Acute pancreatitis
Reading File
Finding Sources
Searching PubMed
"acute pancreatitis"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile a complete, well-structured response.
Acute Pancreatitis
A comprehensive review drawn from Sleisenger & Fordtran's GI and Liver Disease, Schwartz's Principles of Surgery, Current Surgical Therapy, Grainger & Allison's Diagnostic Radiology, and Rosen's Emergency Medicine.
Definition & Epidemiology
Acute pancreatitis (AP) is a sudden inflammatory disease of the pancreas triggered by premature activation of digestive enzymes within acinar cells, causing autodigestion. It accounts for approximately 111 hospitalizations per 100,000 persons/year (US data), and 80% of cases are mild and self-limiting. However, up to 20% are severe and life-threatening.
Etiology
The classic mnemonic is "I GET SMASHED":
| Cause | Notes |
|---|---|
| Gallstones | Most common overall (~40%). Stone/sludge impaction at the ampulla of Vater |
| Alcohol | Second most common (~30%). Chronic use more than acute binge |
| Hypertriglyceridemia | Triglycerides >1000 mg/dL; serum amylase may be falsely normal |
| Hypercalcemia | Any cause; activates trypsinogen |
| ERCP (post-procedure) | Most common iatrogenic cause |
| Trauma | Blunt abdominal injury; often missed in severely injured patients |
| Medications | Valproate, L-asparaginase, azathioprine/6-MP, thiazides, steroids, tetracyclines |
| Infections | Mumps, CMV, Coxsackievirus, Mycoplasma, Ascaris (in endemic areas) |
| Autoimmune / Structural | Pancreas divisum, autoimmune pancreatitis |
| Genetic | SPINK1, CFTR, PRSS1 mutations (esp. in recurrent/hereditary cases) |
| Idiopathic | ~5-15% of cases |
- Sleisenger & Fordtran's, p. 174; Grainger & Allison's, p. 677
Pathophysiology
The central event is premature activation of trypsinogen to trypsin within pancreatic acinar cells (normally a strictly extracellular event). This triggers a cascade:
- Acinar cell injury (oxidative stress, ductal obstruction, alcohol toxicity)
- Intracellular trypsin activation
- Trypsin activates other pro-enzymes: phospholipase A2, elastase, chymotrypsin
- Local inflammation, acinar cell necrosis, fat necrosis
- Systemic inflammatory response syndrome (SIRS) - cytokine release (IL-1, IL-6, TNF-a)
- Distant organ failure (ARDS, AKI, cardiovascular collapse)
Clinical Presentation
| Feature | Details |
|---|---|
| Pain | Acute onset, severe, constant epigastric pain radiating to the back/left scapula; described as "boring through to the back" |
| Nausea/Vomiting | Universal |
| Position | Patient leans forward to relieve pain (anteflexion position) |
| Fever | Usually low grade; high fever suggests infected necrosis |
| Tachycardia / Tachypnea | Reflect SIRS and third-space fluid losses |
| Abdominal exam | Hypoactive bowel sounds, epigastric tenderness, guarding/rigidity (variable) |
Rare but classic signs (indicate retroperitoneal hemorrhage/necrosis):
- Cullen's sign - periumbilical ecchymosis
- Grey Turner's sign - flank ecchymosis
Diagnosis
Diagnosis requires 2 of 3 of the following (Revised Atlanta Criteria):
- Abdominal pain strongly suggestive of AP
- Serum amylase and/or lipase ≥3x upper limit of normal
- Characteristic findings on imaging (CT/MRI)
Amylase: Rises within hours, peaks quickly, returns to normal in 3-5 days. No correlation between magnitude and severity. Can be falsely normal in hypertriglyceridemia or severe necrosis (burnt-out pancreas).
Lipase: More specific and remains elevated longer than amylase. Preferred enzyme.
Other labs: WBC 12,000-20,000, elevated BUN/creatinine (hemoconcentration), hyperglycemia, elevated LDH/AST, hypoalbuminemia, hypocalcemia (saponification).
- Schwartz's Surgery, p. 1471-1472
Imaging
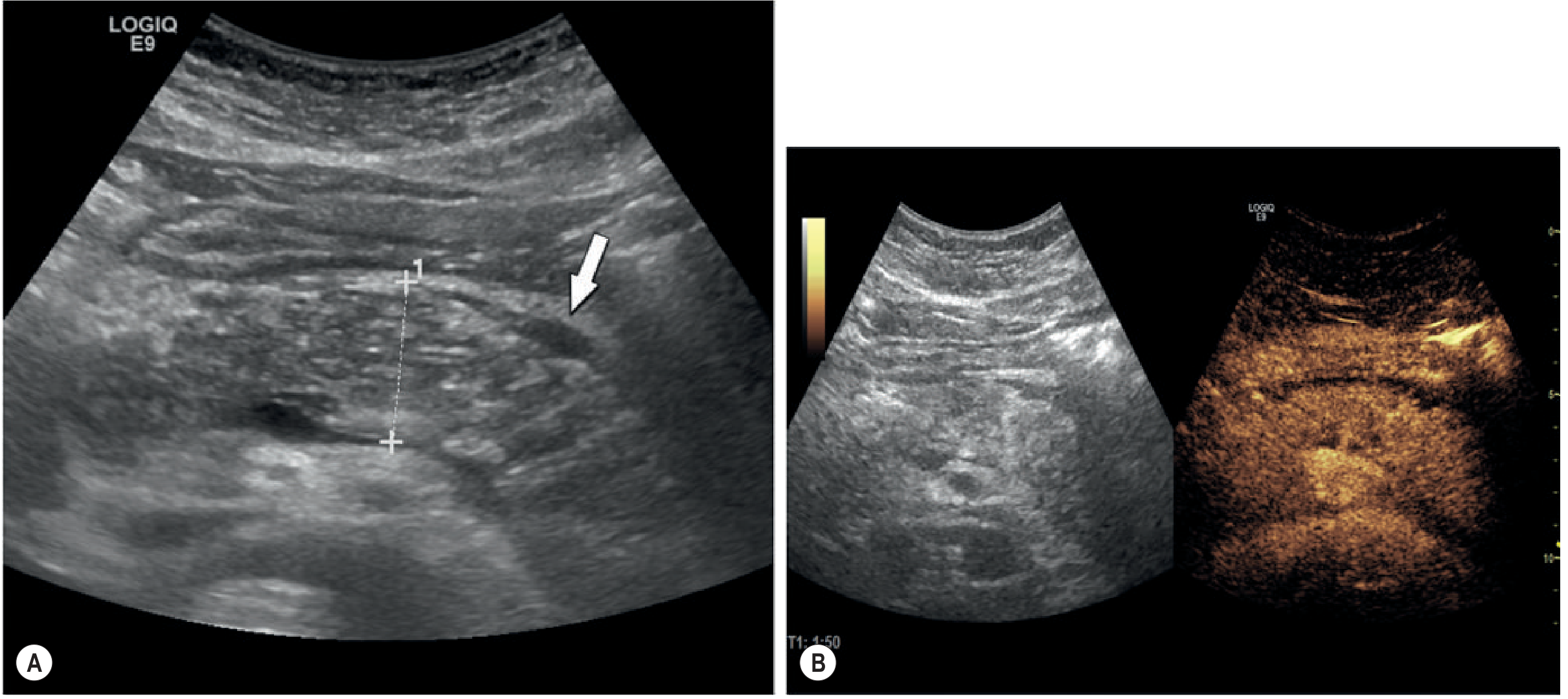
Ultrasound (first-line initial study)
Best for identifying gallstones as etiology. In edematous pancreatitis: diffuse pancreatic enlargement with reduced reflectivity and peripancreatic fluid (below). US cannot reliably detect necrosis.
Contrast-Enhanced CT (CECT) - gold standard for severity
- Indicated when: diagnosis is uncertain, or severe/complicated disease
- NOT routinely needed in mild AP
- Best done 48-72 hours after onset (severity may underestimate early)
- Distinguishes interstitial edematous from necrotizing pancreatitis
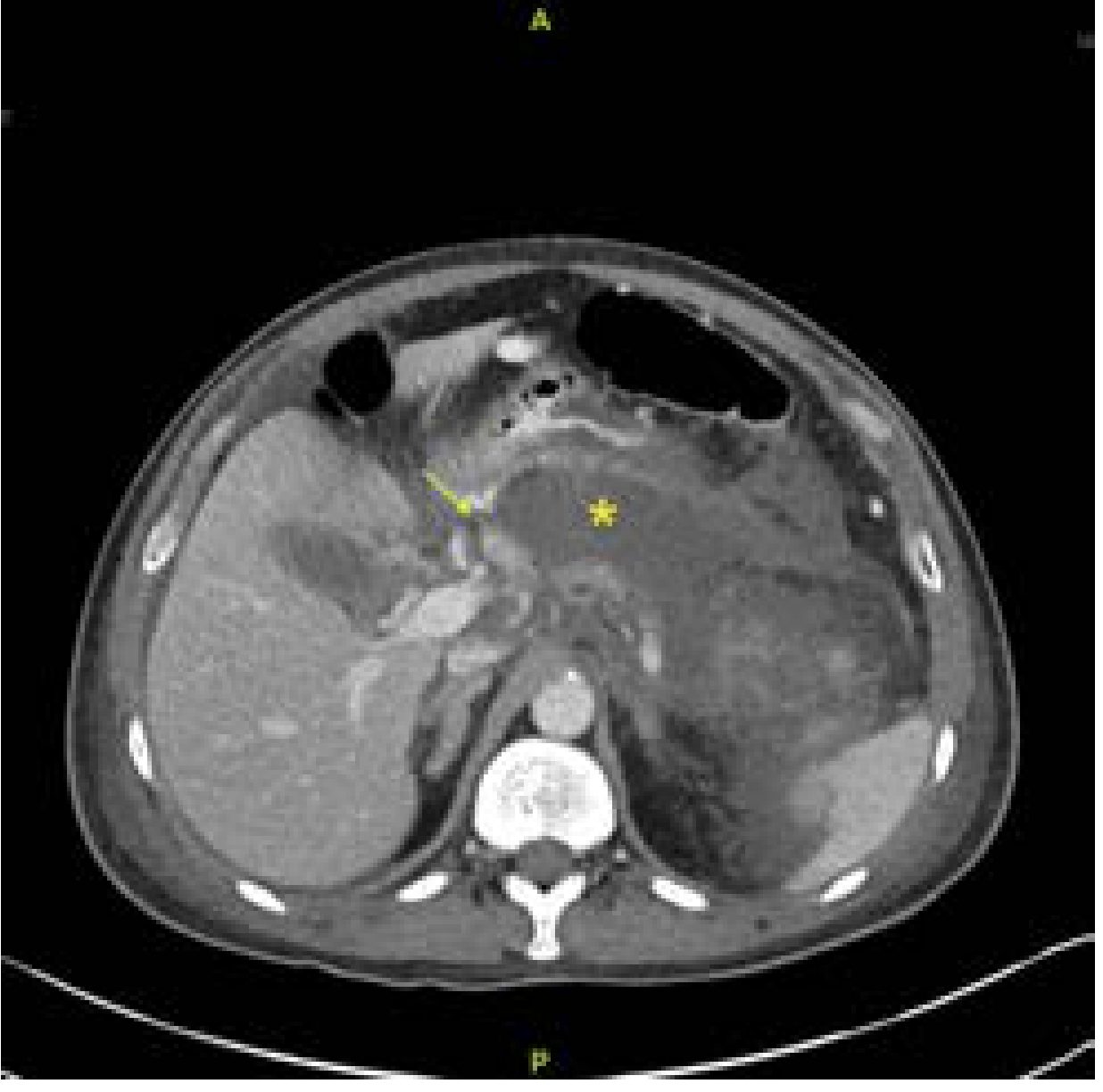
Gas within a necrotic collection = infected necrosis (surgical emergency indicator).
MRI/MRCP
Preferred over CT for: pregnant patients, renal impairment, evaluating ductal anatomy, detecting bile duct stones without ERCP.
Severity Classification (2012 Revised Atlanta Classification)
| Grade | Organ Failure | Local/Systemic Complications | Mortality |
|---|---|---|---|
| Mild | Absent | Absent | Very rare (<5%) |
| Moderately Severe | Transient (<48 hr) | Present, without persistent OF | Low |
| Severe | Persistent (>48 hr) | Present | High: 36-50%; extremely high with infected necrosis |
- Current Surgical Therapy, Table 1; Schwartz's, p. 1472
Scoring Systems
Ranson's Criteria
Scored over 48 hours. ≥3 criteria = severe disease.
| On Admission | At 48 Hours |
|---|---|
| Age >55 years | Hematocrit fall >10% |
| WBC >16,000 | BUN rise >5 mg/dL |
| Blood glucose >200 mg/dL | Serum Ca <8 mg/dL |
| LDH >350 IU/L | PaO₂ <60 mmHg |
| AST >250 IU/L | Base deficit >4 mEq/L |
| Fluid sequestration >6 L |
Score ≥6: mortality ~50%.
BISAP Score (within 24 hours)
BUN >25 mg/dL | Impaired mental status (GCS <15) | SIRS | Age >60 | Pleural effusion
Score ≥3 = high mortality risk. Simpler but comparable accuracy.
APACHE II
Score ≥8 at 24h has similar accuracy to Ranson's.
CT Severity Index (CTSI)
Balthazar grade (A-E) + % necrosis score. Correlates with morbidity and mortality.
Local Complications (Revised Atlanta Nomenclature)
| Complication | Type | Timing | Features |
|---|---|---|---|
| APFC (Acute Peripancreatic Fluid Collection) | Interstitial | <4 weeks | Non-encapsulated, no necrosis; most resolve spontaneously |
| Pseudocyst | Interstitial | >4 weeks | Encapsulated, no solid debris, wall well-defined |
| ANC (Acute Necrotic Collection) | Necrotizing | <4 weeks | Mixed fluid + necrosis |
| WON (Walled-Off Necrosis) | Necrotizing | >4 weeks | Encapsulated necrosis; may become infected |
Other local complications: hemorrhagic pancreatitis, splenic/portal vein thrombosis, pseudoaneurysms, gastric outlet obstruction, colonic infarction (middle/right colic artery - presents as rapid hemodynamic collapse; requires emergent laparotomy).
Management
General Principles
Accurate diagnosis, appropriate triage, high-quality supportive care, and monitoring for/treatment of complications.
1. Pain Control
- Mild pain: NSAIDs (e.g., metamizole 2 g IV q8h)
- Severe pain: Opioids IV (buprenorphine, pentazocine, meperidine)
- Avoid morphine - may cause sphincter of Oddi spasm
2. Fluid Resuscitation
- Most important early intervention
- Ringer's Lactate is preferred - has anti-inflammatory effects, reduces metabolic acidosis compared to normal saline
- Rate: 5-10 mL/kg/hour, titrated to goals
- Targets: HR normalization, MAP, urine output >0.5 mL/kg/hr
- Severe AP: target CVP 8-12 mmHg, mixed venous O₂ sat ≥70%
- Monitor for volume overload (tachypnea, hypoxia, edema, pleural effusion)
3. Nutrition
- Early enteral nutrition is preferred over parenteral (fewer infectious complications, lower cost)
- Nasogastric (NG) feeding is as effective as nasojejunal in most patients
- Nasojejunal preferred if gastric retention from duodenal edema
- TPN only if enteral feeding is not tolerated
- Prior practice of "pancreatic rest"/NPO is no longer recommended
4. Antibiotics
- Prophylactic antibiotics are NOT recommended - necrosis is initially sterile, and prophylaxis promotes resistant organisms
- Indicated when infected necrosis is documented (CT gas, positive culture)
- Preferred: Carbapenems (best pancreatic penetration vs. cephalosporins/fluoroquinolones)
- Aim to stabilize, defer intervention for at least 4 weeks to allow WON maturation
5. Role of ERCP
- NOT routinely recommended in acute biliary pancreatitis
- Indicated for: cholangitis or biliary obstruction (hyperbilirubinemia + clinical cholangitis)
- Use MRCP/EUS first to identify CBD stones - prevents unnecessary ERCP
- Early laparoscopic cholecystectomy (within 3 days in mild disease) is standard of care for gallstone pancreatitis
6. Intervention for Pancreatic Necrosis
- Sterile necrosis - conservative management; surgery/drainage not indicated
- Infected necrosis - drainage required; ideally deferred until WON is mature (≥4 weeks)
- Drainage options (step-up approach preferred):
- Percutaneous drainage (CT or US-guided) - first step
- Endoscopic transmural drainage (EUS-guided) - if collection in apposition to stomach/duodenum
- Surgical necrosectomy - minimally invasive video-assisted retroperitoneal debridement (VARD) or open - reserved for failures of minimally invasive approaches
ICU Admission
Transfer to ICU when: persistent tachycardia/hypotension, oliguria, SOFA score deteriorating, multi-organ failure. Target CVP 8-12 mmHg, MVO₂ ≥70%.
Systemic Complications
| Complication | Notes |
|---|---|
| ARDS | Most common cause of early death; PaO₂/FiO₂ <300 |
| AKI | Hemoconcentration + cytokine-mediated renal vasoconstriction |
| Hypocalcemia | Saponification of fat; low Ca <8 mg/dL is a Ranson's criterion |
| Hyperglycemia | Glucagon excess, insulin deficiency |
| Abdominal compartment syndrome | From massive fluid resuscitation + ascites |
| Splanchnic vein thrombosis | Splenic/portal vein; risk of variceal bleeding |
| Colonic infarction | Middle/right colic artery - rare but catastrophic |
Summary of Key Management Points
- Most AP is mild and self-limiting - supportive care, early enteral feeding, Ringer's lactate
- Severity scoring (Ranson's, BISAP, APACHE-II) guides triage to ICU vs. ward
- CECT is the standard for severity assessment but not needed in obvious mild disease
- ERCP only in cholangitis or biliary obstruction - not routine
- Early laparoscopic cholecystectomy for gallstone pancreatitis
- No prophylactic antibiotics - carbapenems only for documented infected necrosis
- Step-up approach for necrosis intervention: percutaneous/endoscopic before surgery
- Morphine avoided due to sphincter of Oddi spasm
Sources: Sleisenger & Fordtran's Gastrointestinal and Liver Disease; Schwartz's Principles of Surgery, 11th ed.; Current Surgical Therapy, 14th ed.; Grainger & Allison's Diagnostic Radiology; Rosen's Emergency Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.