Uncomplicated malaria short note for mbbs pedia exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed to write a comprehensive short note on uncomplicated malaria for an MBBS pediatrics exam. Let me compile the answer.
Uncomplicated Malaria - Short Note (MBBS Pediatrics)
Definition
Uncomplicated malaria is a symptomatic malaria infection (due to any Plasmodium species) without signs of severe organ dysfunction or high parasite burden. The patient can tolerate oral therapy and does not meet WHO criteria for severe/complicated malaria.
Etiology and Epidemiology
| Species | Erythrocytic Cycle | Fever Pattern | Chloroquine Resistance | Relapse |
|---|---|---|---|---|
| P. falciparum | 48 h | Irregular/tertian | Yes | No |
| P. vivax | 48 h | Benign tertian | Rare | Yes (hypnozoites) |
| P. ovale | 48 h | Ovale tertian | No | Yes (hypnozoites) |
| P. malariae | 72 h | Quartan | No | No |
| P. knowlesi | ~24 h | Daily | No | No |
- Vector: Female Anopheles mosquito (bites at dusk/night)
- In endemic areas, malaria primarily affects children; adults develop immunity with repeated exposure
- In highly endemic areas, a large proportion of children carry asymptomatic parasitemia; illness is commonly mild but occasionally severe
Life Cycle
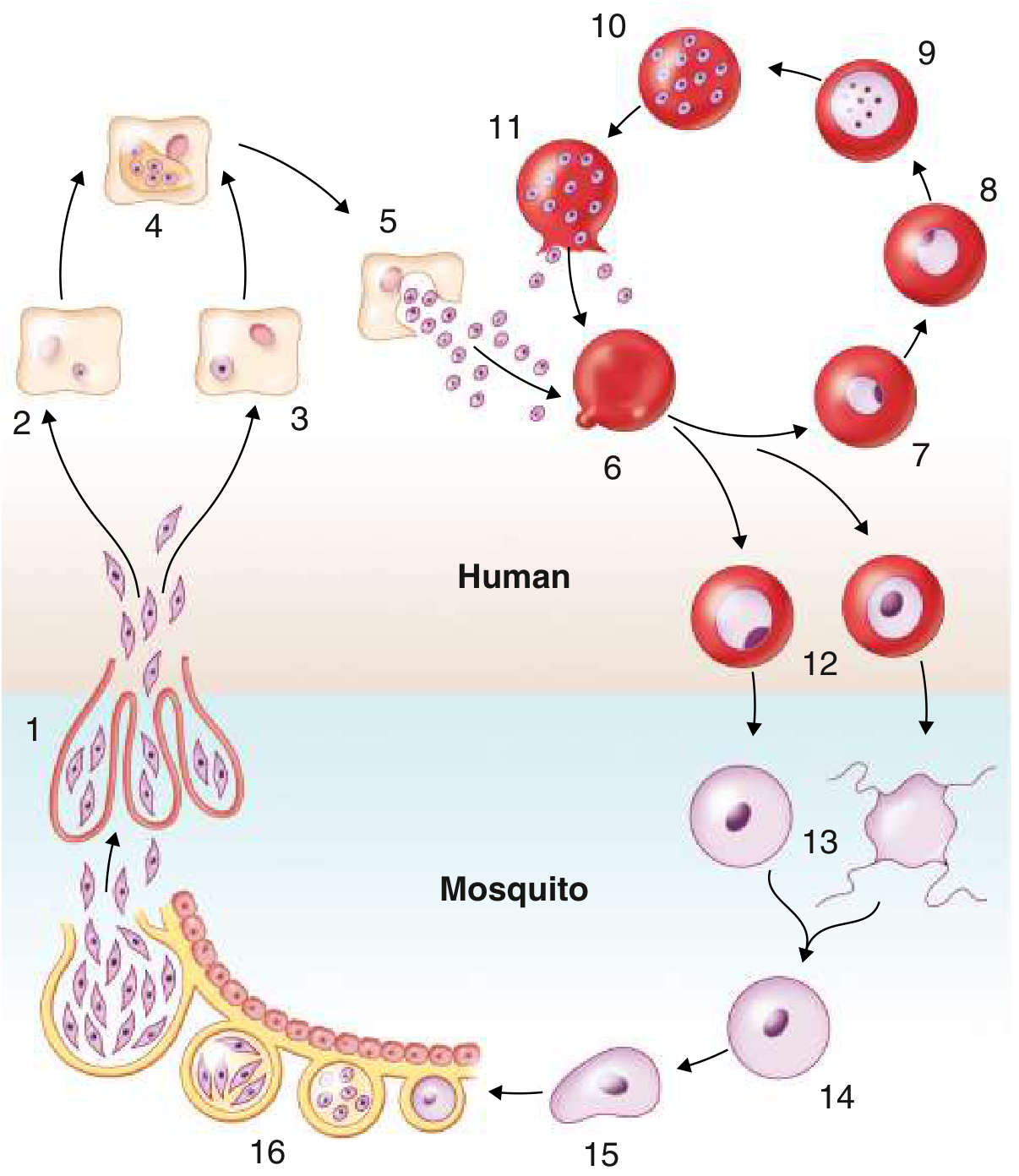
Goldman-Cecil Medicine, Fig. 316-1
- Mosquito bite - sporozoites injected into bloodstream
- Pre-erythrocytic (liver) stage - sporozoites infect hepatocytes → tissue schizonts → merozoites released (P. vivax/ovale also form dormant hypnozoites*)
- Erythrocytic stage - merozoites invade RBCs → ring stage → trophozoite → schizont → RBC rupture releases merozoites + pyrogens → FEVER
- Sexual stage - some merozoites form gametocytes → ingested by mosquito → fertilization → oocyst → sporozoites migrate to salivary gland
Pathophysiology of Fever
Fever is caused by rupture of infected RBCs and release of merozoites and malarial toxins (GPI anchors, hemozoin). These trigger macrophage release of TNF-α, IL-1, IL-6, and IL-12, causing the febrile paroxysm. As erythrocytic cycles synchronize, fever becomes periodic:
- Tertian fever (every 48 h) - P. vivax, P. ovale, P. falciparum
- Quartan fever (every 72 h) - P. malariae
Clinical Features
Classic Malarial Paroxysm (three stages)
- Cold stage - sudden onset rigors, chills, teeth chattering (lasts 15-60 min)
- Hot stage - high fever (39-41°C), flushed, dry skin, headache, vomiting (lasts 2-6 h)
- Sweating stage - profuse diaphoresis, temperature falls, patient exhausted (lasts 2-4 h)
Note: Classic paroxysms are often absent in P. falciparum or in patients who received partial chemoprophylaxis.
Other Features
- Prodrome: Malaise, myalgia, headache, anorexia (often mistaken for influenza or gastroenteritis)
- GI symptoms: Nausea, vomiting, abdominal pain common in children
- Splenomegaly: Common; progressive with repeated infections
- Hepatomegaly: Variable
- Anemia: Normocytic normochromic; due to RBC destruction + dyserythropoiesis
- Thrombocytopenia: Frequent but usually does not cause bleeding
- No lymphadenopathy, no rash (if present, consider alternative/co-existing diagnosis)
In Children Specifically
- Febrile seizures more common
- GI symptoms predominate (diarrhea, vomiting)
- Rapidly developing severe anemia more common than in adults
- High parasite density correlates with likelihood of true malaria disease (vs asymptomatic parasitemia)
Investigations
Confirmatory (Gold Standard)
1. Peripheral Blood Smear (PBS) - Thick and Thin
- Thick smear: Detects and quantifies parasitemia (more sensitive)
- Thin smear: Species identification and morphology
- Key morphological features:
| Species | RBC size | Inclusions | Gametocyte |
|---|---|---|---|
| P. falciparum | Normal | Maurer's clefts; multiple ring forms/RBC; "headphone" rings | Banana-shaped (crescent) |
| P. vivax | Enlarged | Schuffner's dots (fine); amoeboid trophozoite | Round |
| P. ovale | Oval, fimbriated | Schuffner's dots (coarser) | Round |
| P. malariae | Normal | "Band form" trophozoite | Round |
2. Rapid Diagnostic Test (RDT)
- Detects P. falciparum HRP-2 antigen (or LDH for non-falciparum)
- Quick (~15 min), no microscopy needed
- Cannot quantify parasitemia; false negatives in high parasitemia (hook effect with HRP-2 deletion mutants)
3. PCR - Most sensitive and specific; used for species confirmation and epidemiology; not routine bedside
Supportive Investigations
| Test | Expected Finding |
|---|---|
| CBC | Anemia (normocytic), thrombocytopenia, leukopenia or normal WBC |
| Peripheral smear | Parasitized RBCs |
| LFTs | Mild elevation (bilirubin ↑ due to hemolysis) |
| Blood glucose | May be low (especially P. falciparum + quinine) |
| RFTs | Usually normal in uncomplicated disease |
| Urine | May show hemoglobinuria in falciparum |
WHO Criteria: Uncomplicated vs Complicated Malaria
Uncomplicated malaria = fever + confirmed parasitemia + none of the following:
- Prostration / inability to sit
- Altered consciousness / seizures
- Severe anemia (Hb <7 g/dL in children)
- Respiratory distress / pulmonary edema
- Hypoglycemia (<2.2 mmol/L)
- Hemoglobinuria / jaundice
- Abnormal bleeding / shock
- Parasitemia >5% or >200,000 parasites/μL
Treatment
1. P. falciparum (chloroquine-resistant areas - most of the world)
First-line: Artemisinin-Based Combination Therapy (ACT)
| Drug | Dose (Adults) | Notes |
|---|---|---|
| Artemether-Lumefantrine (Coartem) | 4 tabs twice daily × 3 days | Most widely used; FDA-approved; give with fat-containing food |
| Artesunate-Amodiaquine (ASAQ) | 3 days | First-line in many African countries |
| Artesunate-Mefloquine | 3 days | Southeast Asia |
| Dihydroartemisinin-Piperaquine | 3 days | Resistance emerging in SE Asia |
Alternatives (if ACT unavailable):
- Quinine 650 mg TDS × 7 days + Doxycycline 100 mg BD × 7 days (avoid doxycycline in children <8 yrs - use clindamycin instead)
- Atovaquone-Proguanil (Malarone) 4 tabs/day × 3 days
Pediatric dosing (Artemether-Lumefantrine) - weight-based:
- 5-14 kg: 1 tab BD × 3 days
- 15-24 kg: 2 tabs BD × 3 days
- 25-34 kg: 3 tabs BD × 3 days
-
34 kg: 4 tabs BD × 3 days
2. P. vivax / P. ovale (chloroquine-sensitive areas)
-
Chloroquine: 10 mg base/kg stat, then 5 mg base/kg at 6, 24, 48 h
-
PLUS Primaquine (to eradicate hypnozoites and prevent relapse):
- 0.25 mg base/kg/day × 14 days
- Check G6PD status first - primaquine causes hemolysis in G6PD deficiency
- Contraindicated in pregnancy and infants <6 months
-
For chloroquine-resistant P. vivax (parts of SE Asia): Use ACT
3. P. malariae and P. knowlesi
- Chloroquine (as above); no primaquine needed (no hypnozoites)
Key Points for Exam
- Most common cause of fever in tropics in children
- Gold standard diagnosis = Peripheral blood smear (thick + thin)
- Banana-shaped gametocytes = P. falciparum (pathognomonic)
- Schuffner's dots = P. vivax and P. ovale
- Relapse (due to hypnozoites) - P. vivax and P. ovale only; treat with primaquine after checking G6PD
- ACT is first-line for P. falciparum uncomplicated malaria globally
- Doxycycline is avoided in children <8 years - use clindamycin instead
- Classic paroxysm (cold → hot → sweating) is often absent in P. falciparum
- Thrombocytopenia + fever + travel history = think malaria
- Do NOT use steroids in cerebral malaria (worsens outcomes)
Prognosis
- Uncomplicated P. falciparum malaria: mortality ~0.1% with prompt treatment
- Untreated or delayed P. falciparum: can progress to cerebral malaria (mortality 15-25%)
- Non-falciparum malaria: excellent prognosis with treatment
Sources: Goldman-Cecil Medicine International Edition; Tintinalli's Emergency Medicine; Goodman & Gilman's Pharmacological Basis of Therapeutics; Katzung's Basic and Clinical Pharmacology, 16th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.