Safe surgical dislocation of ganz with trochanteric flip osteotomy
Reading File
Finding Sources
Finding Sources
Searching PubMed
safe surgical dislocation hip Ganz trochanteric osteotomy
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive, detailed content from both Campbell's (15th Ed, 2026) and Rockwood & Green's (10th Ed, 2025). Let me compile the full response.
Safe Surgical Dislocation of the Hip (Ganz Technique) with Trochanteric Flip Osteotomy
Concept and Rationale
Surgical dislocation of the hip (Ganz technique) provides full 360-degree access to the acetabular rim, labrum, and femoral head-neck junction while preserving femoral head vascularity. The key anatomical principle is protecting the deep branch of the medial femoral circumflex artery (MFCA) as it supplies the posterolateral retinacular vessels to the femoral head.
The trochanteric flip osteotomy is the cornerstone of this approach - it is a digastric (or trigastric) osteotomy because both the abductor muscles (gluteus medius and minimus) and the vastus lateralis remain attached to the osteotomized trochanteric fragment. This continuity of the soft tissue sleeve preserves the fragment's viability and allows anterior retraction to expose the capsule.
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 435
- Rockwood and Green's Fractures in Adults 10th Ed 2025, p. 2507
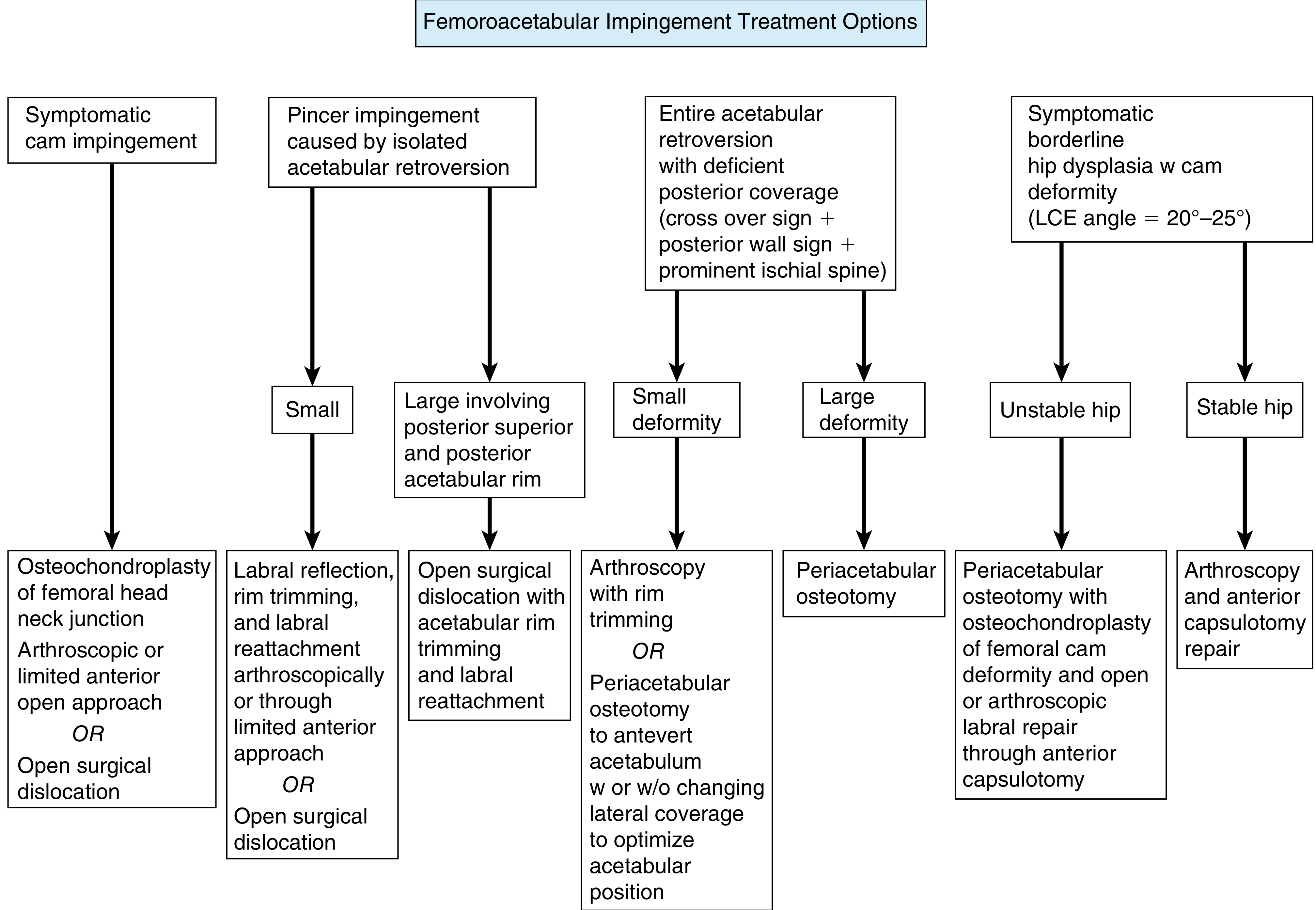
Indications
- Femoroacetabular impingement (FAI) - cam, pincer, or combined (especially large deformities)
- Femoral head fractures (Pipkin types I-IV)
- Acetabular fractures requiring intra-articular visualization
- Slipped capital femoral epiphysis (SCFE)
- Residual Perthes disease deformities
- Loose body removal requiring full joint access
FAI Treatment Algorithm:
Preoperative Planning
| Item | Detail |
|---|---|
| Table | Radiolucent or standard - lateral position |
| Positioning aids | Bean bag or hip positioner, axillary roll, padded mayo stand, large rectangular bump |
| Protect | Down-side peroneal nerve with gel padding |
| Fluoroscopy | From anterior side of patient |
| Implants | Small-fragment kit, mini-fragment kit, long 3.5/4.5 mm screws (50-80 mm), suture anchors |
| Assistants | Minimum 2 surgical assistants required |
- Rockwood and Green's, p. 2615
Positioning
The patient is placed in the lateral decubitus position (as for a posterior/Kocher-Langenbeck approach). An axillary roll is placed and the ipsilateral arm is supported on a padded mayo stand. A padded mayo stand is set up posteriorly to hold the operative leg in slight internal rotation during osteotomy. The leg is bumped to neutral or slight abduction to relax the TFL.
Surgical Technique (Ganz et al.) - Step by Step
1. Approach
Make a Kocher-Langenbeck incision (or Gibson approach) with the patient in lateral decubitus. Split the fascia lata. For the Gibson modification, develop the interval between the TFL and gluteus maximus (rather than splitting gluteus maximus) - this protects the neurovascular supply to the anterior gluteus maximus and extends anterosuperior visualization.
2. Identify Posterior Border of Gluteus Medius
Internally rotate the leg and identify the posterior border of the gluteus medius. Do not mobilize the gluteus medius or attempt to expose the piriformis tendon - this is the most critical step for vascular protection.
3. Trochanteric Flip Osteotomy
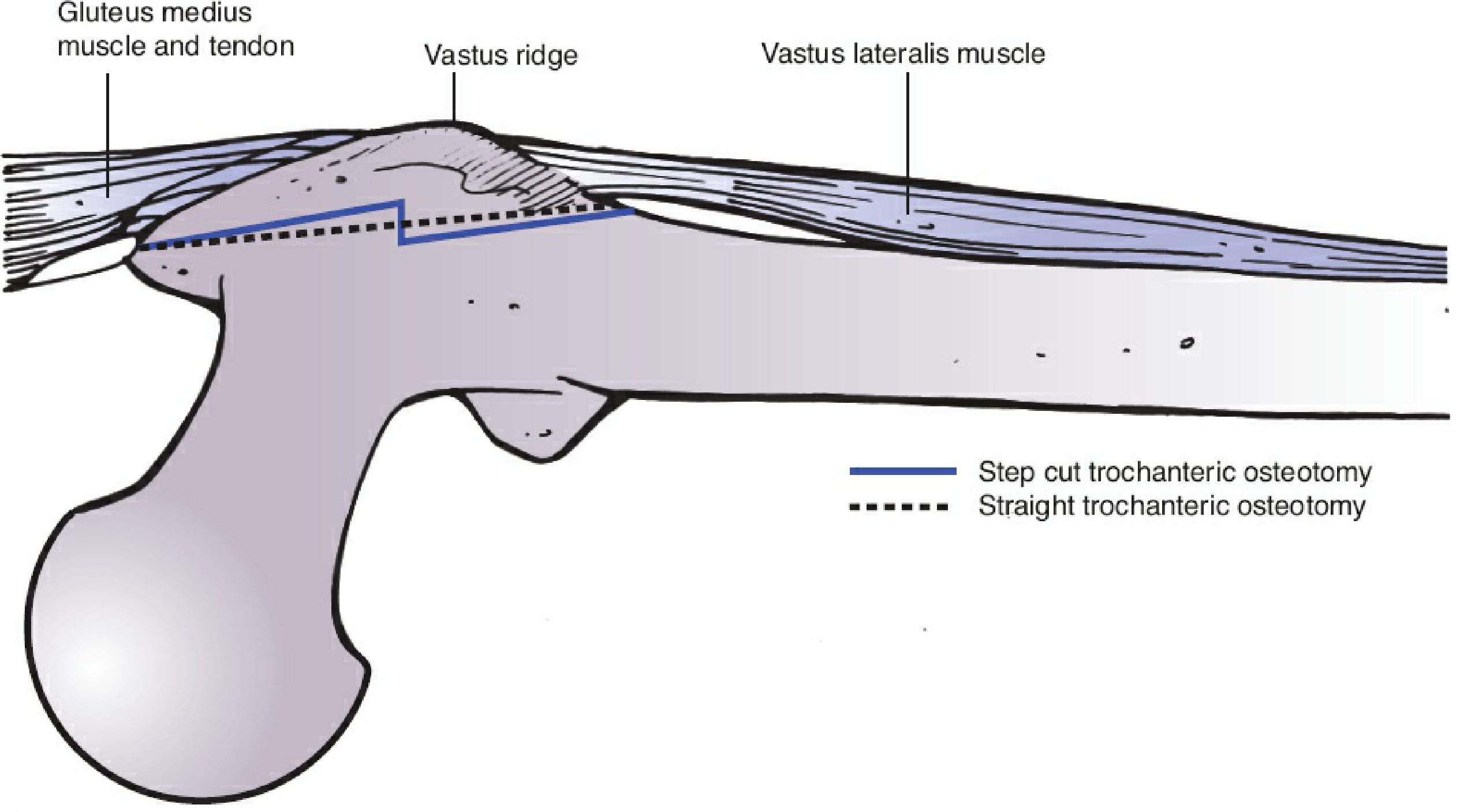
- Mark the osteotomy line from the posterosuperior edge of the greater trochanter extending distally to the posterior border of the vastus ridge
- Use an oscillating saw - maximum thickness 1.5 cm
- The proximal limit exits just anterior to the most posterior insertion of the gluteus medius (this protects the profundus branch of the MFCA)
- The osteotomy starts within the tendon of the gluteus medius in the middle of the tip of the trochanter and ends just distal to the vastus ridge
- Can be performed as a straight osteotomy or a step-cut osteotomy (step-cut improves rotational stability at repair)
- The piriformis tendon insertion remains on the intact proximal femur - this is the critical landmark protecting the MFCA
Why this is "safe": The piriformis marks the entry point of the deep branch of the MFCA into the femoral head. Keeping piriformis on the femur (not on the trochanteric fragment) ensures the arterial supply is never disrupted during fragment retraction.
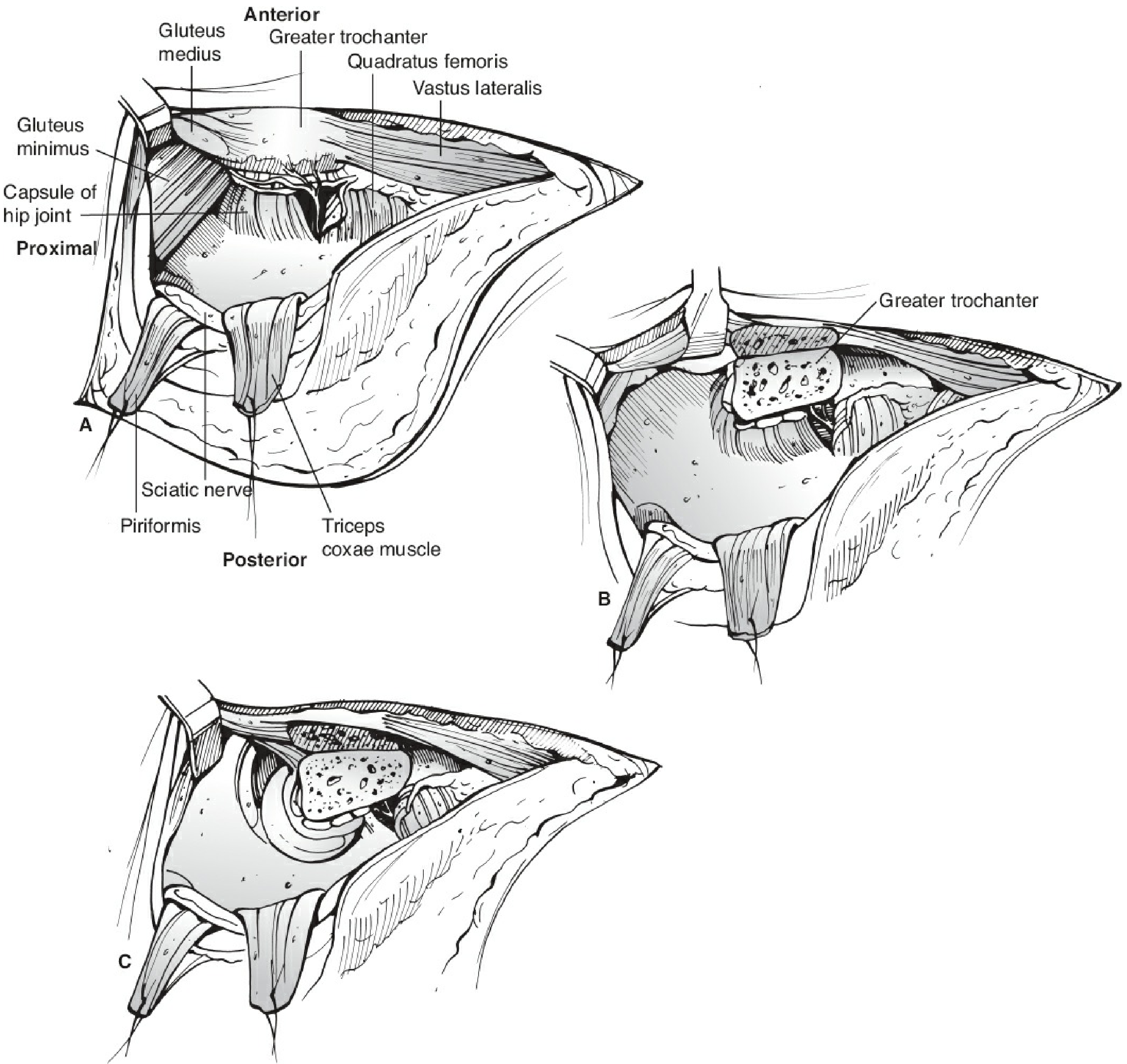
4. Mobilize the Trochanteric Fragment
Release the greater trochanteric fragment along its posterior border to approximately the middle of the gluteus maximus tendon. Retract it anteriorly with its attached gluteus medius, minimus, and vastus lateralis (the digastric/trigastric relationship). Elevate the gluteus minimus and medius off the capsule proximally. As the hip is abducted, flexed, and externally rotated, the vastus lateralis and intermedius are elevated anteriorly off the capsule and femur.
5. Capsulotomy
A Z-shaped capsulotomy is performed:
- Along the superoanterior femoral neck
- At the anterior acetabular rim - curve posteriorly following the acetabular rim
- The anterior limb goes inferiorly along the intertrochanteric ridge - leave a cuff of tissue along the ridge to allow reattachment at closure
6. Hip Dislocation
- Place a bone hook around the femoral neck
- Assistant flexes and externally rotates the femur
- The bone hook is used to subluxate then dislocate the hip anteriorly
- If the ligamentum teres is intact, it must be transected to allow full dislocation
- The leg is externally rotated and the foot is placed in a sterile bag anteriorly
- A sterile padded mayo stand on the posterior side helps support the leg
7. Intra-articular Work
With the hip fully dislocated:
- Full 360-degree access to femoral head, acetabular rim, labrum, and cartilage
- Perform osteochondroplasty, fracture fixation, labral repair, loose body removal as indicated
- Inferior Pipkin fragments often have the ligament of Weitbrecht (from the MFCA) attached - preserve it to maintain blood supply to the fragment
- Use suture anchors for labral reattachment to the acetabular rim
8. Reduction and Capsular Repair
Reduce the hip. Recheck the superior and posterior labrum. Perform a loose capsular repair to prevent increased intracapsular pressure from hematoma that could occlude the femoral head blood supply.
9. Trochanteric Reattachment
- Replace the trochanteric fragment into its osteotomy bed
- Fix with 3.5 mm or 4.5 mm lag screws (50-80 mm length) aimed toward the lesser trochanter
- Fluoroscopy to confirm reduction, implant positioning, and joint congruency
Postoperative Protocol
- 6 weeks of foot-flat partial weight bearing for trochanteric osteotomy healing
- Protected weight bearing protects the fixation until bony union
- DVT prophylaxis
- Physiotherapy for abductor strengthening once union confirmed
Outcomes
In follow-up studies ranging from 2-10 years (Campbell's, p. 435):
- Good to excellent results: 68% to 94%
- Conversion to THA: 0%-30%
- Negative predictors: preoperative Tonnis grade 2 arthritis, intraoperative cartilage delamination, increasing age
- Labral refixation improves results at 10 years vs. debridement
- 10-year survivorship without arthritic progression: 80% in FAI with labral reattachment
- Heterotopic ossification and painful trochanteric implants requiring removal are rarely reported
Key Safety Points Summary
| Risk | Protective Step |
|---|---|
| Avascular necrosis of femoral head | Do NOT expose piriformis tendon; keep its insertion on proximal femur |
| Vascular injury to MFCA | Osteotomy exits anterior to posterior insertion of gluteus medius |
| Trochanteric nonunion | Lag screw fixation toward lesser trochanter; 6 weeks protected WB |
| Abductor weakness | Digastric continuity of gluteus medius/minimus and vastus lateralis on fragment |
| Sciatic nerve injury | Keep knee flexed during exposure to relieve sciatic tension |
| Intracapsular hematoma / AVN | Loose (not tight) capsular repair at closure |
Recent Evidence
A 2025 systematic review (PMID 41262480) evaluated outcomes of surgical hip dislocation for femoral head trauma, and a 2024 review of posterior acetabular approaches (PMID 39325162) discusses the trochanteric flip osteotomy in context of the Kocher-Langenbeck approach - both supporting the safety profile of this technique when performed with strict attention to the piriformis and MFCA.
Sources:
- Campbell's Operative Orthopaedics 15th Ed 2026 - Technique 7.1 (Ganz et al.), pp. 435-436
- Rockwood and Green's Fractures in Adults 10th Ed 2025 - pp. 2507-2508, 2615-2617
- Siebenrock KA et al. Trochanteric flip osteotomy. J Orthop Trauma. 1998;12(6):387-391 (original description)
This is a shared conversation. Sign in to Orris to start your own chat.