, anti-Sm, anti-C1q, anti-endothelial antibodies
These form circulating immune complexes that deposit in glomeruli, or bind planted antigens in situ. Complement activation via the classical pathway (C1q → C3 → C5b–9 membrane attack complex) drives glomerular injury.
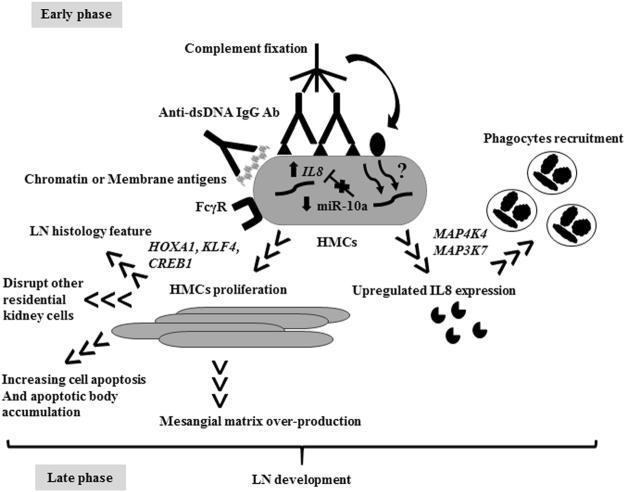
Additional mechanisms include:
- B- and T-lymphocyte abnormalities with loss of peripheral tolerance
- Neutrophil extracellular traps (NETs) — provide a source of nuclear autoantigens
- Defective apoptotic debris clearance → persistent antigenic stimulation
- Macrophage and dendritic cell activation
- Cytokine milieu (IL-6, IL-17, IFN-α, TNF-α)
- Over 50 genetic polymorphisms linked to susceptibility, including CCR6 variants
ISN/RPS Classification (2003, revised 2018)
The International Society of Nephrology / Renal Pathology Society (ISN/RPS) classification divides LN into six classes based primarily on light microscopy (LM), immunofluorescence (IF), and electron microscopy (EM):
| Class | Name | Key Histology | Clinical |
|---|---|---|---|
| I | Minimal mesangial | Normal LM; mesangial deposits on IF/EM only | Asymptomatic; normal urinalysis |
| II | Mesangial proliferative | Mesangial hypercellularity + matrix expansion; mesangial deposits | Mild proteinuria/hematuria; no nephrotic syndrome |
| III | Focal nephritis | Endocapillary ± extracapillary proliferation in <50% glomeruli | Variable; hematuria, proteinuria, possible renal insufficiency |
| IV | Diffuse nephritis | Endo ± extracapillary proliferation in ≥50% glomeruli; wire-loop lesions | Most severe; nephrotic + nephritic, hypertension, renal failure |
| V | Membranous nephritis | Diffuse subepithelial deposits; GBM thickening + spikes | Nephrotic syndrome; may coexist with III or IV |
| VI | Advanced sclerosing | >90% global glomerulosclerosis | ESKD; irreversible |
Class III and IV lesions are qualitatively identical and differ only in the percentage of glomeruli involved (the threshold is 50%).
Class-by-Class Histopathology
Class I — Minimal Mesangial LN
- LM: Normal-appearing glomeruli (normocellular, patent capillary lumens)
- IF: Mesangial IgG (and often other immunoglobulins) deposits
- EM: Small electron-dense deposits within mesangium
- Rarely biopsied; patients are usually asymptomatic
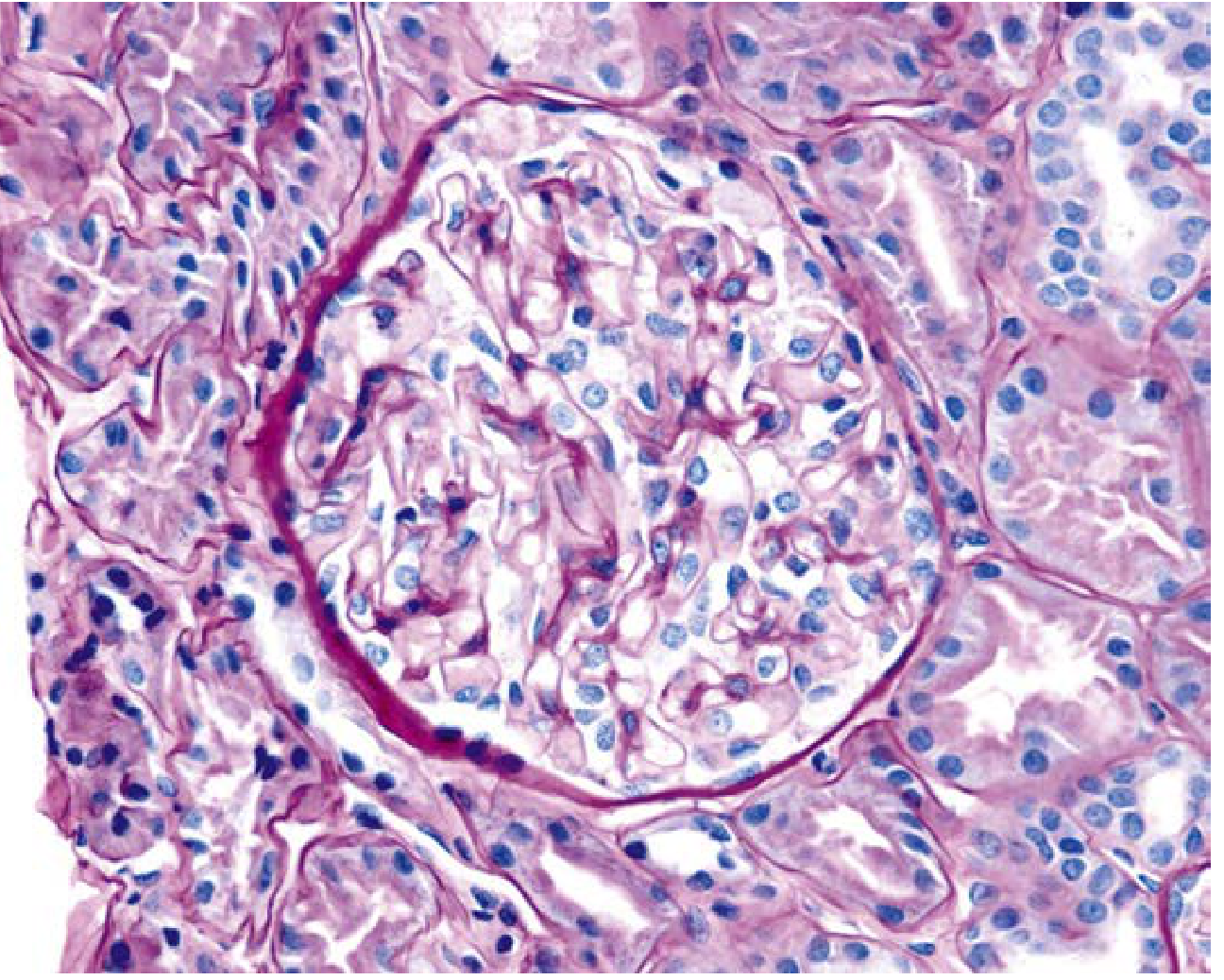
Class II — Mesangial Proliferative LN
- LM: Mesangial hypercellularity with mesangial matrix expansion
- IF: Mesangial deposits of IgG (± IgM, IgA, C3, C1q)
- EM: Numerous electron-dense deposits within expanded mesangium
- No capillary wall involvement
- Clinical: Mild proteinuria or microscopic hematuria; almost never nephrotic syndrome or renal failure
Class III — Focal LN
- LM: Endocapillary hypercellularity in <50% of glomeruli, often segmental; fibrinoid necrosis, karyorrhectic debris, ± crescents; PMN infiltration
- IF: Focal mesangial and capillary wall deposits
- EM: Mesangial and subendothelial electron-dense deposits
- May include active (A), chronic (C), or mixed (A/C) lesions
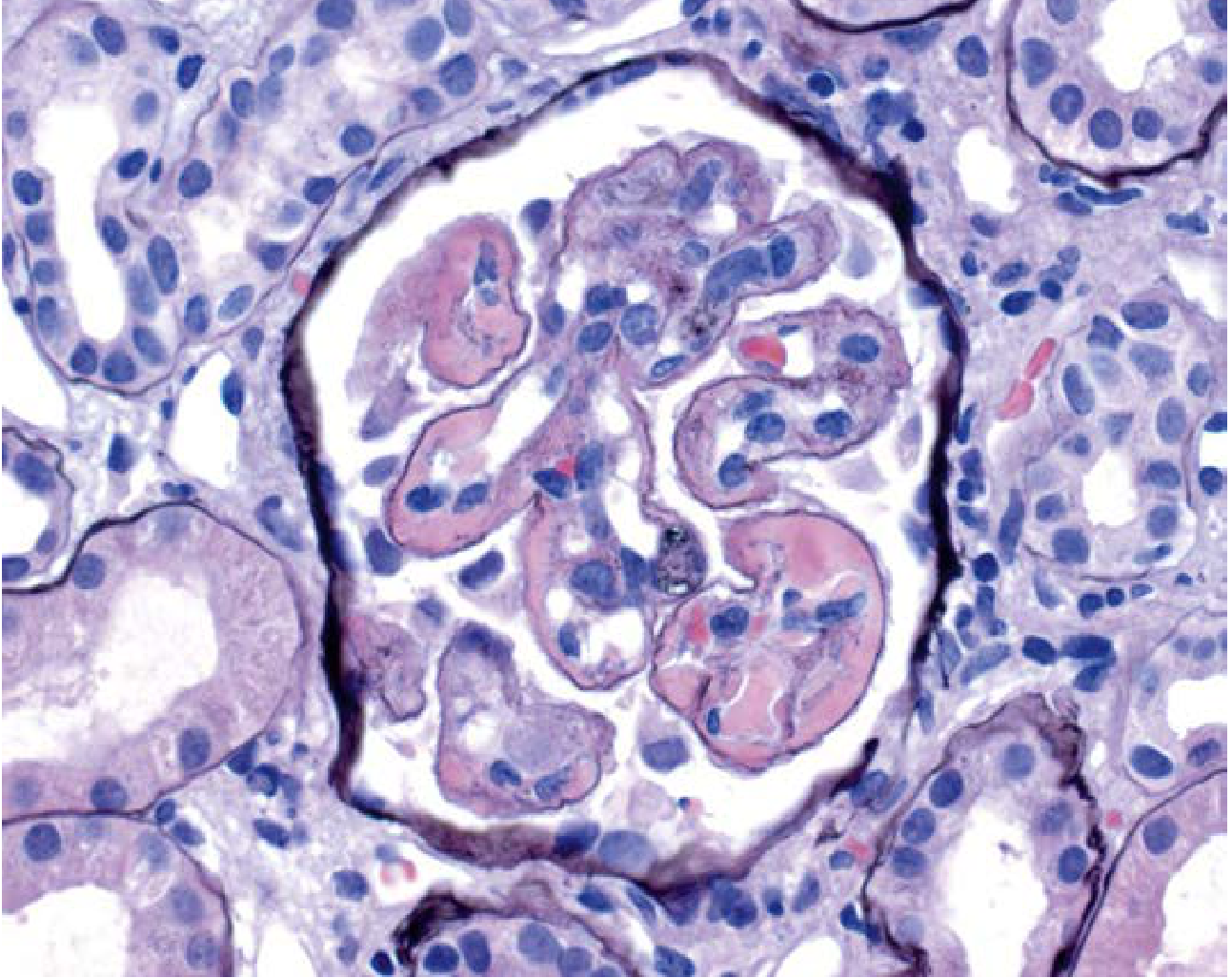
Class IV — Diffuse LN (Most Common & Most Severe)
- LM: Endocapillary (and often extracapillary) hypercellularity in ≥50% of glomeruli
- "Wire-loop" lesions — eosinophilic thickening of peripheral capillary walls due to massive subendothelial immune deposits enclosed by silver-positive GBM
- "Hyaline thrombi" (misnomer) — intraluminal immune complex deposits filling capillary lumens
- Karyorrhectic nuclear debris, monocyte infiltration, crescents
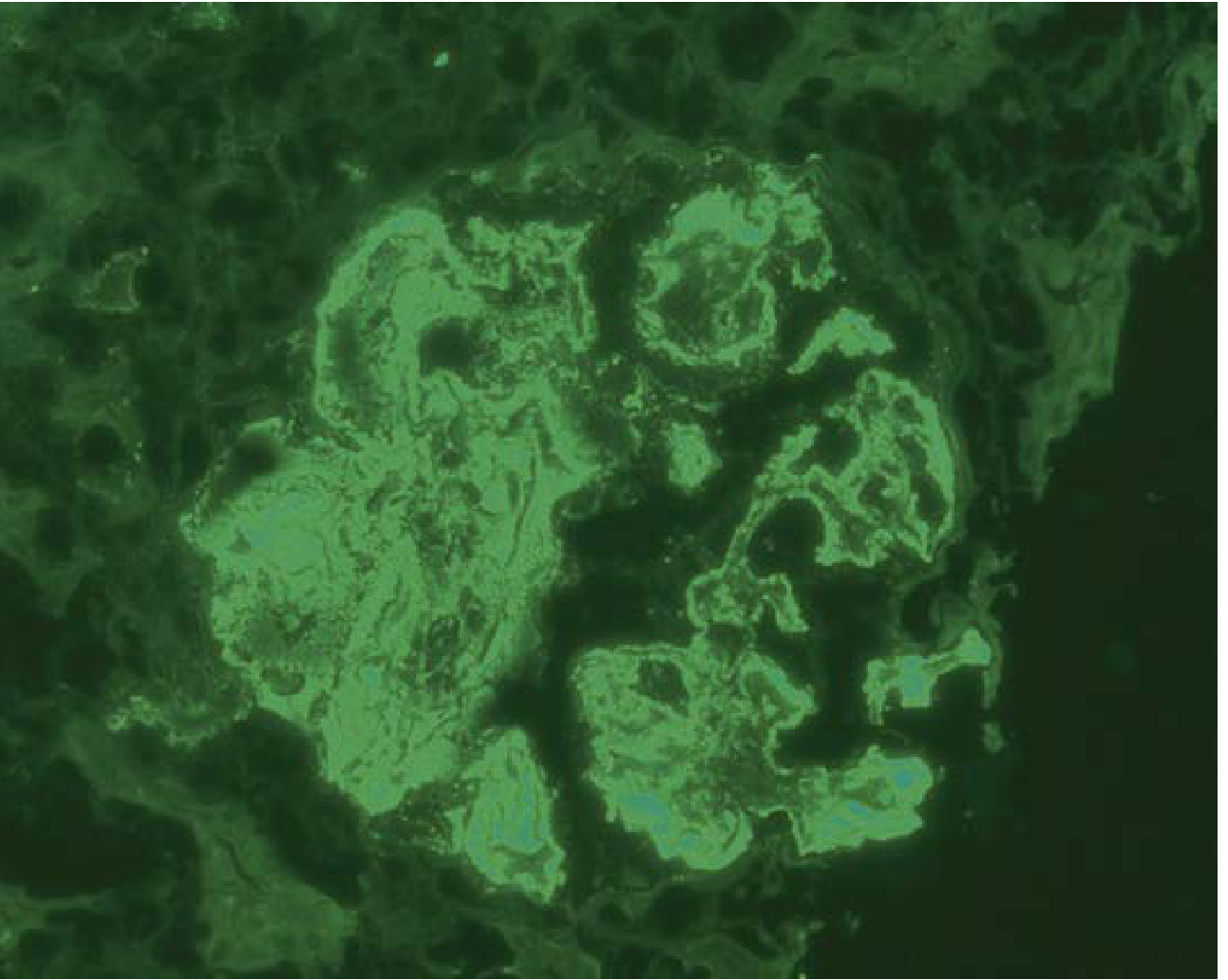
- IF: Diffuse granular deposits of IgG, IgM, IgA, C3, C1q in mesangium and capillary walls — "full house" pattern; intense C1q staining is a helpful diagnostic clue
- EM: Massive mesangial and subendothelial electron-dense deposits; may show tubular/fingerprint substructure; tubuloreticular inclusions (TRIs) in endothelial cytoplasm (induced by IFN-α)
- Clinical: Hematuria + proteinuria + hypertension ± renal failure; red cell casts; nephrotic syndrome
Class IV is further subclassified:
- IV-S: diffuse segmental (>50% glomeruli, each with segmental lesions)
- IV-G: diffuse global (>50% glomeruli, each with global lesions)
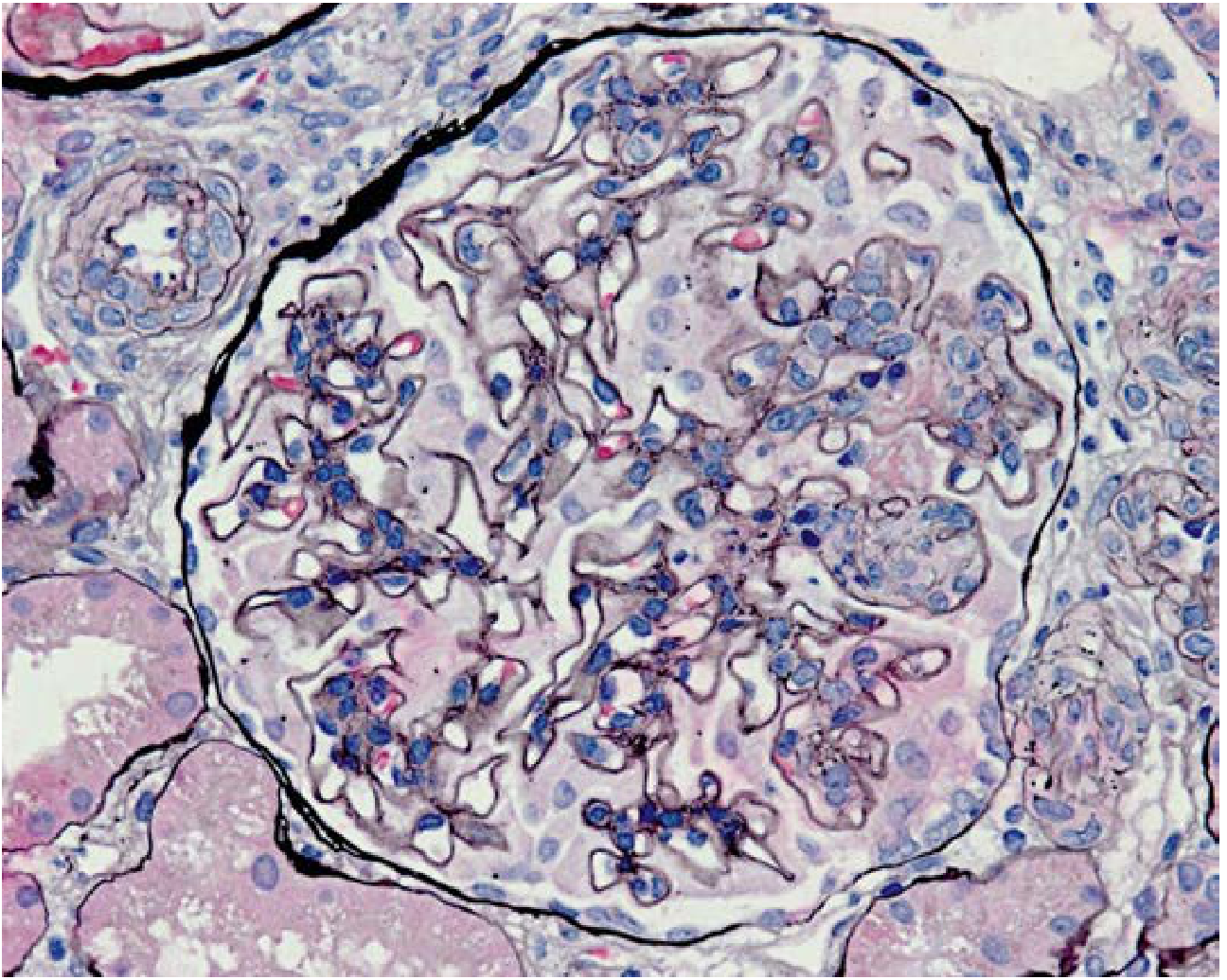
Class V — Membranous LN
- LM: Diffuse thickening of glomerular capillary walls (spherical/rigid-loop appearance); mild mesangial hypercellularity
- Silver stain: "Spikes" of GBM projecting between subepithelial deposits
- IF: Diffuse granular IgG (± others) along capillary walls (subepithelial pattern)
- EM: Prominent subepithelial electron-dense deposits; podocyte foot process effacement
- May coexist with class III or IV ("mixed" membranous + proliferative)
- Clinical: Severe proteinuria and nephrotic syndrome
Class VI — Advanced Sclerosing LN
- LM: >90% global glomerulosclerosis — no residual activity
- Represents end-stage, irreversible kidney disease (ESKD)
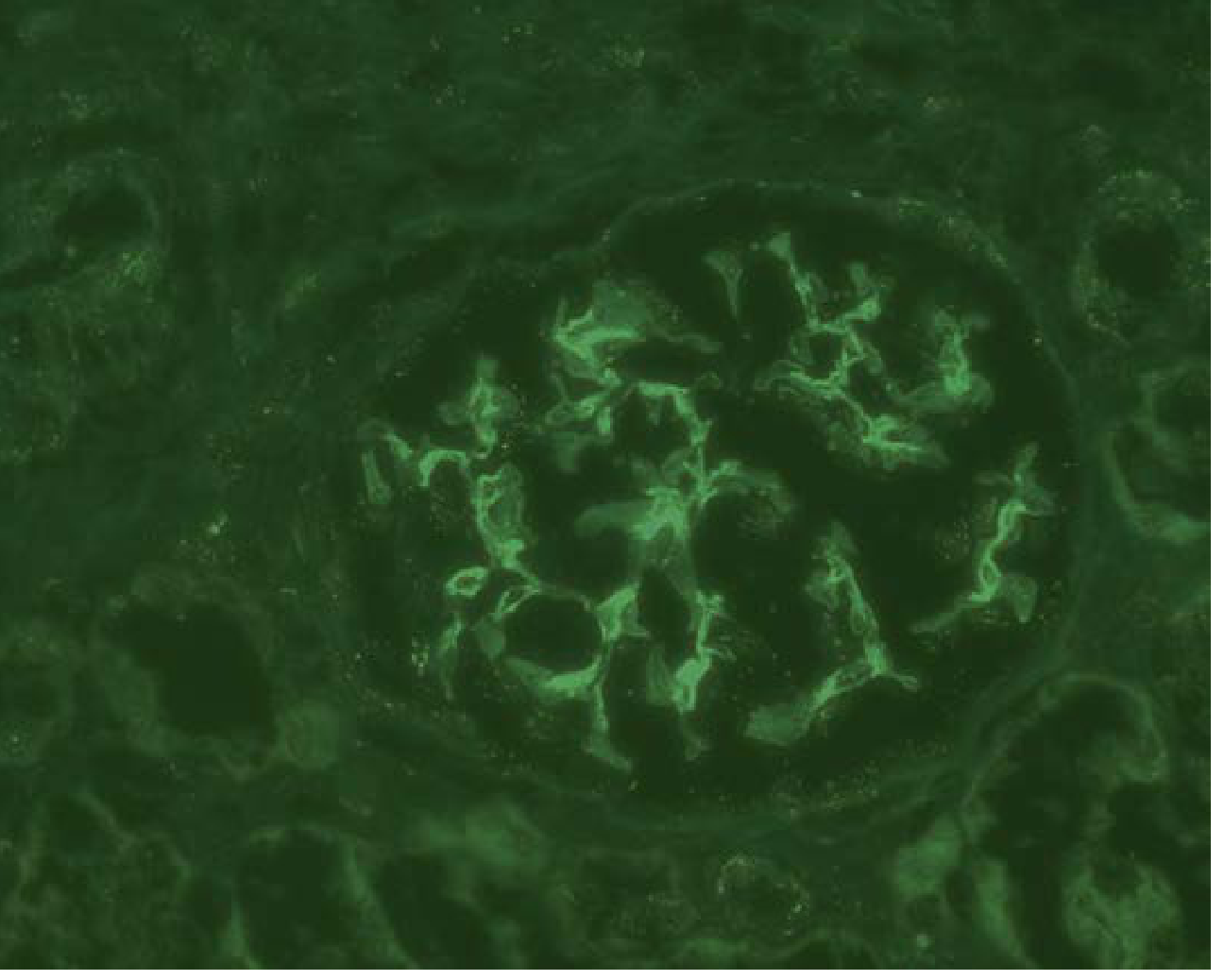
"Full House" Immunofluorescence
A hallmark of lupus nephritis across all classes is the "full house" IF pattern: simultaneous granular staining for IgG, IgM, IgA, C3, and C1q within glomeruli. The intense C1q staining is particularly characteristic. This multi-isotype, multi-complement deposition reflects activation of the classical pathway by DNA–anti-DNA immune complexes.
Tubulointerstitial and Vascular Lesions
LN can involve all renal compartments beyond the glomerulus:
Tubulointerstitial:
- Immune complex deposits in tubular basement membranes (on IF/EM)
- Tubulitis with lymphocytic infiltration
- Tubular atrophy and interstitial fibrosis (chronicity markers)
Vascular lesions — several patterns are recognised:
- Lupus vasculopathy — non-inflammatory immune complex deposits in vessel walls
- Thrombotic microangiopathy (TMA) — fibrin thrombi, endothelial swelling, possibly related to antiphospholipid antibodies
- True vasculitis — rare necrotising arteritis
- Arteriosclerosis — chronic hypertensive changes
NIH Activity and Chronicity Indices
Separate scoring of individual lesions guides prognosis and treatment response:
Activity Index (AI) — total score 0–24 (scored 0–3+ each):
| Lesion | Weight |
|---|---|
| Endocapillary hypercellularity | ×1 |
| Neutrophil infiltration | ×1 |
| Subendothelial hyaline deposits (wire loops) | ×1 |
| Fibrinoid necrosis/karyorrhexis | ×2 |
| Cellular crescents | ×2 |
| Interstitial inflammation | ×1 |
Chronicity Index (CI) — total score 0–12 (scored 0–3+ each):
| Lesion |
|---|
| Glomerular sclerosis |
| Fibrous crescents |
| Tubular atrophy |
| Interstitial fibrosis |
High chronicity index predicts poor renal prognosis. These indices are used to assess response to therapy on repeat biopsies.
Lupus Podocytopathy
A separate entity not included in ISN/RPS classification. Presents with nephrotic syndrome in SLE patients but shows:
- Normal glomeruli, FSGS, or mesangial proliferation on LM
- No endocapillary hypercellularity or crescents
- IF: No deposits or only mesangial deposits
- EM: Severe diffuse podocyte foot process effacement without electron-dense deposits
- Represents primary podocyte injury rather than immune complex deposition; high relapse rate
Progression and Clinical Correlations
| Feature | Prognostic Implication |
|---|---|
| Class IV with crescents | Aggressive; requires prompt induction therapy |
| High AI | Active disease amenable to treatment |
| High CI | Irreversible damage; poor renal prognosis |
| Mixed class IV + V | More proteinuria; harder to treat |
| Crescentic LN | Associated with anti-neutrophil cytoplasm antibodies (ANCA) in Chinese patients |
| Vascular/endothelial lesions | Signify aggressive disease |
| Baseline creatinine >0.9 mg/dL + proteinuria >0.5 g/24h | Adverse prognostic markers |
Recent Evidence (2024–2026)
A 2026 systematic review (PMID 41169181) in Arthritis & Rheumatology reviews serum and urinary biomarkers (including anti-dsDNA, complement, urinary CXCL10, TWEAK) that correlate with histopathologic class and activity indices, potentially enabling non-invasive disease monitoring. A 2025 meta-analysis (PMID 41142814) highlights IL-18 as an amplifier of immune-mediated nephropathy in LN. These studies do not alter the ISN/RPS classification or standard biopsy interpretation but underscore the need for biomarkers that reflect histologic activity without repeat biopsy.
Sources: Robbins & Kumar Basic Pathology (9780323790185); Henry's Clinical Diagnosis and Management by Laboratory Methods (9780323673204); Brenner and Rector's The Kidney (9780323532655); Comprehensive Clinical Nephrology 7e (9780323825924); National Kidney Foundation Primer on Kidney Diseases 8e (9780323791229)
This is a shared conversation. Sign in to Orris to start your own chat.