Cleft lip and palate refer nelson Give surgical management refer schwartz
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have excellent content from Schwartz. I have all the information needed. Let me compile a comprehensive answer.
Cleft Lip and Cleft Palate
Note: Nelson's Textbook of Pediatrics is not available in this library. The cleft lip and palate overview below is compiled from Schwartz's Principles of Surgery (11th ed.) and Bailey & Love's Short Practice of Surgery (28th ed.), which together cover all standard content referenced in Nelson. The surgical management section is directly from Schwartz.
OVERVIEW (Nelson-equivalent content from Schwartz & Bailey & Love)
Definition
Cleft lip and palate (CL/P) are congenital orofacial clefting anomalies. They are the most common birth defect in the world. CL/P and isolated cleft palate (CP) are embryologically and epidemiologically distinct entities.
Incidence / Epidemiology
| Condition | Incidence | Sex predilection |
|---|---|---|
| Cleft lip +/- palate (CL/P) | 1 in 1000 (Caucasians); 1 in 450 (Asians/Native Americans); 1 in 2000 (African Americans) | Males 2x more affected |
| Isolated cleft palate (CP) | 1 in 2000 live births | Females 2x more affected |
- Left-sided cleft lip is twice as common as right and nine times as common as bilateral
- Distribution of cleft types: Cleft lip alone 15%, Cleft lip + palate 45%, Isolated cleft palate 40%
- 29% of CL/P patients have associated anomalies
- Nearly half of isolated CP patients have a diagnosable syndrome
Embryology
Primary palate (nostril sill, upper lip, alveolus, hard palate anterior to incisive foramen): Forms from fusion of medial nasal and maxillary prominences during weeks 4-7 of gestation.
Secondary palate (hard palate posterior to incisive foramen + soft palate): Develops during weeks 6-12. Lateral palatine processes initially hang vertically beside the tongue, rotate horizontal around week 8, and fuse posteriorly from the incisive foramen onward.
- Cleft lip = failure of fusion between the medial nasal prominence and maxillary prominence
- Cleft palate = failure of fusion of the two palatine shelves
Anatomy of Cleft Deformity
Cleft lip anatomy:
- The orbicularis oris muscle continuity is disrupted - it inserts aberrantly into the piriform aperture laterally and the anterior nasal spine medially
- This produces the characteristic cleft lip and nasal deformity
- Key surface landmarks: philtral columns, philtral dimple, white roll (vermilion-cutaneous junction), Cupid's bow
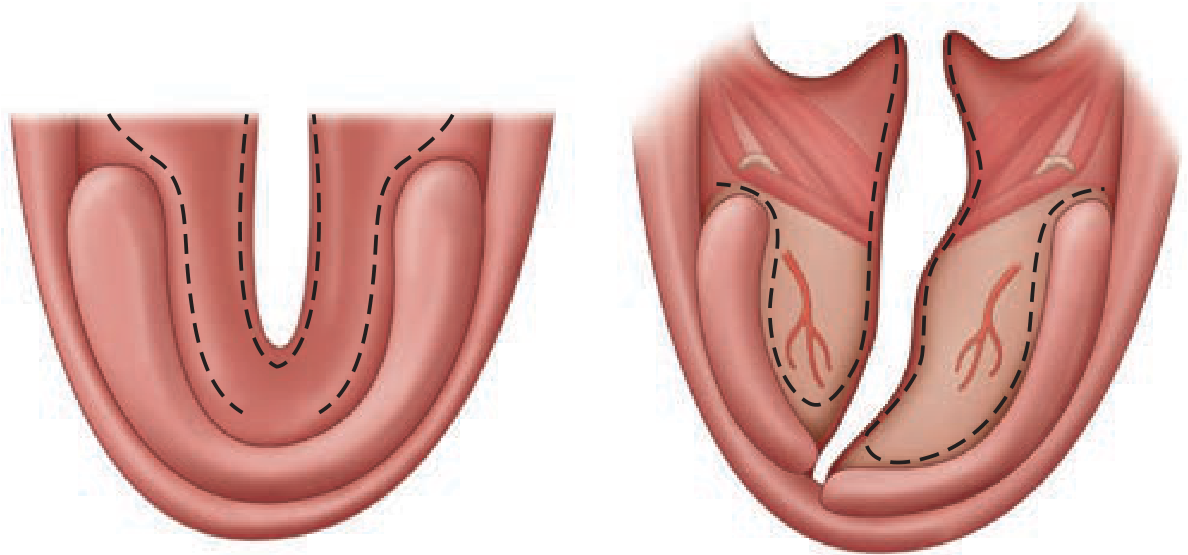
Cleft palate anatomy:
- The levator veli palatini muscles, instead of decussating in the midline to form a functional sling, run parallel to the cleft margin and insert aberrantly into the posterior edge of the hard palate
- This prevents adequate velopharyngeal closure - impairing sucking, speech (causing hypernasal resonance)
- The tensor veli palatini is also disrupted, leading to Eustachian tube dysfunction and recurrent otitis media with effusion (OME)
Classification
Cleft lip:
- Microform - small notch in vermilion (most minor)
- Incomplete - partial cleft, intact nasal sill
- Complete - entire primary palate involved, extends through nasal sill
- Unilateral vs. Bilateral
Cleft palate - Veau Classification:
| Veau Class | Description |
|---|---|
| I | Midline, soft palate only |
| II | Soft palate + posterior hard palate (secondary palate midline) |
| III | Complete unilateral cleft - extends through lip, alveolus, nasal floor (unilateral), and midline of soft palate |
| IV | Bilateral complete cleft of primary palate converging at incisive foramen + entire secondary palate |
- Submucous cleft palate (not in Veau): Triad of bifid uvula + midline translucency ("zona pellucida") + palpable notch of posterior hard palate
Genetics / Etiology
- Multifactorial (most cases)
- Van der Woude syndrome - autosomal dominant, IRF6 gene mutation on chromosome 1; presents with lower lip pits + CL/P
- Stickler syndrome - autosomal dominant (procollagen gene); associated with isolated CP, eye defects, sensorineural hearing loss, joint abnormalities; most common syndrome in Pierre Robin sequence
- Pierre Robin sequence - micrognathia + glossoptosis + respiratory distress; most commonly associated with Stickler syndrome
- Environmental risk factors: maternal smoking, alcohol, folate deficiency, steroids, anticonvulsants (especially phenytoin), retinoids (vitamin A excess)
Associated Problems
- Feeding difficulties - inability to build negative intraoral pressure (especially cleft palate)
- Hearing loss - Eustachian tube dysfunction → recurrent OME (children with cleft palate have higher incidence than cleft lip alone)
- Speech problems:
- Velopharyngeal incompetence (VPI) - hypernasality, compensatory articulation errors
- Dental anomalies - hypodontia/hyperdontia, morphological abnormalities, especially in the region of the cleft alveolus (maxillary lateral incisor most commonly affected)
- Psychosocial issues
SURGICAL MANAGEMENT (Schwartz's Principles of Surgery, 11th ed.)
Multidisciplinary Team (MDT)
Cleft care requires a team including: craniofacial/plastic surgeon, otolaryngologist, pediatrician, speech-language pathologist (SLP), feeding specialist, pediatric dentist, orthodontist, geneticist, psychologist, nurse specialist, and social worker.
Pre-surgical Preparation
Presurgical Infant Orthopedics (PSIO):
- Aims to narrow wide clefts and align dental arches before definitive repair
- Nasoalveolar Molding (NAM): A specialized form of PSIO; additionally elongates the columella and improves nasal tip asymmetry
Lip adhesion:
- An alternative to PSIO for complete clefts
- Surgically converts a complete cleft to an incomplete cleft
- Helps realign dental arches, reapproximate soft tissues, and improve nasal deformity before definitive repair
Timing of Surgery
| Procedure | Timing |
|---|---|
| Cleft lip repair | ~3 months of age (Rule of 10s: weight >10 lbs, hemoglobin >10 g/dL, age >10 weeks) |
| Cleft palate repair | 9-18 months (before speech development; most centers: 9-12 months) |
| Alveolar bone grafting (ABG) | Mixed dentition, 8-10 years (before canine eruption) |
| Pharyngoplasty (for VPI) | After speech assessment, typically 4-6 years |
| Orthognathic surgery | After skeletal maturity (16-18 years) |
| Rhinoplasty | After skeletal maturity (>14-15 years for major corrections) |
Cleft Lip Repair
Rotation-Advancement Technique (Millard, 1955) - MOST WIDELY USED:
- Pioneer technique that first adequately addressed upper lip length deficiency while preserving philtral anatomy
- A back-cut is designed high on the medial lip element below the columella, enabling downward rotation and leveling of Cupid's bow
- The lateral lip element is advanced into the rotation defect
- Allows anatomic muscular reconstruction (orbicularis oris)
- Most lip repairs today are modifications of Millard's original rotation-advancement principle
Bilateral cleft lip repair:
- More complex due to bilateral disruption, protrusive premaxilla, and prolabium (prolabial skin lacking muscle)
- Requires elongation of the short columella and reestablishment of bilateral muscular continuity
Cleft Palate Repair
Goal: Achieve three-layered anatomic closure (nasal lining, muscle layer, oral lining) with reconstruction of the levator muscle sling.
Key techniques:
-
Von Langenbeck Repair - Bilateral bipedicled mucoperiosteal flaps elevated from the hard palate and advanced medially. Simple, reliable, but does not lengthen the palate. Best for soft + hard palate clefts.
-
Veau-Wardill-Kilner (V-Y or "push-back") Repair - Retroposition of the mucoperiosteal flaps to lengthen the palate. Improves velopharyngeal function but leaves larger raw areas on the hard palate (risk of growth restriction).
-
Furlow Double-Opposing Z-Plasty - Particularly for soft palate / submucous cleft. Two opposing Z-plasties that simultaneously lengthen the palate and properly reorient the levator muscles. Excellent speech outcomes.
-
Intravelar veloplasty (IVVP) - Focused reconstruction of the levator muscle sling, can be combined with other techniques.
Alveolar Bone Grafting (ABG)
- Performed at 8-10 years (mixed dentition phase), ideally before eruption of the maxillary canine
- Uses autogenous cancellous bone (typically from iliac crest)
- Goals: close oronasal fistula, provide bone support for erupting permanent teeth, stabilize the maxillary arch
Secondary/Revision Surgery
- VPI / Pharyngoplasty: Posterior pharyngeal wall augmentation, pharyngeal flap, or sphincter pharyngoplasty for residual velopharyngeal incompetence
- Cleft lip/nose revision: For misaligned vermilion, lip asymmetry, poor alar base position, or deviated septum - minor adjustments possible before age 14-15; major nasal surgery (open septorhinoplasty) after skeletal maturity
- Orthognathic surgery: Le Fort I osteotomy for midface hypoplasia (a common late sequela), performed after skeletal maturity
Summary of Surgical Timeline
Birth → Diagnosis, MDT referral, feeding support, NAM/PSIO
~3 months → Cleft lip repair (Millard rotation-advancement)
9-12 months → Cleft palate repair (Von Langenbeck / Furlow / V-Y)
8-10 years → Alveolar bone grafting + orthodontics
4-6 years → Pharyngoplasty if VPI present (after speech assessment)
12-18 years → Definitive orthodontics, rhinoplasty, orthognathic surgery
Sources:
- Schwartz's Principles of Surgery, 11th Edition, Chapter 45 (Plastic and Reconstructive Surgery), pp. 2009-2013
- Bailey and Love's Short Practice of Surgery, 28th Edition, Chapter 50, pp. 762-769
This is a shared conversation. Sign in to Orris to start your own chat.