Approach to vertigo
Reading File
Finding Sources
Finding Sources
Searching PubMed
"vertigo" AND "diagnosis" AND "management"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive material. Let me compose the full, structured response.
Approach to Vertigo
Vertigo is the illusion of spinning or motion when no actual movement is occurring. It is the most common subtype of dizziness and most often results from dysfunction of the vestibular system (inner ear or its central connections). The paramount task is to separate life-threatening central causes (stroke, hemorrhage, cerebellar lesion, MS) from the far more common benign peripheral causes (BPPV, vestibular neuritis, Meniere disease).
Step 1 - Classify the Symptom: "Is this truly vertigo?"
Patients use "dizzy" loosely. Distinguish four subtypes before proceeding:
| Type | Sensation | Key Features | Common Causes |
|---|---|---|---|
| Vertigo | Spinning/self-motion | Triggered by head movement; nausea; nystagmus | BPPV, vestibular neuritis, stroke, Meniere |
| Near syncope | Impending blackout | Orthostatic, on standing, tunnel vision | Cardiac, orthostatic hypotension, PE |
| Dysequilibrium | Imbalance / falling | Worse with walking; no spinning | Parkinson, cerebellar disease, B12 deficiency |
| Ill-defined light-headedness | Floating, vague | Often with anxiety, medications | Depression, GAD, medication side effects |
True vertigo (spinning) is most often peripheral vestibular in origin (38-56% of persistent dizziness cases). Central etiologies account for fewer than 10%.
- Symptom to Diagnosis, 4e
Step 2 (Pivotal Step 1) - Screen for Central Causes First
Any patient with unexplained CNS symptoms or signs should be evaluated urgently with MRI.
Ask about and examine for:
- New severe headache or neck pain
- Brainstem symptoms: dysarthria, diplopia, dysphagia, facial weakness, hoarseness
- Cerebellar symptoms: ataxia, incoordination, falls
- Cranial nerve deficits, dysmetria, abnormal Romberg, papilledema
Nystagmus types suggesting central etiology:
- Bidirectional - fast component beats left on left gaze and right on right gaze
- Purely vertical - fast phase beating toward the nose (downbeating) or toward the forehead
- Not suppressed by visual fixation
- Persists > 1 minute or does not fatigue with repetition
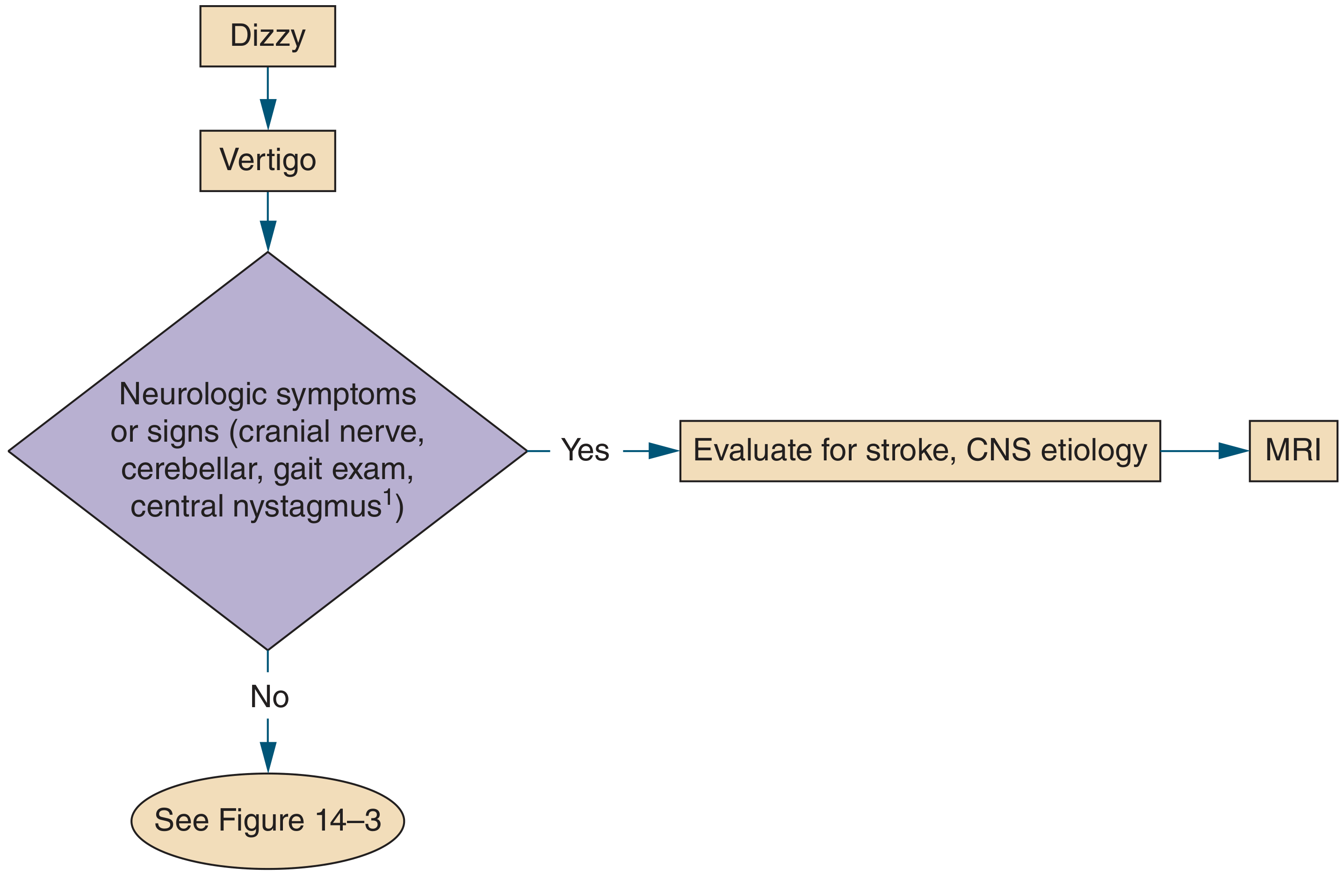
Step 3 (Pivotal Step 2) - Episode Duration + Trigger
For patients without obvious CNS signs, the duration of each individual episode and whether vertigo is triggered (not merely worsened) by head movement are the two most important questions. This separates three distinct clinical patterns:
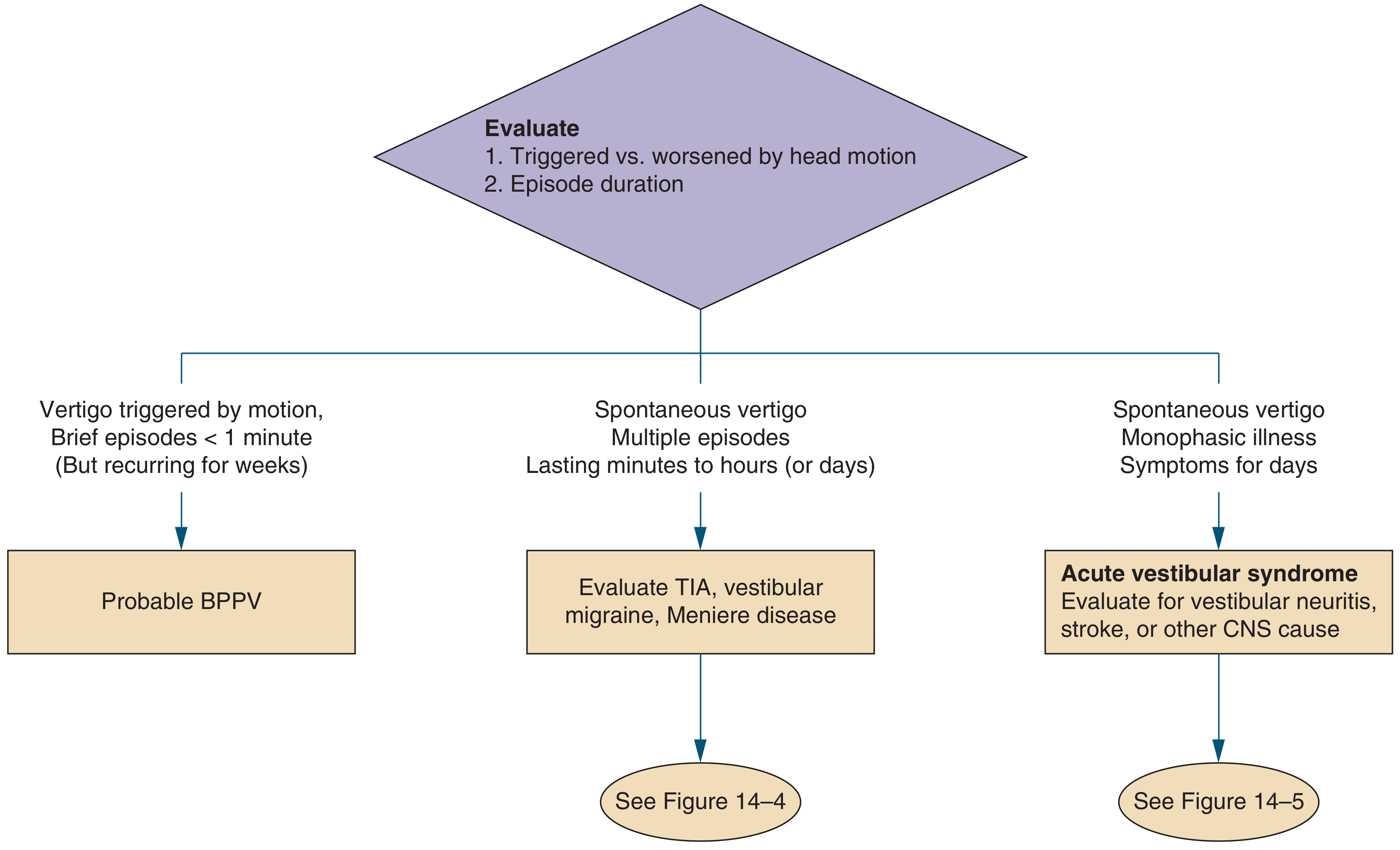
Pattern A: Brief episodes < 1 min, triggered by head motion → BPPV
Pattern B: Spontaneous episodes lasting minutes to hours, recurrent → Meniere disease / Vestibular migraine / TIA
Pattern C: Spontaneous, continuous/monophasic, lasting days → Acute Vestibular Syndrome (vestibular neuritis vs stroke)
Pattern A: BPPV
- Mechanism: Displaced calcium carbonate otoliths (canaliths) within semicircular canals - posterior canal most common (80-90%)
- Classic history: Vertigo on rolling over in bed, looking up at a shelf, extending the neck; lasts < 1 minute; recurs over weeks
- Diagnosis: Dix-Hallpike maneuver - positive if it reproduces vertigo with upbeat-torsional nystagmus with latency of a few seconds and fatigue on repeated testing
- Negative head impulse test (distinguishes from vestibular neuritis)
- Treatment: Epley maneuver (canalith repositioning) - highly effective for posterior canal BPPV; "Barbecue roll" or Gufoni maneuver for horizontal canal variant
- Prognosis: Frequent recurrence (unlike vestibular neuritis)
Pattern B: Recurrent Spontaneous Episodes
| Feature | Meniere Disease | Vestibular Migraine | Posterior Circulation TIA |
|---|---|---|---|
| Duration | 20 min - 12 hours | Minutes to hours | Minutes (< 1 hour) |
| Hearing | Fluctuating low-frequency loss + tinnitus + aural fullness | Normal (usually) | Normal |
| Headache | Absent or mild | Often present; may be headache-free | Absent or present |
| Onset age | 30-60 years | Adolescence to middle age | Older, vascular risk factors |
| Nystagmus | Horizontal | Variable | Variable |
| Other CNS features | None | Photophobia, phonophobia | Diplopia, ataxia, weakness |
TIA must always be considered in older patients with vascular risk factors and new-onset episodic vertigo - VBI can progress to posterior circulation occlusion in the first 24-72 hours. Consider MRA and hospital admission even in stable patients.
- Rosen's Emergency Medicine, 10e
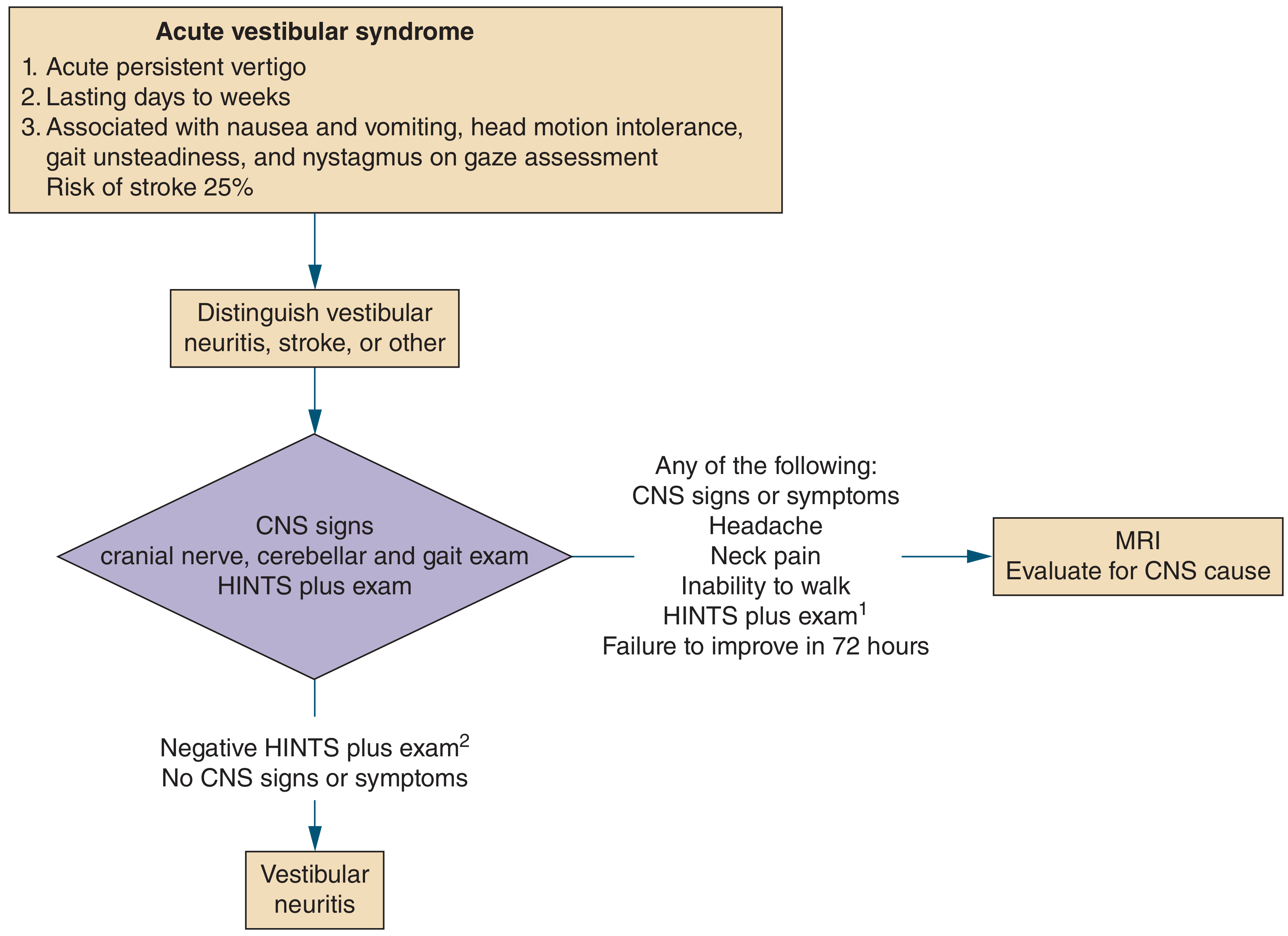
Pattern C: Acute Vestibular Syndrome (AVS)
AVS = acute, persistent vertigo lasting days with nausea, gait unsteadiness, and spontaneous nystagmus. 25% of AVS patients have a posterior fossa stroke - this is the most dangerous diagnostic pitfall.
The HINTS Plus Exam (for AVS with ongoing nystagmus)
HINTS Plus = Head impulse test + Nystagmus + Test of Skew + bedside hearing test. Sensitivity 98%, specificity 85% for stroke - more sensitive than early DWI-MRI.
Only apply HINTS to patients with continuous vertigo AND spontaneous/gaze-evoked nystagmus (not brief positional episodes).
| HINTS Component | Peripheral (Vestibular Neuritis) | Central (Stroke) |
|---|---|---|
| Head Impulse Test | Abnormal - catch-up saccade present (VOR impaired) | Normal - no saccade (VOR intact) |
| Nystagmus | Unidirectional; horizontal-torsional; same direction on all gazes | Direction-changing on lateral gaze; purely vertical or torsional |
| Test of Skew | Negative - no vertical deviation on cover-uncover test | Positive - vertical eye deviation on uncovering |
| Hearing (Plus) | No new hearing loss | New unilateral hearing loss possible |
Key counterintuitive rule: A NORMAL head impulse test in AVS is a RED FLAG for central disease. An abnormal head impulse test (catch-up saccade) is paradoxically reassuring for peripheral disease.
Positive HINTS Plus (any one of: normal HIT, direction-changing nystagmus, vertical skew, new hearing loss) → MRI brain urgently
Peripheral vs Central Vertigo - Summary Comparison
| Feature | Peripheral | Central |
|---|---|---|
| Onset | Sudden | Gradual or sudden |
| Intensity | Severe initially, decreases over time | Mild to severe (severe in stroke) |
| Duration (BPPV) | Seconds to < 1 min | Usually weeks-months (continuous) |
| Duration (VN) | Hours to days | Can be seconds (vascular TIA) |
| Nystagmus direction | Horizontal-torsional; unidirectional | Purely vertical; direction-changing; downbeating |
| Fixation suppression | Suppressed by fixation | Not suppressed |
| Hearing loss | Present in labyrinthitis and Meniere | Absent (usually) |
| Associated neuro signs | Absent | Present (cranial nerves, ataxia, Horner) |
| Head impulse test | Abnormal (catch-up saccade) | Normal |
| Gait | Able to walk (tilts to affected side) | Often cannot walk |
- Rosen's Emergency Medicine, 10e
Physical Examination Checklist
- Vital signs including orthostatic BP
- Otoscopy - tympanic membrane (cholesteatoma, hemotympanum); pneumatic otoscopy (perilymphatic fistula)
- Tuning fork tests (Weber and Rinne) - sensorineural vs conductive hearing loss
- Ocular examination - nystagmus (direction, type, fixation suppression), gaze palsy, INO
- Cranial nerve examination - CN V (facial sensation), CN VII (facial movement), CN IX/X/XII
- Cerebellar exam - finger-nose-finger, dysdiadochokinesis, Romberg
- Gait - tandem walking (wide-based = cerebellar; shuffling = Parkinson)
- Dix-Hallpike maneuver - for suspected BPPV
- HINTS exam - for AVS with spontaneous nystagmus
Differentiating BPPV from Vestibular Neuritis
| Feature | BPPV | Vestibular Neuritis / Labyrinthitis |
|---|---|---|
| Age | More common in older adults | More common in younger patients |
| Hearing loss | None | None (VN); present in labyrinthitis |
| Symptom pattern | Episodic with specific movements | Constant |
| Dix-Hallpike | Positive (upbeat-torsional nystagmus) | May worsen but not classic (avoid test) |
| Head impulse test | Negative | Positive (catch-up saccade) |
| Epley maneuver | Highly effective | Ineffective |
| Recurrence | Frequent | Rare (2-11%) |
- Rosen's Emergency Medicine, 10e
Management
BPPV
- Epley maneuver (posterior canal): 4-5 sequential head rotations, each held ~30 seconds
- Barbecue roll / Gufoni maneuver: horizontal canal variant
- Vestibular suppressants are not routinely recommended for BPPV (per guidelines)
- Discharge with Epley self-maneuver instructions
Vestibular Neuritis
- Supportive: antiemetics, hydration
- Short course of oral corticosteroids (methylprednisolone) may reduce severity and speed recovery
- Avoid benzodiazepines on discharge - they interfere with vestibular compensation/habituation
- Vestibular rehabilitation exercises
Acute Central Vertigo (stroke, cerebellar hemorrhage)
- Emergent CT if hemorrhage suspected (cerebellar bleed = neurosurgical emergency)
- MRI with DWI preferred for posterior fossa infarction (CT misses ~50% of posterior fossa strokes acutely)
- Neurology/neurosurgery consultation
- Antithrombotic therapy per stroke guidelines if ischemic
Meniere Disease
- Low-salt diet, diuretics (hydrochlorothiazide/acetazolamide)
- Acute attacks: vestibular suppressants
- Intratympanic gentamicin or steroids for refractory cases
Medications for Acute Vertigo
| Drug | Dose | Antiemetic Effect |
|---|---|---|
| Ondansetron (Zofran) | 4 mg IV/PO | Prominent - preferred first-line IV |
| Promethazine (Phenergan) | 12.5-25 mg IM/PO/PR | Moderate (IV boxed warning - avoid) |
| Prochlorperazine (Compazine) | 5-10 mg IV/IM/PO | Prominent |
| Dimenhydrinate (Dramamine) | 50-100 mg IM/IV/PO | Moderate |
| Meclizine (Antivert) | 12.5-50 mg PO q4-6h | Mild - onset ~1 hour |
| Lorazepam | 1-2 mg IV (intractable) | Mild - reserve for refractory vomiting |
| Metoclopramide (Reglan) | 5-10 mg IV/IM/PO | Prominent |
Ondansetron IV is recommended as first-line - comparable efficacy to promethazine IM with fewer side effects. Benzodiazepines impair vestibular compensation and should not be prescribed for discharge in vestibular neuritis.
- Rosen's Emergency Medicine, 10e
"Must Not Miss" Diagnoses in Vertigo
| Diagnosis | Red Flags | Action |
|---|---|---|
| Cerebellar hemorrhage | Sudden severe headache, vomiting, truncal ataxia, unable to walk | Emergency CT; neurosurgery |
| Posterior inferior cerebellar artery (PICA) infarct - Wallenberg syndrome | Ipsilateral facial sensory loss, contralateral body pain/temperature loss, Horner syndrome, hoarseness | MRI; stroke pathway |
| Vertebrobasilar TIA | Older patient, vascular risk factors, episodic vertigo with diplopia/dysarthria | MRA; admit for monitoring |
| Vertebral artery dissection (VAD) | Neck pain/headache + vertigo after trauma or chiropractic manipulation | MRA/CTA neck vessels urgently |
| Multiple sclerosis | Young patient, relapsing symptoms, INO (adducting eye lags on lateral gaze) | MRI brain + spine |
| Acoustic neuroma | Progressive unilateral sensorineural hearing loss + tinnitus | MRI with gadolinium |
Sources: Symptom to Diagnosis: An Evidence-Based Guide, 4e | Rosen's Emergency Medicine, 10e | Tintinalli's Emergency Medicine, 9e | Textbook of Family Medicine, 9e
This is a shared conversation. Sign in to Orris to start your own chat.