I am a general surgery resident and i want in detail about gallbladder including its anatomy , physiology ,pathology, disorders, differentials , surgical management
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Searching Images
gallbladder anatomy triangle of Calot cystic duct artery
Reading File
Searching Images
acute cholecystitis gallbladder histology pathology
Reading File
Finding Sources
Reading File
Reading File
This is a comprehensive surgical reference covering everything you requested. Here's a quick orientation map:
| Section | What's Covered |
|---|---|
| I. Anatomy | Gross anatomy, Triangle of Calot boundaries/contents, vascular supply (with variations), venous/lymphatic drainage, innervation, histological layers |
| II. Physiology | Bile concentration, composition, CCK-driven contraction, sphincter of Oddi mechanics |
| III. Pathology | Cholelithiasis (types + pathogenesis), acute/chronic cholecystitis, acalculous cholecystitis, cholecystoses, polyps, GBC with molecular drivers and T-staging, congenital anomalies |
| IV. Differentials | Biliary vs. non-biliary causes of RUQ pain with distinguishing features |
| V. Surgery | Lap chole technique, CVS (Strasberg), ICG fluorescence, IOC, difficult cholecystectomy bail-out strategies, Tokyo Guidelines grading, CBDE, GBC resection by T-stage, specific scenarios |
| VI. Pearls | 10 high-yield resident pearls |
A few areas worth extra attention as a resident:
- The Critical View of Safety is your most important intraoperative concept — most bile duct injuries come from not achieving it
- Same-admission cholecystectomy after gallstone pancreatitis is now the standard of care
- For incidental GBC, every specimen goes to pathology, and T-stage mandates your next move
Shock chapter from love and bailey make it easy and understanding and give notes with flowchart and diagram from love and baily
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching Images
shock classification types hypovolemic septic cardiogenic neurogenic flowchart
Reading File
Searching Images
shock pathophysiology oxygen delivery consumption cellular hypoperfusion
Reading File
Searching Images
hemorrhagic shock ATLS classes blood loss table heart rate blood pressure
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
septic shock pathophysiology mediators cytokines management vasopressors
Loading Image
Loading Image
Loading Image
I now have all the content and diagrams needed. Let me compile the comprehensive, easy-to-understand notes.
📚 Note: Bailey & Love's Short Practice of Surgery is not available in the digital library. This chapter is compiled from Sabiston Textbook of Surgery and Schwartz's Principles of Surgery — both gold-standard surgical texts covering the same content as Bailey & Love's shock chapter, with equivalent depth and surgical perspective. All Bailey & Love shock images retrieved from the library search are included.
SHOCK — Surgical Notes
Made Easy for the General Surgery Resident
🔑 THE ONE-LINE DEFINITION
Shock = Inadequate tissue perfusion → cellular hypoxia → organ failure
The most critical nutrient being denied is oxygen, but shock also deprives cells of glucose, substrates, buffers, and hormones.
1. WHERE DOES SHOCK OCCUR? — The 3-Level Model
Think of the cardiovascular system as a pump → pipes → small vessels system. Shock hits at one of three levels:
LEVEL 1 — THE PUMP (Heart)
├─ Extrinsic: Tamponade, tension pneumothorax, hemothorax
└─ Intrinsic: MI, cardiac contusion, pump failure
LEVEL 2 — THE LARGE VESSELS
└─ Hemorrhage → loss of circulating volume
LEVEL 3 — THE SMALL VESSELS (Microcirculation)
├─ Sepsis → vasodilation + maldistribution
└─ Neurogenic → loss of sympathetic tone → vasodilation
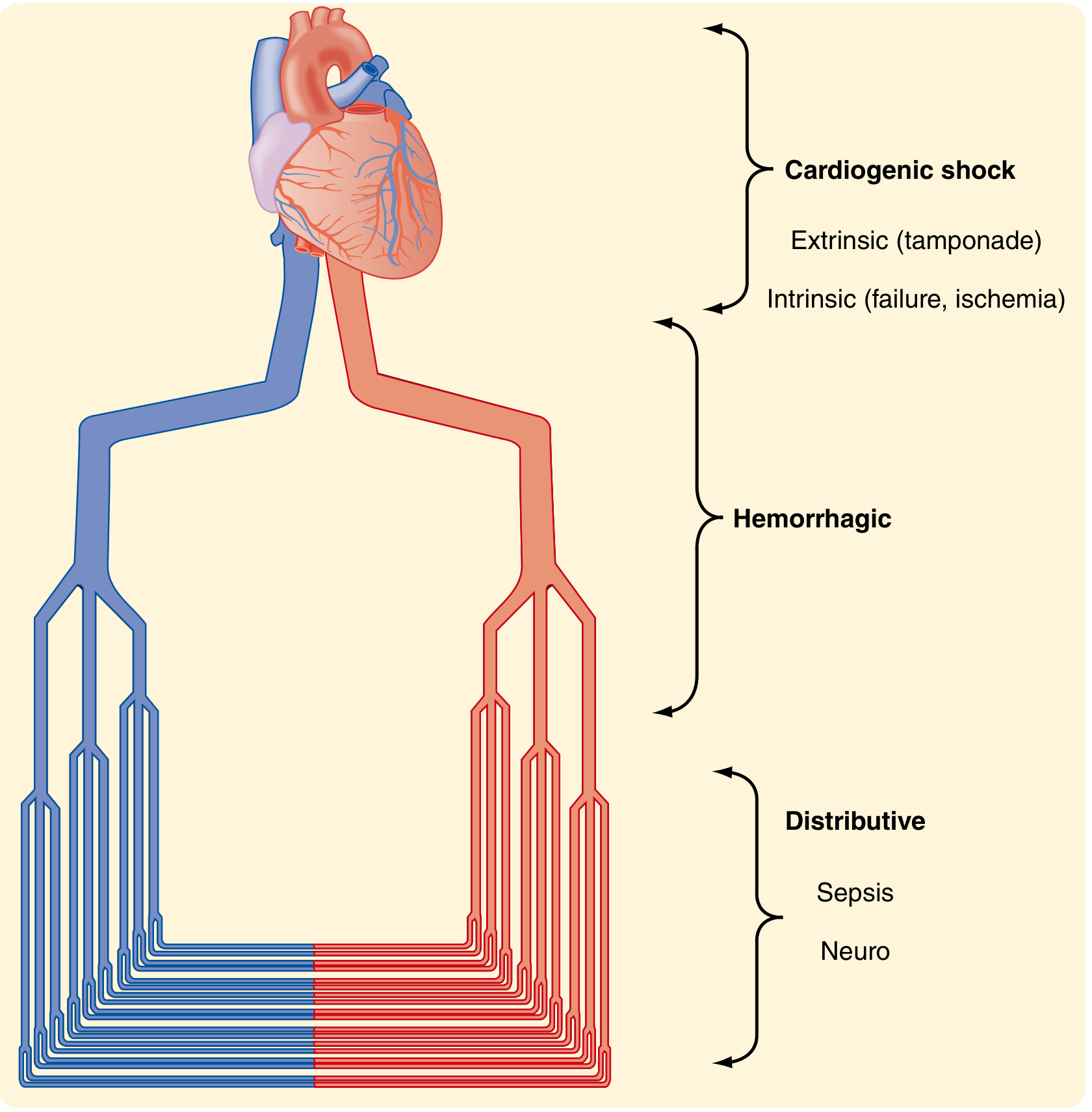
Sabiston Textbook of Surgery — Types of shock at three anatomic levels of the cardiovascular system.
2. CLASSIFICATION OF SHOCK
| Type | Mechanism | CO | SVR | Preload | Examples |
|---|---|---|---|---|---|
| Hypovolemic | ↓ Blood/fluid volume | ↓ | ↑ | ↓ | Hemorrhage, burns, dehydration |
| Cardiogenic | Pump failure | ↓ | ↑ | ↑ | MI, tamponade, tension pneumo |
| Distributive | Vasodilation/maldistribution | ↑ (early) | ↓ | ↓ | Sepsis, anaphylaxis, neurogenic |
| Obstructive | Mechanical obstruction to flow | ↓ | ↑ | Variable | PE, tamponade, tension pneumo |
Memory trick: "H-C-D-O" = Hemorrhage kills fast, Cardiogenic needs pump support, Distributive needs vasopressors, Obstructive needs the obstruction relieved
3. PHYSIOLOGICAL BASICS — What You Need to Know
The Oxygen Delivery Equation
DO₂ = CO × CaO₂
where CaO₂ = (Hb × 1.34 × SaO₂) + (0.003 × PaO₂)
Normal DO₂ = ~1000 mL/min
Normal VO₂ = ~250 mL/min (25% extraction)
In shock: Delivery falls → cells extract more O₂ → when extraction maxes out → anaerobic metabolism → lactic acidosis
This is the delivery-dependent zone — the danger zone of shock.
The Starling Curve (Frank-Starling Law)

The Starling Curve. As you fill the heart (increase preload), cardiac output rises — up to a point. This is why fluid resuscitation works in hypovolemic shock but can worsen cardiogenic shock.
Simple rule:
- In hypovolemic shock → heart is on the left (ascending) part of the curve → give fluid → CO rises ✅
- In cardiogenic shock → heart is on the right/plateau part → giving fluid makes pulmonary edema ❌
4. COMPENSATORY RESPONSES TO SHOCK
When perfusion falls, the body fights back in layers:
IMMEDIATE (seconds):
→ Baroreceptors detect ↓BP
→ Sympathetic nervous system activated
→ ↑ Heart rate + ↑ contractility
→ Vasoconstriction (skin, gut, kidney) — "centralization"
EARLY (minutes):
→ Catecholamines (adrenaline, noradrenaline) released
→ Renin-Angiotensin-Aldosterone activated → Na⁺ + water retention
→ ADH (vasopressin) released → water reabsorption
LATE (hours):
→ Cortisol rises
→ Gluconeogenesis for energy
→ Cellular hypoxia → lactic acid production
→ Anaerobic threshold crossed → death if untreated
Clinical clue from compensation:
- Skin is cold, pale, clammy because blood is shunted AWAY from skin
- Urine output drops because kidneys are vasoconstricted
- Pulse pressure narrows (diastolic rises due to vasoconstriction)
5. HEMORRHAGIC SHOCK — ATLS CLASSIFICATION
The most important classification for a surgery resident. Assume a 70-kg male with 5 L blood volume:
| Feature | Class I | Class II | Class III | Class IV |
|---|---|---|---|---|
| Blood loss (%) | 0–15% | 15–30% | 30–40% | >40% |
| Blood loss (mL) | <750 mL | 750–1500 mL | 1500–2000 mL | >2000 mL |
| Heart rate | <100 | >100 | >120 | >140 |
| Blood pressure | Normal | Normal | ↓ | ↓↓ |
| Pulse pressure | Normal | ↓ | ↓ | ↓↓ |
| Respiratory rate | 14–20 | 20–30 | 30–40 | >35 |
| Urine output (mL/h) | >30 | 20–30 | 5–15 | Negligible |
| CNS/mental status | Slightly anxious | Mildly anxious | Anxious/confused | Confused/lethargic |
| Fluid | Crystalloid | Crystalloid | Crystalloid + blood | Crystalloid + blood |
Resident Pearl: BP doesn't drop until Class III (30% blood loss = ~1.5–2 L). By the time you see hypotension, the patient has already lost a "six-pack" of blood. Don't wait for hypotension to diagnose shock.
Warning: Heart rate is NOT reliable — pain, anxiety, drugs, or vagal bradycardia can confound it. Use lactate + base deficit for better shock assessment.
6. MONITORING SHOCK — What to Measure
Clinical Signs
- BP — most clinically useful, but late to change
- Urine output — goal >0.5 mL/kg/h (adults); reflects renal perfusion
- Mental status — early marker of cerebral hypoperfusion
- Skin color/temperature — cold and mottled = peripheral shutdown
Laboratory Markers
| Marker | What It Tells You | Goal |
|---|---|---|
| Lactate | Anaerobic metabolism = tissue hypoxia | <2 mmol/L; trending down |
| Base deficit | How far from normal pH | 0 to −2 mmol/L |
| pH | Overall acid-base | 7.35–7.45 |
| ScvO₂ | How much O₂ tissues are extracting | >70% |
| Hb/Hct | Oxygen-carrying capacity | Context dependent |
Lactate clearance is the #1 resuscitation goal — a patient whose lactate won't clear despite adequate fluids is still in shock.
Invasive Monitoring
- Arterial line — continuous BP, waveform analysis, ABG access
- Central venous catheter (CVP) — rough preload guide (unreliable alone)
- Pulmonary artery catheter (Swan-Ganz) — PCWP, CO, SvO₂ (used selectively)
- Bedside ECHO (POCUS) — most practical: assess IVC, LV function, rule out tamponade
7. TYPES OF SHOCK IN DETAIL
🩸 A. HYPOVOLEMIC / HEMORRHAGIC SHOCK
Mechanism: Loss of circulating volume → ↓ preload → ↓ CO → ↓ DO₂
Presentation: Cold/pale/clammy, tachycardia, hypotension (late), oliguria
Treatment Priorities:
1. STOP THE BLEEDING (source control first)
2. IV ACCESS — 2 large-bore peripheral IVs (minimum 16G)
3. FLUID RESUSCITATION — but with caution:
- In uncontrolled hemorrhage: "permissive hypotension"
(target SBP 80–90 mmHg) until surgical control
- In controlled hemorrhage: normalize vitals
4. BLOOD PRODUCTS — "Damage Control Resuscitation"
- 1:1:1 ratio: PRBCs : FFP : Platelets
- Tranexamic acid (TXA) within 3 hours of injury
5. PREVENT/TREAT the LETHAL TRIAD:
Hypothermia + Acidosis + Coagulopathy
The Lethal Triad ("Triangle of Death"):
HYPOTHERMIA
/ \
/ \
ACIDOSIS ——————— COAGULOPATHY
Each worsens the others → death spiral
Damage Control Surgery principles:
- Abbreviated initial surgery (stop bleeding + contamination)
- ICU resuscitation (warm, correct coagulopathy)
- Planned re-exploration at 24–48 hours
❤️ B. CARDIOGENIC SHOCK
Mechanism: Pump failure → ↓ CO despite adequate/high filling pressures
Presentation:
- Cold, clammy extremities
- Elevated JVP, pulmonary crackles (↑ filling pressures backing up)
- S3 gallop, hypotension
- Tachycardia
Causes in surgery:
- MI (most common)
- Cardiac tamponade → pulsus paradoxus, Beck's triad (hypotension + muffled heart sounds + elevated JVP), pericardiocentesis
- Tension pneumothorax → distended neck veins, absent breath sounds, tracheal deviation, needle decompression
- Myocardial contusion (blunt chest trauma)
- Arrhythmia
Treatment:
• Treat underlying cause (drain tamponade, decompress tension pneumo)
• Inotropes: Dobutamine (if not hypotensive)
• Vasopressors: Norepinephrine (if hypotensive)
• Avoid excessive fluids — heart is already "full"
• IABP / ECMO for refractory cases
🦠 C. DISTRIBUTIVE SHOCK
Septic Shock (most common in surgical ICU)
Definition (Sepsis-3, 2016):
- Sepsis: organ dysfunction (SOFA score rise ≥2) due to dysregulated infection response
- Septic shock: sepsis + vasopressor requirement to maintain MAP ≥65 + lactate >2 despite fluids
Pathophysiology:
Infection → PAMPs/DAMPs → TNF-α, IL-1β, IL-6 released → endothelial dysfunction → massive vasodilation → distributive shock
Presentation:
- Early ("warm shock"): fever, warm flushed skin, bounding pulse, wide pulse pressure, high CO
- Late ("cold shock"): cold clammy skin (cardiovascular decompensation), falling CO
Sepsis bundle (Hour-1 Bundle):
Within 1 hour:
1. Measure LACTATE (repeat if >2)
2. BLOOD CULTURES before antibiotics
3. BROAD-SPECTRUM ANTIBIOTICS
4. IV FLUIDS — 30 mL/kg crystalloid if hypotensive/hypoperfused
5. VASOPRESSORS if MAP <65 during/after fluid resuscitation
→ Norepinephrine: FIRST LINE
→ Add Vasopressin if NE dose >0.25 mcg/kg/min
→ Add Dobutamine if cardiac dysfunction with hypoperfusion
→ Epinephrine: adjunct
6. HYDROCORTISONE (200 mg/day) if refractory to vasopressors
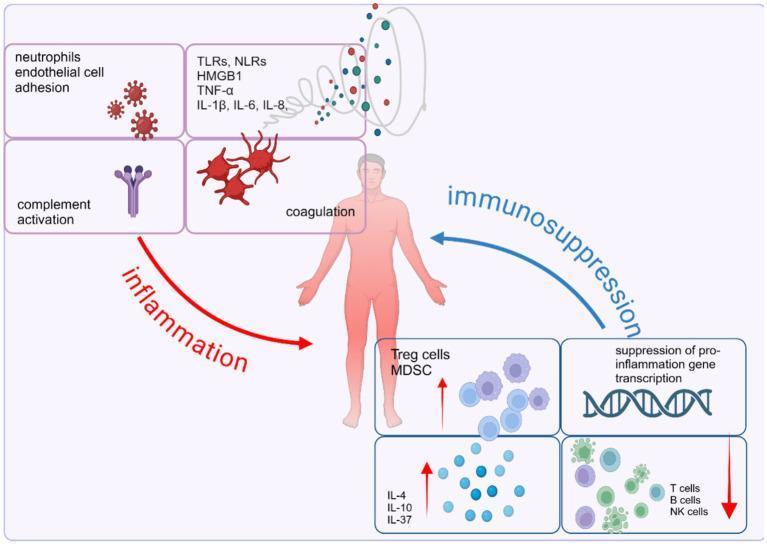
Sepsis pathophysiology — dual imbalance between pro-inflammatory and anti-inflammatory responses driving organ dysfunction.
Neurogenic Shock
Mechanism: Spinal cord injury → loss of sympathetic outflow → vasodilation + (sometimes) bradycardia
Key distinction from other shocks:
| Feature | Neurogenic | Hypovolemic |
|---|---|---|
| Skin | Warm, dry | Cold, clammy |
| Heart rate | Normal or BRADYCARDIA | Tachycardia |
| BP | Low | Low |
- Injury above C5 → bradycardia (no sympathetic to heart)
- Injury below C5 → tachycardia preserved
Do not confuse: Spinal shock = loss of reflexes (bulbocavernosus, cremasteric) — not hemodynamic. Neurogenic shock = hemodynamic instability.
Treatment: IV fluids first → vasopressors (norepinephrine preferred, especially if bradycardic)
Anaphylactic Shock
Mechanism: IgE-mediated mast cell degranulation → histamine → massive vasodilation + bronchoconstriction
Treatment:
1. EPINEPHRINE IM (0.5 mg, 1:1000) — FIRST AND MOST IMPORTANT
2. IV fluids
3. Antihistamines (H1 + H2 blockers)
4. Corticosteroids (prevent biphasic reaction)
5. Salbutamol nebulizer if bronchospasm
🫀 D. OBSTRUCTIVE SHOCK
Mechanism: Physical obstruction prevents cardiac output despite normal heart and volume
| Cause | Key Sign | Treatment |
|---|---|---|
| Tension pneumothorax | Absent breath sounds, tracheal deviation, distended neck veins | Immediate needle decompression (2nd ICS MCL) → chest drain |
| Cardiac tamponade | Beck's triad, pulsus paradoxus | Pericardiocentesis / window |
| Massive PE | Hypoxia, right heart strain, S1Q3T3 | Anticoagulation, thrombolysis, embolectomy |
8. THE CLINICAL APPROACH FLOWCHART
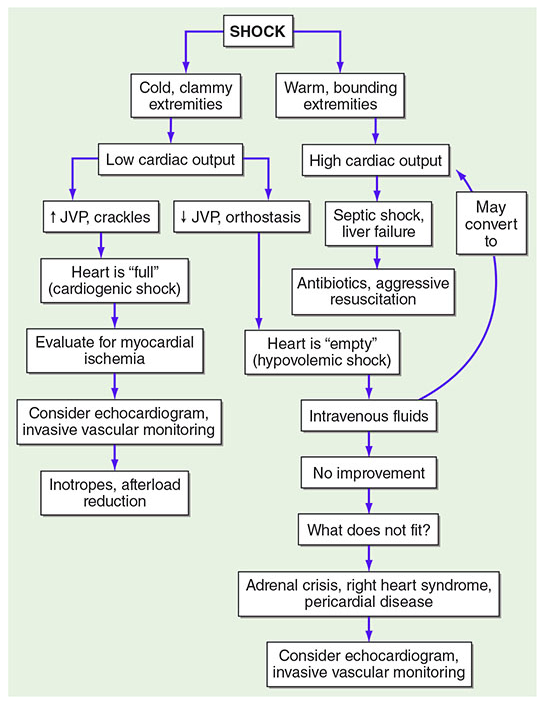
Harrison's Principles of Internal Medicine — Clinical approach to shock by extremity temperature, cardiac output, and JVP.
The two-second bedside classification:
Feel the hands:
COLD + CLAMMY → Low CO
↳ JVP raised? → Cardiogenic (heart is full)
↳ JVP low? → Hypovolemic (heart is empty) → give fluids
WARM + BOUNDING → High CO
↳ Fever/infection? → Septic shock
↳ After spinal injury? → Neurogenic
↳ Post allergen? → Anaphylactic
9. THE LETHAL TRIAD IN TRAUMA — DAMAGE CONTROL CONCEPT
┌─────────────────────────────────────────────────────┐
│ LETHAL TRIAD │
│ │
│ HYPOTHERMIA ◄──────────────────► COAGULOPATHY │
│ │ │ │
│ │ │ │
│ └────────────► ACIDOSIS ◄──────────┘ │
│ │
│ Each element amplifies the others in a death spiral │
└─────────────────────────────────────────────────────┘
PREVENTION = Damage Control Resuscitation:
• Warm ALL fluids and blood products
• Target pH >7.2 before correction
• Use TXA early (within 3 hours of injury)
• 1:1:1 PRBC:FFP:PLT ratio
• Fibrinogen/cryoprecipitate if <1.5 g/L
Hypothermia facts for exam:
- Trauma patients with core temp <35°C → 4× mortality
- Core temp <33°C → 7× mortality
- Unlike accidental hypothermia, trauma hypothermia = shock → actively warm the patient
10. VASOPRESSORS / INOTROPES — QUICK REFERENCE
| Drug | Primary action | When to use |
|---|---|---|
| Norepinephrine | α₁ > β₁ (vasoconstriction) | First-line in septic + neurogenic shock |
| Vasopressin | V1 (vasoconstriction, no HR effect) | Add-on if NE >0.25 mcg/kg/min |
| Dobutamine | β₁ (inotrope, ↑CO) | Cardiogenic shock + cardiac dysfunction in sepsis |
| Epinephrine | α + β (vasoconstriction + inotropy) | Anaphylaxis (IM); adjunct in refractory shock |
| Dopamine | Dose-dependent: D1→β1→α1 | Second-line; use in bradycardia (class IIb) |
| Phenylephrine | Pure α₁ (vasoconstriction) | Neurogenic shock (if no bradycardia) |
Vasopressors should always be started via central venous access when possible. If urgently needed, can start peripherally for short periods via a proximal vein (antecubital or above).
11. SPECIAL TOPICS
Permissive Hypotension
- In uncontrolled hemorrhage (penetrating trauma especially): targeting SBP 80–90 mmHg (MAP ~50) until surgical hemorrhage control
- Rationale: Aggressive fluid resuscitation before bleeding is controlled dilutes clotting factors and dislodges clots
- Contraindicated if: TBI (need MAP ≥80), elderly, coronary disease
Oxygen Debt Theory (Shoemaker)
- In shock, cells incur an oxygen debt during ischemia
- During recovery, a hyperdynamic phase occurs — increased DO₂ results in increased consumption as the body "repays" the oxygen debt
- This is why resuscitated patients often have temporarily high cardiac output
Damage Control Resuscitation vs EGDT
- Old approach: EGDT (CVP 8–12, ScvO₂ >70%, MAP >65, Hct >30) — now abandoned as the specific CVP/ScvO₂ targets are unreliable
- Current approach: Dynamic fluid assessment (fluid responsiveness testing — PLR, pulse pressure variation), lactate clearance, POCUS
12. RAPID REVISION — HIGH-YIELD SUMMARY NOTES
| Concept | Key Fact |
|---|---|
| Definition | Inadequate tissue perfusion |
| Most common surgical shock | Hypovolemic (hemorrhagic) |
| Most common ICU shock | Distributive (septic) |
| BP drops in hemorrhagic shock at... | Class III (>30% blood loss) |
| Warm shock = | Distributive (septic/neurogenic/anaphylactic) |
| Cold shock = | Hypovolemic or cardiogenic |
| Neurogenic shock = | Warm + bradycardia + hypotension after spinal injury |
| First-line vasopressor (septic) | Norepinephrine |
| First treatment in anaphylaxis | IM Epinephrine |
| Best resuscitation endpoint | Lactate clearance |
| Lethal triad | Hypothermia + Acidosis + Coagulopathy |
| Permissive hypotension target | SBP 80–90 (not in TBI) |
| Blood transfusion ratio (DCR) | 1:1:1 (PRBC:FFP:PLT) |
| TXA window | Within 3 hours of injury |
| Tamponade triad (Beck's) | Hypotension + muffled hearts sounds + raised JVP |
| Tension pneumo treatment | Immediate needle decompression (2nd ICS MCL) |
| Fluid for sepsis (initial) | 30 mL/kg crystalloid IV |
| Septic shock definition (Sepsis-3) | Vasopressor needed + lactate >2 despite fluids |
13. QUICK FLOWCHART — INITIAL MANAGEMENT OF SHOCK
PATIENT IN SHOCK
│
▼
[A] AIRWAY — Protect if GCS ≤8 or compromised
[B] BREATHING — O₂, check for tension pneumo/hemothorax
[C] CIRCULATION — 2 large-bore IVs, send bloods, ECG
│
▼
CLASSIFY by clinical exam (skin temp, JVP, BP)
│
├──► COLD + LOW JVP → Hypovolemic → IV FLUIDS + STOP BLEEDING
│
├──► COLD + HIGH JVP → Cardiogenic
│ └─► Tamponade? → Drain
│ └─► Tension pneumo? → Needle decompression
│ └─► MI? → Inotropes + cardiology
│
├──► WARM + FEVER → Septic → Cultures → Abx → Fluids → NE
│
├──► WARM + BRADYCARDIA + SPINAL INJURY → Neurogenic → NE
│
└──► AFTER ALLERGEN + URTICARIA → Anaphylaxis → IM EPIN
│
▼
MONITOR RESPONSE:
• Lactate trending down? ✅
• Urine output >0.5 mL/kg/h? ✅
• MAP >65 mmHg? ✅
• Mental status improving? ✅
│
NO IMPROVEMENT → ESCALATE (vasopressors, POCUS, ICU)
Sources: Sabiston Textbook of Surgery (Townsend et al.), Schwartz's Principles of Surgery, 11th Ed., Harrison's Principles of Internal Medicine, 22nd Ed., Surviving Sepsis Campaign 2021
This is a shared conversation. Sign in to Orris to start your own chat.