Treatment for mtp
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"medical termination of pregnancy" AND "mifepristone" AND "misoprostol"
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive information. Here is a full, well-structured answer:
Treatment for Medical Termination of Pregnancy (MTP)
MTP methods are selected based on gestational age, patient factors, and available resources. There are two main categories: medical and surgical.
1. Medical Methods
A. Mifepristone + Misoprostol (First-line, up to 10 weeks / 70 days)
This is the standard evidence-based regimen with 96-99% efficacy:
| Step | Drug | Dose & Route | Timing |
|---|---|---|---|
| Day 1 | Mifepristone | 200 mg orally | Day 1 |
| 24-48 hrs later | Misoprostol | 800 mcg buccally or vaginally | 24-72 hrs after mifepristone |
- Mifepristone acts as a progesterone receptor antagonist, sensitizing the myometrium
- Misoprostol (a prostaglandin E1 analogue) causes uterine contractions and cervical ripening
- In India, the commercial MTP Kit contains: mifepristone 200 mg (1 tablet) + misoprostol 200 mcg x 4 tablets (800 mcg total)
An older alternative regimen: mifepristone 600 mg on day 1, followed by misoprostol 400 mcg orally on day 3.
Follow-up: Return at ~14 days to confirm complete termination by clinical exam or ultrasound.
B. Methotrexate + Misoprostol (when mifepristone unavailable)
- Methotrexate (antifolate) given first, followed by misoprostol - effective but takes longer than mifepristone regimen
- Less commonly used today
C. Misoprostol Alone
- Used when mifepristone is unavailable
- Vaginal misoprostol 800 mcg, repeated in 24 hours if expulsion has not occurred
- Complete abortion in ~91% of pregnancies up to 56 days
- Less effective than the combination regimen
2. Surgical Methods
First Trimester (up to 12-13 weeks)
| Method | Details |
|---|---|
| Manual Vacuum Aspiration (MVA) | Handheld plastic syringe + cannula; no electric pump needed; safe and effective up to ~10 weeks; can be done in outpatient/clinic settings |
| Electric Vacuum Aspiration (EVA) | Electric suction pump; standard for first-trimester termination |
| Dilation & Curettage (D&C) | Older method; largely replaced by vacuum aspiration |
- Cervical preparation: osmotic dilators or misoprostol 400 mcg vaginally/buccally 3-4 hours before procedure
- Prophylactic antibiotics: a single dose of doxycycline pre-operatively to reduce infection risk (Society of Family Planning recommendation)
- Complication rate is very low: major complications requiring hospitalization occur in <1% of cases
Second Trimester (13-24 weeks)
| Method | Details |
|---|---|
| Dilation & Evacuation (D&E) | Cervical preparation with osmotic dilators and/or mifepristone/prostaglandins, followed by surgical evacuation using suction + grasping forceps; fewer complications than medication abortion at this stage |
| Medical induction | Prostaglandins (misoprostol, PGE2) or oxytocin to stimulate labor and expulsion; used especially 13-20 weeks |
Beyond 24 weeks
For pregnancies with lethal fetal anomalies or serious maternal medical indications beyond 24 weeks, induction of labor and vaginal delivery (induction termination) is recommended.
3. MTP Act (India) - Legal Framework
Under the MTP Act 1971 (amended 2021):
- Up to 20 weeks: with consent of one registered medical practitioner
- 20-24 weeks: requires opinion of two registered medical practitioners (for specific categories - rape survivors, fetal abnormalities, etc.)
- Beyond 24 weeks: only for substantial fetal abnormalities, decided by a Medical Board
Contraindications to Medical Abortion (Mifepristone/Misoprostol)
- Confirmed/suspected ectopic pregnancy or undiagnosed adnexal mass
- IUD in place (must be removed first)
- Chronic adrenal failure
- Hemorrhagic disorder or concurrent anticoagulant therapy
- Inherited porphyria
- Allergy/hypersensitivity to mifepristone, misoprostol, or other prostaglandins
- Long-term corticosteroid therapy
- No access to emergency medical facilities (for backup surgical management)
Complications to Watch For
| Timing | Complication | Management |
|---|---|---|
| Immediate (<24h) | Bleeding, pain, uterine perforation, cervical laceration | Repair, surgical intervention |
| Delayed (24h - 4 weeks) | Retained products, endometritis | D&C or misoprostol; antibiotics |
| Late (>4 weeks) | Amenorrhea, Rh isoimmunization | Rh0(D) immunoglobulin 300 mcg IM for Rh-negative women |
| Medical abortion-specific | Heavy/prolonged bleeding (up to 8% of women); incomplete abortion (0.5%) | Surgical curettage if needed |
Rh-negative women require Rh0(D) immunoglobulin 300 mcg IM within 72 hours after any termination procedure.
Sources: Berek & Novak's Gynecology, p. 779-782 | Tintinalli's Emergency Medicine, p. 3394 | Park's Textbook of Preventive & Social Medicine, p. 592 | Goodman & Gilman's Pharmacological Basis of Therapeutics
Difference between gout and psedogout
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive data from multiple authoritative sources. Here is a complete comparison:
Gout vs. Pseudogout
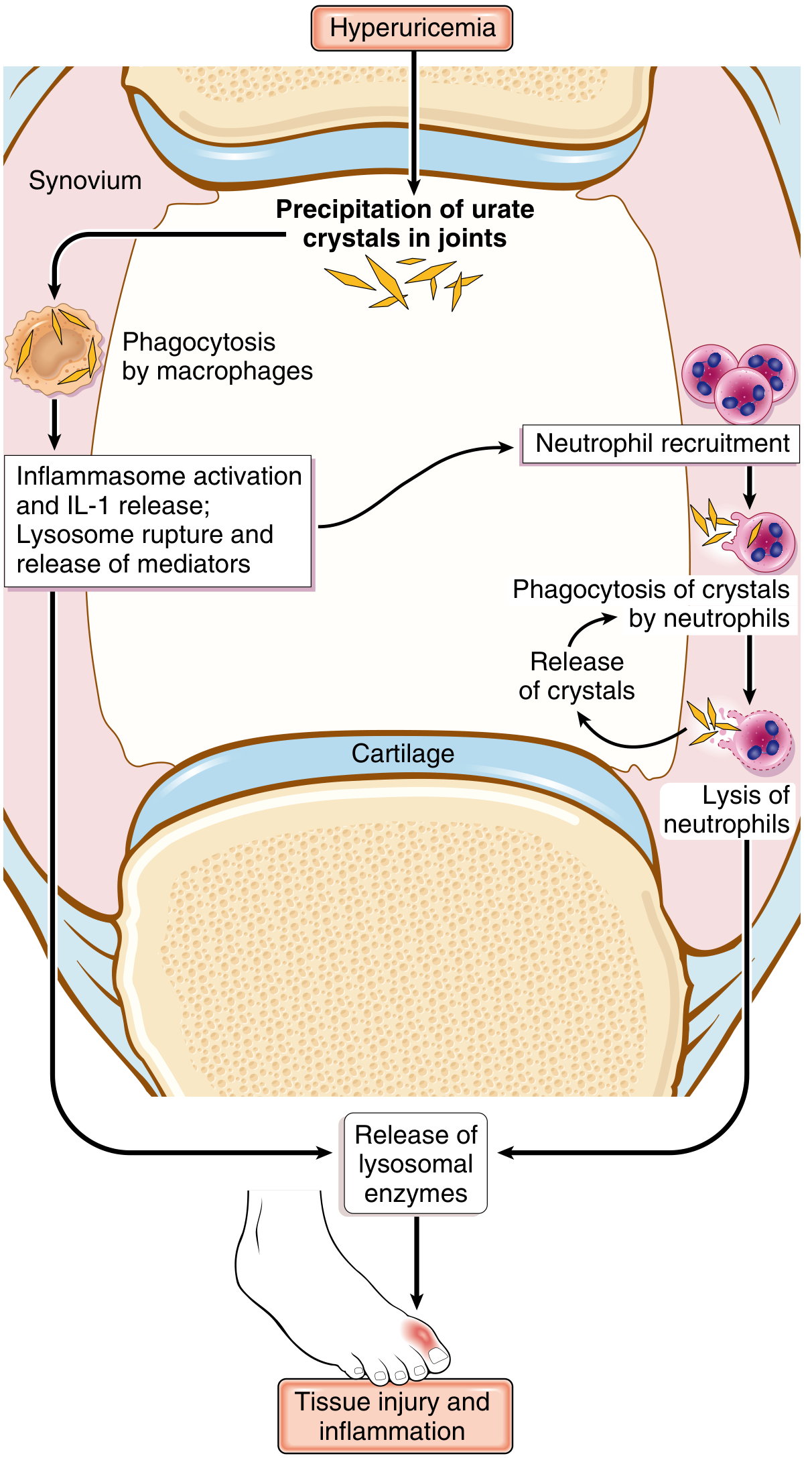
Both are crystal-induced arthropathies that trigger acute inflammatory synovitis via the same inflammasome/IL-1 pathway - but they differ in crystal type, joints affected, associated conditions, and microscopic appearance.
Side-by-Side Comparison
| Feature | Gout | Pseudogout (CPPD) |
|---|---|---|
| Crystal type | Monosodium urate (MSU) monohydrate | Calcium pyrophosphate dihydrate (CPPD) |
| Crystal origin | Purine metabolism (uric acid) | Articular cartilage degeneration; pyrophosphate transporter mutation (ANKH gene) |
| Underlying cause | Hyperuricemia (>6.8 mg/dL) - reduced excretion (90%) or overproduction | Idiopathic, hereditary, or secondary to metabolic disease |
| Associated conditions | Obesity, alcohol, high-purine diet, renal disease, thiazide diuretics, Lesch-Nyhan syndrome, leukemia | Hyperparathyroidism, hemochromatosis, hypomagnesemia, hypothyroidism, ochronosis, diabetes, previous joint damage |
| Age/Sex | Men >40 years (most common inflammatory joint disease in men >40); less common in women during reproductive years | >50 years; becomes more common with age - up to 60% of those age 85+ are affected; equal sex distribution |
| Classic joint | 1st metatarsophalangeal joint (podagra) - 50% of first attacks | Knees (most common), then wrists, elbows, shoulders, ankles |
| Attack duration | Hours to weeks; typically resolves completely | Can last weeks to months (longer than gout) |
| Attack pattern | Sudden, excruciating pain; monoarticular initially; polyarticular with recurrence | Sudden pain, often in one or a few joints; can mimic OA or RA |
| Serum marker | Uric acid elevated (but may be normal in 30% during acute attack) | No elevation of serum uric acid, calcium, or phosphate |
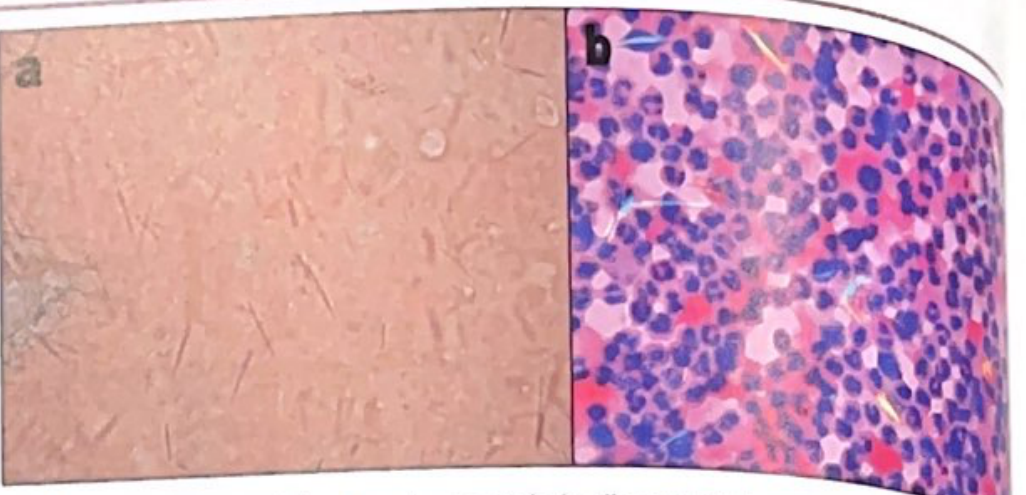
| Crystal morphology | Needle-shaped rods, 5-20 μm | Rhomboid (rectangular), 0.5-5 μm |
| Birefringence | Strongly NEGATIVE (yellow when parallel to compensator axis; blue when perpendicular) | POSITIVE (blue when parallel to compensator axis; yellow when perpendicular) |
| Radiographic sign | Soft tissue tophi, "rat-bite" erosions; double-contour sign + snowstorm sign on US | Chondrocalcinosis - calcification of hyaline cartilage or fibrocartilage |
| Crystals found in | Synovium, synovial fluid neutrophils | Hyaline cartilage and fibrocartilage first (then ruptures into joint) |
| Chronic form | Chronic tophaceous gout: tophi in periarticular tissue, cartilage destruction (~10 years after first attack) | Chronic CPPD: joint damage in ~50% of affected individuals; can mimic RA or OA |
| Extra-articular deposits | Tophi (ears, tendons, soft tissue), urate nephropathy, kidney stones | Primarily articular; no tophi |
Crystal Identification Under Polarized Light
| Gout (MSU) | Pseudogout (CPPD) | |
|---|---|---|
| Shape | Needle-shaped | Rhomboid |
| Birefringence | Negative (strongly) | Positive (weakly) |
| Color parallel to axis | Yellow | Blue |
| Color perpendicular to axis | Blue | Yellow |
| Location | Intracellular in neutrophils | Articular cartilage / synovial fluid |
Memory trick: "gout = negative = needle" - MSU crystals are needle-shaped with negative birefringence. CPPD are rhomboid with positive birefringence.
Pathogenesis (Shared Mechanism)
Both crystals activate the NLRP3 inflammasome in macrophages and neutrophils, triggering caspase-1 activation and release of IL-1, which recruits more leukocytes. Lysis of neutrophils releases lysosomal enzymes causing further tissue injury - a self-amplifying cycle of inflammation.
In CPPD, CPP crystals also physically disrupt cartilage matrix structure even in the absence of inflammation.
Stages of Gout (Not seen in Pseudogout)
- Asymptomatic hyperuricemia - begins around puberty in males, after menopause in females
- Acute gouty arthritis - sudden-onset, excruciating; 50% first attacks at 1st MTP joint
- Intercritical period - symptom-free interval; most have a second attack within months to years
- Chronic tophaceous gout - ~10 years after first attack; juxtaarticular bone erosion, joint space loss
Treatment
| Gout | Pseudogout | |
|---|---|---|
| Acute attack | NSAIDs (indomethacin 50 mg TID or naproxen 250-500 mg BD for 3-7 days), Colchicine (1.2 mg then 0.6 mg after 1 hr), Corticosteroids | Same - NSAIDs, colchicine, corticosteroids, IL-1 inhibitors |
| Long-term prevention | Allopurinol (xanthine oxidase inhibitor), probenecid (uricosuric), uricases; lifestyle: weight loss, dietary purine reduction, reduce alcohol | No known treatment that prevents or slows crystal formation; treat underlying metabolic cause |
| Lifestyle modifications | Reduce purines, alcohol, sugar-sweetened beverages; weight loss; exercise | Treat underlying condition (e.g., hyperparathyroidism, hemochromatosis) |
Sources: Robbins & Cotran Pathologic Basis of Disease, p. 1111-1113 | Tintinalli's Emergency Medicine, p. 76-95 | Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 602 | Miller's Review of Orthopaedics, 9th Ed.
What lab findings help diagnose gout vs pseudogout?
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Excellent - I now have all the data needed for a thorough, well-referenced answer.
Lab Findings: Gout vs. Pseudogout
1. Synovial Fluid Analysis - The Gold Standard
Arthrocentesis with synovial fluid examination is the only definitive way to distinguish gout from pseudogout. No serum test can do this reliably.
Fluid Collection Tips
- Crystal examination: collect in green-top tube (liquid heparin) - avoid powdered anticoagulant tubes as undissolved heparin crystals cause artifacts
- Cell count + differential: purple-top (EDTA)
- Culture/chemistry/serology: red-top (clot tube)
Synovial Fluid Profile Comparison
| Parameter | Normal | Gout | Pseudogout | Septic Arthritis | Osteoarthritis |
|---|---|---|---|---|---|
| Appearance | Clear, straw | Translucent to cloudy | Translucent to cloudy | Cloudy/purulent | Transparent |
| Viscosity | High | Low | Low | Variable | High |
| WBC count (cells/mm³) | <180 | 200 to >50,000 | 200-50,000 | 2,000 to >50,000 | 200-2,000 |
| PMN (%) | <10% | >90% | >90% | >90% | <10% |
| Crystals | None | MSU - needle-shaped | CPPD - rhomboid | None | Occasional CPPD/hydroxyapatite |
| Culture | Negative | Negative | Negative | Positive | Negative |
| String sign | Long, tenacious | Absent (low viscosity) | Absent (low viscosity) | Absent | Present |
Key caveat: WBC >50,000/mm³ is highly suggestive of septic arthritis, but gout and RA can also exceed this threshold. Always send culture to exclude co-existing infection.
A synovial WBC >2,000/mm³ is 84% sensitive and 84% specific for inflammatory arthritis of any cause.
2. Crystal Identification Under Polarized Light Microscopy
This is pathognomonic - crystal presence confirms the diagnosis.
| Feature | Gout (MSU) | Pseudogout (CPPD) |
|---|---|---|
| Shape | Needle-shaped rods | Rhomboid / rod / rectangular |
| Size | 5-20 μm (can be 1-2 μm) | 0.5-20 μm |
| Birefringence | Strongly NEGATIVE | Weakly POSITIVE |
| Color parallel to z-axis (compensator) | Yellow | Blue |
| Color perpendicular to z-axis | Blue | Yellow |
| Location | Intracellular in neutrophils (acute); extracellular between attacks | Articular cartilage first; then shed into fluid |
| Sensitivity | ~78% (polarized microscopy) | ~72% |
| Specificity | ~79% | ~67% |
Memory trick: "Negative = Needle = goUt" and "Pseudogout = Positive = rhomboPoid"
Important: MSU crystals are found in 90% of acute gout attacks and ~75% of patients between attacks. Many CPPD crystals are too small to polarize - use phase-contrast microscopy to improve detection.
3. Serum / Blood Tests
| Test | Gout | Pseudogout |
|---|---|---|
| Serum uric acid | Usually elevated (>6.8 mg/dL); but normal in up to 30% during acute attack - NOT reliable for acute diagnosis | Normal - no elevation |
| Serum calcium | Normal | Normal (no elevation even in CPPD) |
| Serum phosphate | Normal | Normal |
| ESR / CRP | Elevated (nonspecific) | Elevated (nonspecific) |
| WBC | May be mildly elevated | May be mildly elevated |
| Serum Mg, PTH, ferritin, TSH | Not relevant | Check if CPPD suspected: hypomagnesemia, hyperparathyroidism (elevated PTH/Ca), hemochromatosis (elevated ferritin), hypothyroidism (elevated TSH) |
Serum uric acid should not be used as a diagnostic test for acute gout - it is often misleadingly normal during the attack.
4. Imaging Findings
| Modality | Gout | Pseudogout |
|---|---|---|
| X-ray | Soft-tissue tophi; "rat-bite"/"overhanging edge" erosions (late disease) | Chondrocalcinosis - calcification of articular cartilage (pathognomonic) |
| Ultrasound | Double-contour sign (urate coating cartilage), tophi, snowstorm sign | Hyperechoic deposits within cartilage (midsubstance) |
| CT / Dual-energy CT | Can quantify urate deposits; DECT distinguishes urate from calcium | Identifies calcification |
| MRI | Not routinely used; can show tophi | Not routinely used |
5. Summary Diagnostic Approach
Suspected crystal arthritis
↓
Arthrocentesis (joint aspiration)
↓
Synovial fluid → polarized light microscopy
↓
Needle-shaped, NEGATIVE birefringence → GOUT (MSU)
Rhomboid, POSITIVE birefringence → PSEUDOGOUT (CPPD)
No crystals, +ve culture → Septic arthritis
↓
If CPPD confirmed → screen for secondary causes:
PTH, calcium (hyperparathyroidism)
Ferritin, transferrin sat. (hemochromatosis)
Magnesium (hypomagnesemia)
TSH (hypothyroidism)
Sources: Roberts & Hedges' Clinical Procedures in Emergency Medicine, p. 1276-1279 | Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 602 | Quick Compendium of Clinical Pathology, 5th ed. | Frameworks for Internal Medicine, p. 680 | Tintinalli's Emergency Medicine, p. 84-92
This is a shared conversation. Sign in to Orris to start your own chat.