Tubercolosis I want a full fledge account on it that i can also write in university exams of mbbs first year in AIT questions of subjects anatomy,physiology and biochemistry
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Reading File
TUBERCULOSIS - A Complete MBBS First Year Account
For AIT (Answer-in-Time) Questions in Anatomy, Physiology & Biochemistry
OVERVIEW / INTRODUCTION
Tuberculosis (TB) is a chronic granulomatous infectious disease caused primarily by Mycobacterium tuberculosis (MTB). It most commonly affects the lungs but can involve virtually any organ. It is the world's leading cause of death from a single infectious agent and remains a major global health burden, with the highest incidence rates in South-East Asia and Sub-Saharan Africa.
PART I - BIOCHEMISTRY PERSPECTIVE
1. The Organism - Mycobacterium tuberculosis
M. tuberculosis is a non-motile, non-spore-forming, obligate aerobe, slightly curved rod. It is classified as weakly Gram-positive but is best identified by acid-fast staining.
Key biochemical properties (from Medical Microbiology 9e):
| Property | Detail |
|---|---|
| Guanine + Cytosine content | 61-71 mol% (very high G+C content in DNA) |
| Generation time | ~15-20 hours (extremely slow-growing) |
| Growth in culture | 3-8 weeks on Lowenstein-Jensen (LJ) medium |
| Colony morphology | Non-pigmented or light tan, rough "buff-coloured" colonies |
| Catalase | Positive at 22°C but negative at 68°C (heat-labile catalase) |
2. The Biochemistry of the Cell Wall (Most Important Biochemistry Topic)
The cell wall of M. tuberculosis is unique and is the molecular basis for most of its properties - acid-fastness, slow growth, drug resistance, and pathogenicity.
Structure (from innermost to outermost):
- Cytoplasmic membrane - standard phospholipid bilayer
- Peptidoglycan layer - linked to arabinogalactan by a phosphodiester bond
- Arabinogalactan - a complex polysaccharide covalently linked to peptidoglycan
- Mycolic acids (most important!) - very long-chain (C70-C90) branched fatty acids, esterified to arabinogalactan. These are unique to mycobacteria and related genera.
- Free lipids in the outer layer:
- Cord factor (trehalose dimycolate) - causes serpentine "cord-like" growth in culture, inhibits neutrophil migration, toxic to mitochondria
- Phthiocerol dimycocerosate (PDIM) - contributes to phagosomal escape and virulence
- Sulfolipids - inhibit phagolysosome fusion
- Lipoarabinomannan (LAM) - major surface glycolipid, immunomodulatory, inhibits macrophage activation by IFN-γ
Why acid-fastness?
The mycolic acids form a hydrophobic barrier that resists decolorization by acid-alcohol after Ziehl-Neelsen (ZN) staining. The dye carbol fuchsin penetrates via heat and cannot be washed out by 20% H2SO4 or 3% HCl-alcohol. Hence M. tuberculosis stains red on blue background (AFB positive).
Biochemical consequences of the cell wall:
- Resistance to common antibiotics (beta-lactams, etc.) - the thick waxy layer reduces permeability
- Resistance to desiccation - survives months in dried sputum
- Resistance to host digestive enzymes after phagocytosis
- Slow growth - the thick cell wall slows nutrient transport
3. Purified Protein Derivative (PPD) / Tuberculin
PPD is extracted from culture filtrates of MTB. It contains cell wall proteins that act as antigens, stimulating the patient's cellular (Th1) immune response. This is used in the Mantoux test (tuberculin skin test, TST) - basis of delayed hypersensitivity (Type IV hypersensitivity reaction involving sensitized T lymphocytes).
4. Biochemistry of Drug Action (Important for Exams)
| Drug | Biochemical Target |
|---|---|
| Isoniazid (INH) | Inhibits InhA (enoyl-ACP reductase) - blocks mycolic acid synthesis |
| Rifampicin | Inhibits DNA-dependent RNA polymerase (β-subunit), blocks mRNA synthesis |
| Pyrazinamide | Disrupts membrane transport; active at low pH (inside granuloma) |
| Ethambutol | Inhibits arabinosyl transferase - blocks arabinogalactan synthesis |
| Streptomycin | Binds 30S ribosomal subunit - inhibits protein synthesis |
Isoniazid and Ethambutol both target the unique cell wall, making them highly specific anti-TB agents.
PART II - PHYSIOLOGY PERSPECTIVE
1. Respiratory Physiology and TB
M. tuberculosis is transmitted via aerosolized droplet nuclei (1-5 μm in diameter) produced when a person with active pulmonary TB coughs, sneezes, or speaks. Particles of this size bypass upper airway defenses (mucociliary escalator, nasal turbinate filtration) and reach the respiratory bronchioles and alveoli directly.
- Particles >10 μm are filtered by nasal hairs and mucus
- Particles 5-10 μm are trapped by the mucociliary ladder
- Particles <5 μm (droplet nuclei) - reach alveoli - the infective units of TB
2. The Immune (Physiological) Response to TB
This is the most important physiology topic relating to TB:
Phase A: Before Cell-Mediated Immunity Develops (First ~3 weeks)
- MTB bacilli land in the alveolus and are phagocytosed by alveolar macrophages
- MTB survives inside the phagosome by:
- Blocking phagolysosome fusion (sulfolipids, LAM)
- Preventing acidification of the phagosome
- Escaping reactive oxygen and nitrogen species
- Without adequate immune control → unchecked bacillary proliferation → bacteremia with seeding of multiple sites
Phase B: Initiation of Cell-Mediated Immunity (after ~3 weeks)
This is shown beautifully in the diagram below:
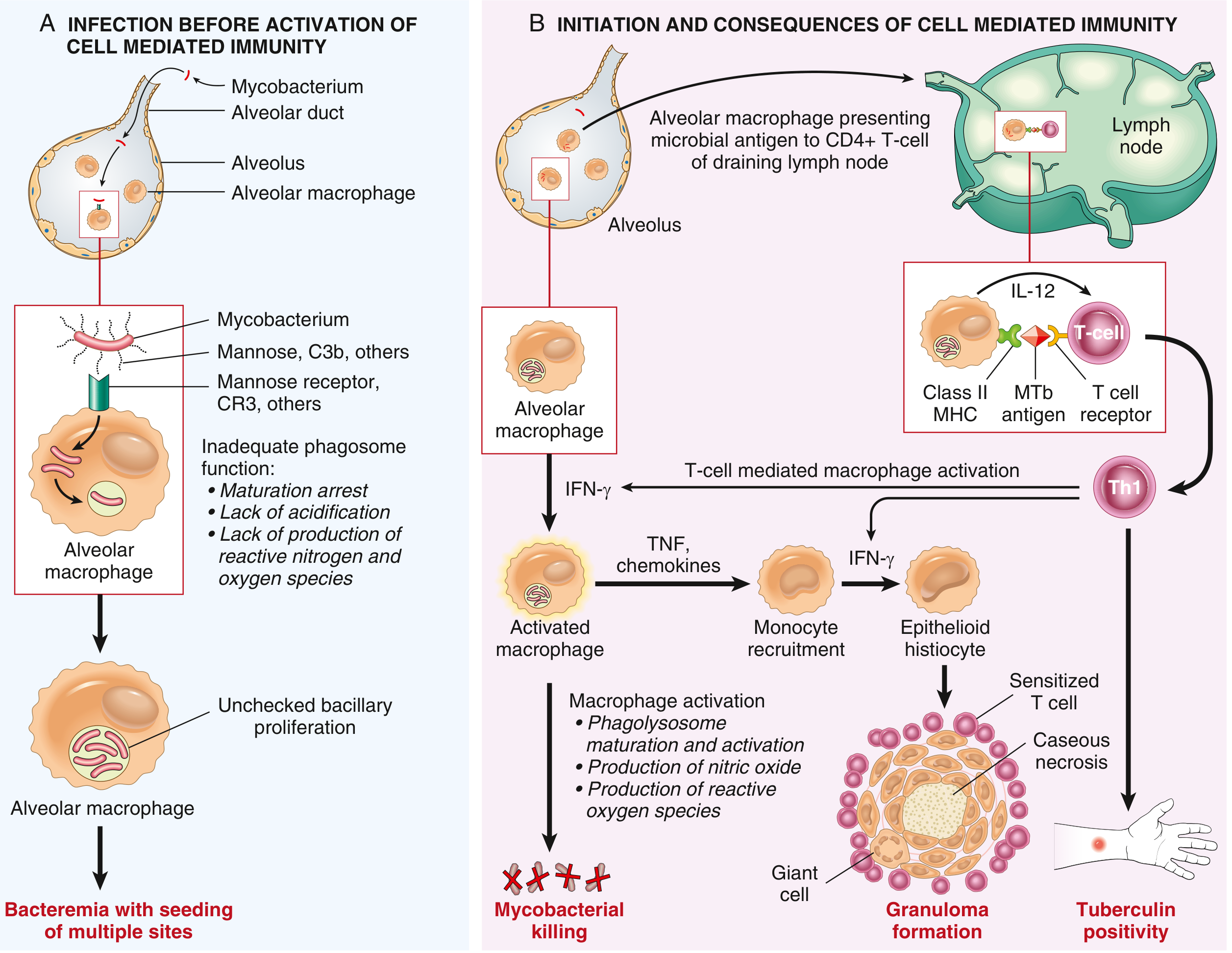
Fig. 11.34 from Robbins & Kumar Basic Pathology - showing the full sequence from macrophage phagocytosis (A) to Th1-mediated immunity and granuloma formation (B)
Step-by-step mechanism:
- Alveolar macrophages present MTB antigens via Class II MHC to CD4+ T cells in draining lymph nodes
- Macrophages secrete IL-12 → drives differentiation of CD4+ T cells into Th1 subset
- Th1 cells release IFN-γ → feeds back to activate macrophages
- Activated macrophages:
- Complete phagolysosome fusion
- Produce reactive nitrogen intermediates via inducible nitric oxide synthase (iNOS) → most important mycobactericidal mechanism
- Produce reactive oxygen species (ROS)
- Release TNF → recruits more monocytes
- Differentiate into epithelioid histiocytes → aggregate to form granulomas
- Sensitized T cells accumulate around the granuloma
- Tuberculin test becomes positive (conversion) - sign that immunity has developed
Summary: Immunity in TB is primarily Th1/Cell-mediated
Defects in: IL-12, IFN-γ, TNF, or nitric oxide production → poorly formed granulomas → disease progression. This explains why TNF-blocker drugs (used for rheumatoid arthritis) can reactivate latent TB.
3. Physiological Basis of Symptoms
| Symptom | Physiological Mechanism |
|---|---|
| Fever | TNF-α and IL-6 act on the hypothalamus as endogenous pyrogens, raising set point |
| Night sweats | Compensatory sweating as fever breaks in early morning hours |
| Weight loss / cachexia | Chronic TNF-α secretion promotes muscle protein catabolism and anorexia |
| Cough | Irritation of airways by caseous necrosis and cavity formation |
| Hemoptysis | Erosion of pulmonary blood vessels by cavitating lesions |
| Dyspnea | Impaired gas exchange from lung consolidation and fibrosis |
4. Hypoxic Drive in TB
In advanced pulmonary TB with extensive consolidation, the hypoxic ventilatory response may be blunted. The V/Q mismatch from areas of consolidation reduces PaO2, eventually stimulating chemoreceptors and increasing respiratory rate.
PART III - ANATOMY PERSPECTIVE
1. Anatomical Sites of TB Involvement
A. Primary TB - The Ghon Complex
Primary TB begins when bacilli first infect a previously unsensitized person. The anatomical lesion is the Ghon Complex (from Robbins Basic Pathology):
| Component | Description |
|---|---|
| Ghon focus | 1-1.5 cm area of gray-white consolidation in the lung parenchyma. Undergoes central caseous necrosis. Location: lower part of upper lobe OR upper part of lower lobe, close to the pleura |
| Regional lymphadenopathy | Tubercle bacilli travel via lymphatics to hilar/mediastinal lymph nodes, which also undergo caseation |
| Ghon complex | Ghon focus + regional caseating lymphadenopathy together |
| Ranke complex | Calcified Ghon complex visible on chest X-ray (after healing) |
Why this location? The lower upper lobe / upper lower lobe has greatest ventilation and blood flow, so inhaled bacilli preferentially implant here.
When the healed Ghon focus calcifies, it is visible as a calcified scar on CXR. Simon foci are calcified secondary foci of infection in the lung apices.
B. Secondary (Reactivation) TB - Apical Localization
Secondary TB is classically located at the apex of the upper lobes (Apex = "Simon foci" region). Reasons for apical preference:
- Higher oxygen tension (obligate aerobe thrives here)
- Relatively poor lymphatic drainage
- Lower blood flow relative to ventilation (high V/Q ratio)
C. Anatomy of the Granuloma (Tubercle)
The basic anatomical/histological unit of TB is the tuberculous granuloma (tubercle):
Structure from center to periphery:
- Central caseous necrosis - cheese-like amorphous material (contains dead macrophages, bacteria, lipid). Unique to TB among common granulomas.
- Epithelioid macrophages - activated macrophages with abundant pale cytoplasm
- Langhans giant cells - multinucleate cells formed by fusion of epithelioid macrophages; nuclei arranged in a horseshoe or peripheral ring pattern (distinguishes from foreign body giant cells where nuclei are central)
- Lymphocytes - surrounding cuff of CD4+ T cells
- Fibroblasts - peripheral rim, producing fibrous capsule
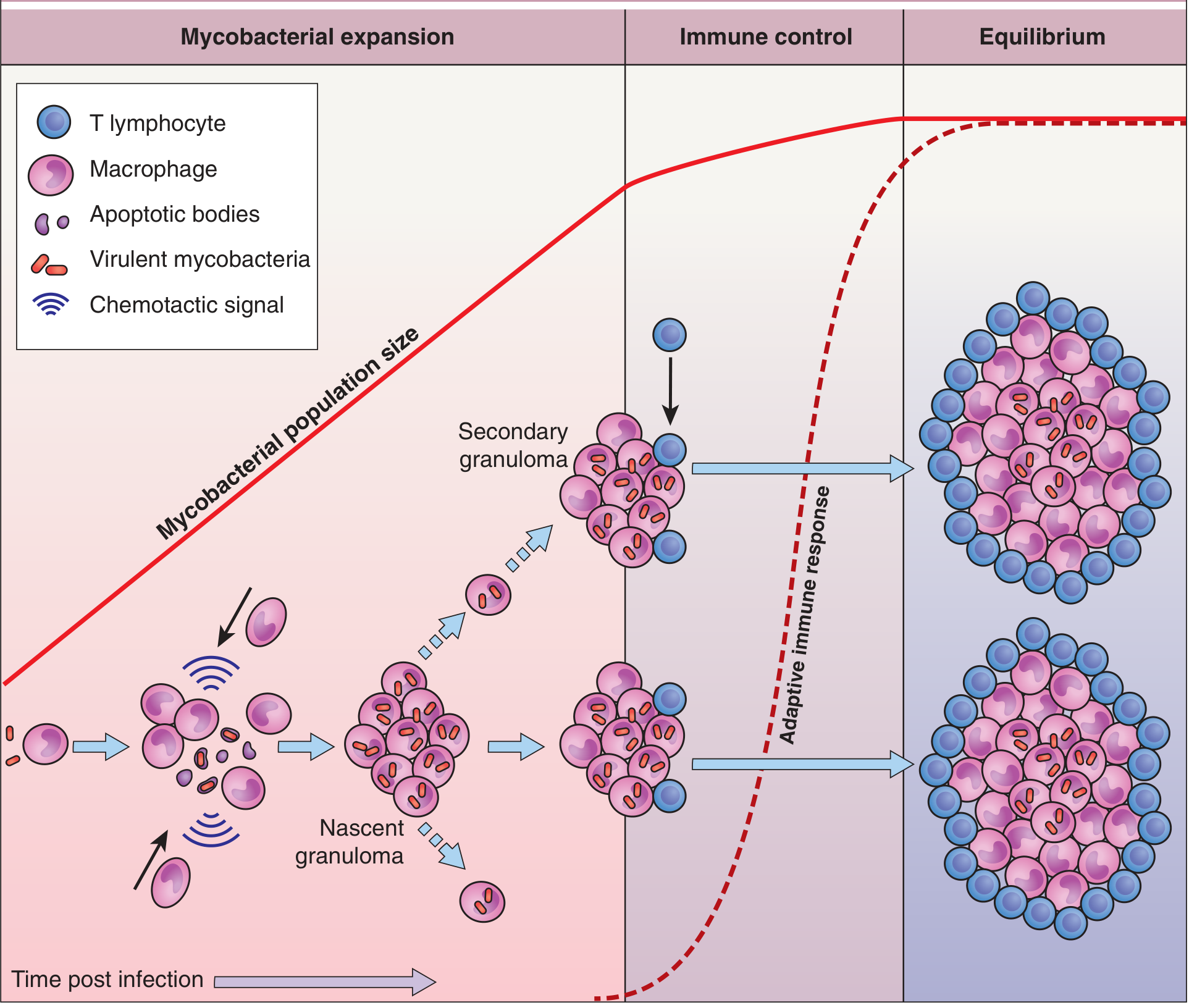
Stages of granuloma formation in tuberculosis (Dermatology 5e) - showing mycobacterial expansion phase, immune control phase, and equilibrium
The diagram above shows:
- Left (mycobacterial expansion): Nascent granuloma - macrophages (pink) engulf virulent mycobacteria (red rods); apoptotic bodies released; chemotactic signals recruit more macrophages
- Middle (immune control): T lymphocytes (blue) are recruited as adaptive immune response begins; secondary granuloma forms
- Right (equilibrium): Mature granuloma - T lymphocytes surround a core of macrophages containing bacteria; bacterial growth is controlled but not eradicated
D. Anatomical Spread of TB
TB can spread anatomically by several routes:
1. Lymphatic spread:
- From Ghon focus to hilar nodes (part of Ghon complex)
- Further to mediastinal, supraclavicular, or abdominal nodes
2. Hematogenous spread:
- Via thoracic duct → superior vena cava → systemic circulation
- Miliary TB: uniform seeding of multiple organs (appears as millet seed-sized nodules on CXR)
- Sites seeded: meninges (TB meningitis), bone marrow, liver, spleen, kidney, adrenal (Addison's disease), fallopian tubes, epididymis
3. Direct extension:
- Pleura → TB pleuritis / pleural effusion
- Pericardium → tuberculous pericarditis
- Chest wall (rare)
4. Bronchogenic spread:
- Liquefied caseous material drains through a bronchus → cavity formation
- Spread to new lung segments/lobes via the bronchial tree
- Most contagious stage
E. Extrapulmonary TB - Anatomical Locations
| Site | Disease | Anatomical Notes |
|---|---|---|
| Meninges | TB meningitis | Basilar meningitis; thick exudate at base of brain; involvement of cranial nerves II, III, IV, VI |
| Cervical lymph nodes | Scrofula | Most common extrapulmonary site; painless rubbery nodes → collar-stud abscess (pus tracks through deep fascia) |
| Vertebral column | Pott's disease | Affects thoracic vertebrae most commonly (T10-L2); disc space loss + vertebral collapse → kyphosis ("Gibbus deformity"); paravertebral abscess ("cold abscess") |
| Hip/Knee joint | TB arthritis | Monoarthritis; bone destruction; "dough-like" joint swelling |
| Kidney | Renal TB | "Putty kidney" (dystrophic calcification); sterile pyuria |
| Epididymis | TB epididymo-orchitis | Beaded vas deferens on palpation |
| Fallopian tube | Genital TB | Commonest cause of infertility in TB-endemic areas |
| Adrenal gland | Addison's disease | Bilateral adrenal destruction; mineralocorticoid + glucocorticoid deficiency |
| Skin | Lupus vulgaris | Soft brownish-red plaque; "apple-jelly" nodules on diascopy |
F. Anatomy of the Lung - Relevant to TB
The right lung has 3 lobes (upper, middle, lower) and 10 bronchopulmonary segments. The left lung has 2 lobes (upper, lower) and 8-9 segments.
TB commonly affects:
- Posterior segment of upper lobe (S2) - most common in both lungs
- Apical segment of upper lobe (S1)
- Superior segment of lower lobe (S6)
The bronchopulmonary segment is the functional anatomical unit relevant to surgical resection of TB lesions. Each segment has its own bronchus, artery, and is separated from adjacent segments by a connective tissue septum.
PART IV - PATHOLOGICAL SUMMARY (Integrating All Three Subjects)
Types of TB Lesions (Morphology)
| Lesion | Features |
|---|---|
| Caseating granuloma | Central caseous necrosis; classic TB; Langhans giant cells; AFB may be present |
| Non-caseating granuloma | May occur in TB; also seen in sarcoidosis (distinguish on clinical grounds) |
| Liquefaction | Caseous material becomes liquid → cavity formation; high bacillary load; most infectious |
| Fibrosis/Calcification | Healing phase; bacilli may be trapped but viable (latent TB reservoir) |
| Miliary TB | 1-2 mm yellow-white nodules scattered throughout organ; hematogenous dissemination |
Fate of Primary TB in 95% of Patients:
- Cell-mediated immunity develops (~3 weeks post-infection)
- Granuloma walls off the infection
- Caseous material desiccates and calcifies
- Ghon complex → Ranke complex (radiologically visible calcified scar)
- Latent TB - bacilli remain viable within granuloma for decades
Reactivation (5% lifetime risk; rises with immunosuppression):
- Triggers: HIV infection (CD4 <200/μL), malnutrition, diabetes, steroids, anti-TNF therapy, silicosis, aging
- Reactivation TB localizes to the lung apex (high O2 tension)
PART V - DIAGNOSIS (Integration)
| Test | Basis |
|---|---|
| Sputum AFB smear (ZN stain) | Mycolic acids make MTB acid-fast; red bacilli on blue background |
| Culture (LJ medium) | Growth in 3-8 weeks; definitive; biochemical basis |
| Mantoux test (TST) | Type IV hypersensitivity; 0.1 mL PPD intradermal; read at 48-72 hours; induration >10 mm = positive |
| IGRA (Interferon-gamma release assay) | Measures IFN-γ released by sensitized T cells when stimulated by TB-specific antigens (ESAT-6, CFP-10); physiological basis |
| Chest X-ray | Upper lobe infiltrates, cavities, fibrosis, calcified Ghon complex; anatomical basis |
| Nucleic Acid Amplification (GeneXpert) | Detects MTB DNA and rifampicin resistance (rpoB gene) |
QUICK REVISION TABLE FOR EXAMS
| Subject | Key Topic | Core Fact |
|---|---|---|
| Biochemistry | Cell wall | Mycolic acids (C70-C90); cause acid-fastness; inhibit phagolysosome fusion |
| Biochemistry | Drug targets | INH → mycolic acid synthesis; Ethambutol → arabinogalactan; Rifampicin → RNA polymerase |
| Biochemistry | Cord factor | Trehalose-6,6'-dimycolate; inhibits PMN migration; serpentine cord growth |
| Physiology | Immunity | Th1 → IFN-γ → macrophage activation → iNOS → reactive nitrogen intermediates → kill MTB |
| Physiology | Symptoms | TNF-α causes fever, night sweats, cachexia (anorexia + muscle wasting) |
| Physiology | Transmission | Droplet nuclei <5 μm → alveoli; bypass mucociliary defense |
| Anatomy | Primary TB | Ghon focus (lower upper/upper lower lobe) + hilar LN = Ghon complex |
| Anatomy | Secondary TB | Apex of upper lobe; cavitation; high O2 tension |
| Anatomy | Granuloma | Center-out: caseous necrosis → epithelioid cells → Langhans giant cells → lymphocytes → fibrosis |
| Anatomy | Pott's disease | T10-L2 vertebrae; cold abscess; Gibbus deformity |
| Anatomy | Miliary TB | Hematogenous spread; 1-2 mm nodules; affects any organ |
SAMPLE EXAM QUESTION ANSWERS
Q: Describe the cell wall of Mycobacterium tuberculosis and its significance. (Biochemistry AIT)
Answer: The cell wall of M. tuberculosis is uniquely complex. From inside out: cytoplasmic membrane → peptidoglycan → arabinogalactan → mycolic acids (C70-C90 branched fatty acids). Outer free lipids include cord factor (trehalose dimycolate), sulfolipids, and lipoarabinomannan (LAM). The mycolic acid layer confers acid-fastness (resistance to decolorization with acid-alcohol in ZN stain). It also: (1) resists common antibiotics by reducing permeability, (2) inhibits phagolysosome fusion allowing intracellular survival, (3) slows nutrient transport causing slow growth, (4) provides antigens (PPD) for tuberculin testing. Isoniazid inhibits InhA (mycolic acid synthesis) and ethambutol inhibits arabinosyl transferase (arabinogalactan synthesis), both specifically targeting this cell wall.
Q: Write the immunological/physiological basis of granuloma formation in TB. (Physiology AIT)
Answer: TB granuloma formation is a Th1-mediated process. After M. tuberculosis is phagocytosed by alveolar macrophages, it survives by blocking phagolysosome fusion (via sulfolipids, LAM). At ~3 weeks, macrophages present MTB antigens via Class II MHC to CD4+ T cells in draining lymph nodes. IL-12 from macrophages drives Th1 differentiation. Th1 cells release IFN-γ, which activates macrophages to produce: (1) reactive nitrogen intermediates (via iNOS) - main mycobactericidal mechanism, (2) reactive oxygen species, (3) TNF - recruits more monocytes and promotes granuloma formation. IFN-γ also induces differentiation of macrophages into epithelioid histiocytes, which aggregate to form the granuloma core. Some fuse into Langhans giant cells. The mature granuloma - with central caseous necrosis, epithelioid cells, giant cells, and a cuff of lymphocytes - represents an equilibrium between mycobacterial persistence and host immune containment.
Q: Describe the Ghon complex. What are its anatomical components and fate? (Anatomy AIT)
Answer: The Ghon complex is the primary anatomical lesion of tuberculosis in a previously unsensitized individual. It comprises: (1) Ghon focus - a 1-1.5 cm area of gray-white consolidation with central caseous necrosis, located in the lower part of the upper lobe or upper part of the lower lobe, close to the pleura. (2) Regional lymphadenopathy - caseating hilar/mediastinal lymph nodes, as bacilli travel via lymphatics. Together, the pulmonary focus and caseating lymph nodes constitute the Ghon complex. Fate: In ~95% of cases, cell-mediated immunity develops, the lesion undergoes fibrosis and calcification → Ranke complex (visible on CXR). Bacilli remain dormant (latent TB). In the remaining 5%, or in immunocompromised patients, progressive primary TB develops with possible hematogenous dissemination → miliary TB, TB meningitis, etc.
Sources: Robbins & Kumar Basic Pathology 11e; Medical Microbiology 9e (Murray); Sherris & Ryan's Medical Microbiology 8e; Dermatology 5e (Griffiths); Murray & Nadel's Textbook of Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.