Types of Nstemi and stemi with ecg images and description
Reading File
Finding Sources
Finding Sources
Searching Images
STEMI ECG ST elevation myocardial infarction types
Finding Sources
Finding Sources
Searching Images
NSTEMI ECG ST depression T wave inversion non-ST elevation
Reading File
Searching Images
inferior STEMI ECG leads II III aVF right coronary artery
Searching Images
posterior STEMI lateral STEMI ECG types territories
Finding Sources
Searching Images
right ventricular infarction ECG V1 V4R STEMI right sided leads
Reading File
Searching Images
Wellens syndrome T wave inversion anterior leads NSTEMI LAD
Now I have comprehensive material. Let me compile a thorough, well-illustrated response.
NSTEMI and STEMI — Types, ECG Findings, and Images
Understanding the Distinction
STEMI (ST-Elevation Myocardial Infarction) results from complete occlusion of a coronary artery, causing transmural (full-thickness) ischemia. The hallmark is ST-segment elevation in ≥2 contiguous leads.
NSTEMI (Non-ST-Elevation Myocardial Infarction) results from partial occlusion (or subtotal occlusion), causing subendocardial ischemia. Troponin is elevated but there is no ST elevation — instead, you see ST depression, T-wave inversion, or nonspecific changes.
Overview Comparison Diagram
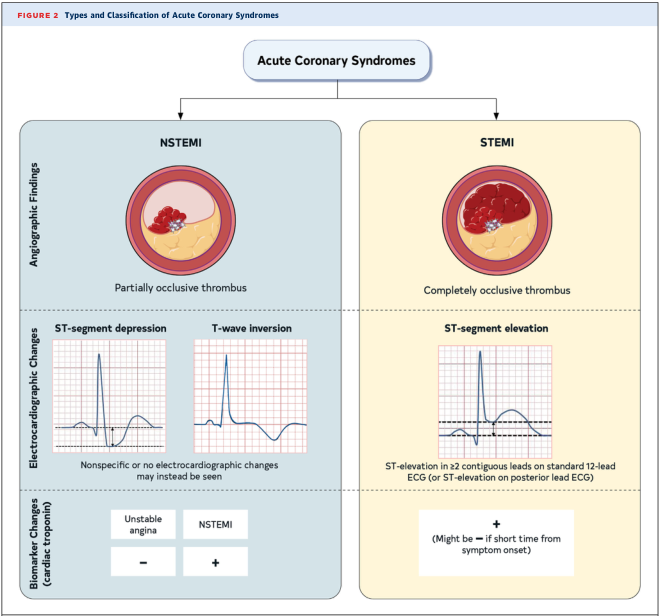
NSTEMI (partial thrombus, ST depression/T-wave inversion, troponin+) vs. STEMI (complete thrombus, ST elevation, troponin+). — Management of Patients With Acute Coronary Syndromes
STEMI — Types by Territory
STEMI is classified by the territory of infarction, which correlates with the culprit coronary artery and the ECG leads showing elevation.
1. Anterior STEMI
Artery: Left Anterior Descending (LAD)
Leads with ST elevation: V1–V4 (and I, aVL for anterolateral)
Reciprocal changes: ST depression in II, III, aVF
Wall affected: Anterior (and anteroseptal, anterolateral depending on extent)
Classic features: convex "tombstone" ST elevation in precordial leads, evolving Q waves in V2–V3
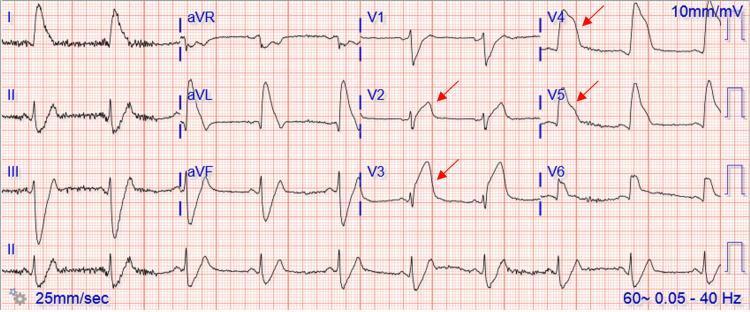
Anterior STEMI: ST elevation V2–V5, reciprocal depression in II, III, aVF. Proximal LAD occlusion pattern.
Anterior STEMI with evolving QS waves in V2–V3 (necrotic changes), tombstoning morphology.
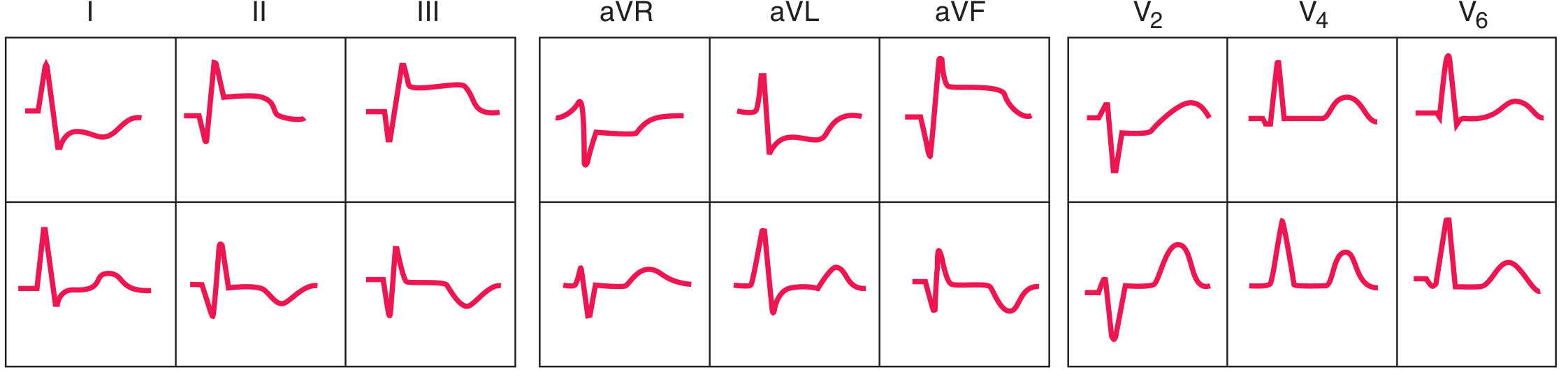
ECG Sequence (Acute → Evolving):
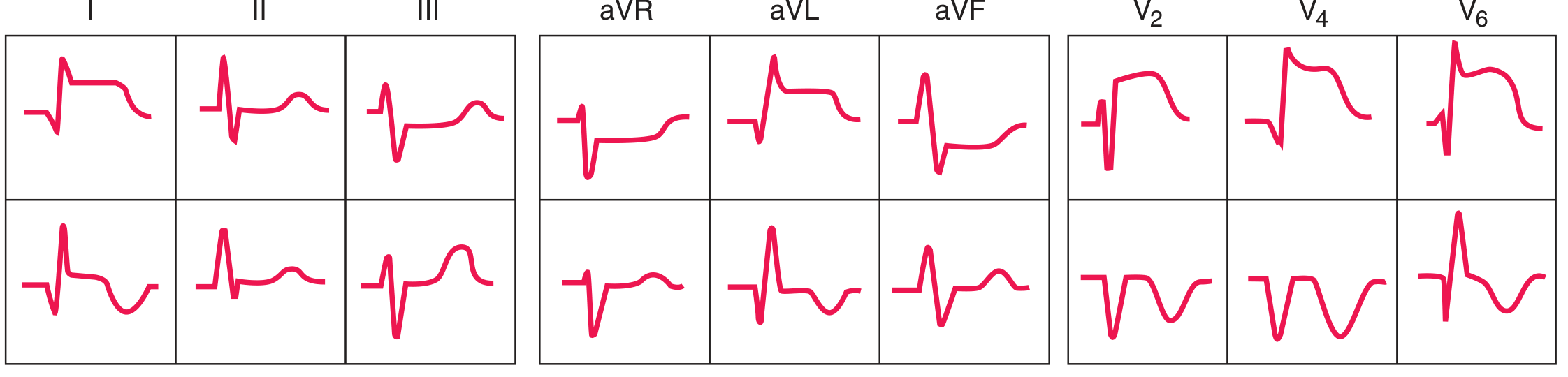
Acute and evolving anterior STEMI sequence — leads I, aVL, and V1–V6 showing progression to Q-wave formation. — Harrison's Principles of Internal Medicine, 22nd Ed.
2. Anterolateral STEMI
Artery: Proximal LAD or left main
Leads: V1–V6, I, aVL (extensive anterior involvement)
Reciprocal changes: ST depression in inferior leads

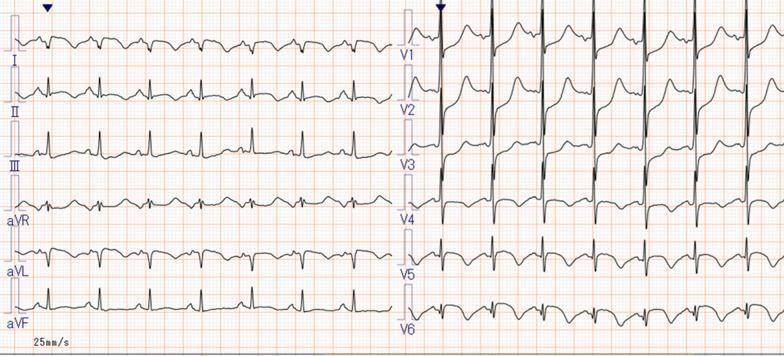
Anterolateral STEMI: V1–V6 + I, aVL elevation, hyperacute T waves V2–V4, reciprocal depression II/III/aVF. Proximal LAD/left main occlusion.
3. Inferior STEMI
Artery: Right Coronary Artery (RCA) ~80%, Left Circumflex (LCx) ~20%
Leads with ST elevation: II, III, aVF
Reciprocal changes: ST depression in I and aVL (high lateral leads)
Key clue: ST elevation in lead III > lead II → suggests RCA occlusion
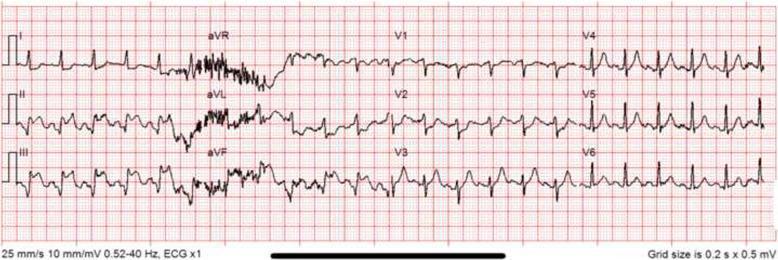
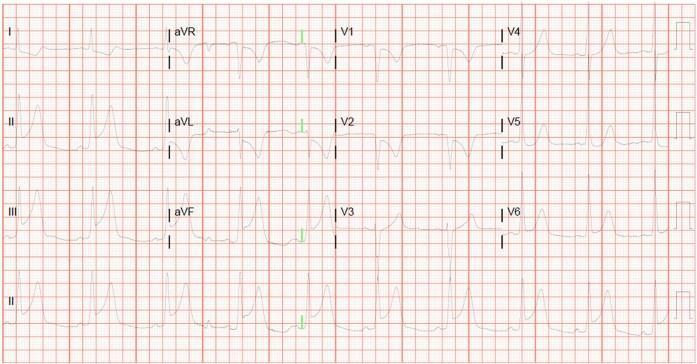
Inferior STEMI: ST elevation II/III/aVF, Q waves in III/aVF, reciprocal depression I/aVL, consistent with RCA occlusion.
Inferior STEMI with additional reciprocal changes in V4–V6, sinus rhythm.
ECG Sequence (Acute → Evolving):
Acute and evolving inferior STEMI — inferior leads showing Q-wave formation with reciprocal anterior depressions. — Harrison's Principles of Internal Medicine, 22nd Ed.
4. Inferior + Right Ventricular (RV) STEMI
Artery: Proximal RCA (before RV branches)
Leads: II, III, aVF (inferior) + V3R–V4R (right-sided leads, ≥1 mm elevation)
Clinical importance: RV infarction causes hypotension sensitive to nitrates and volume depletion — IV fluids are required, nitrates are contraindicated
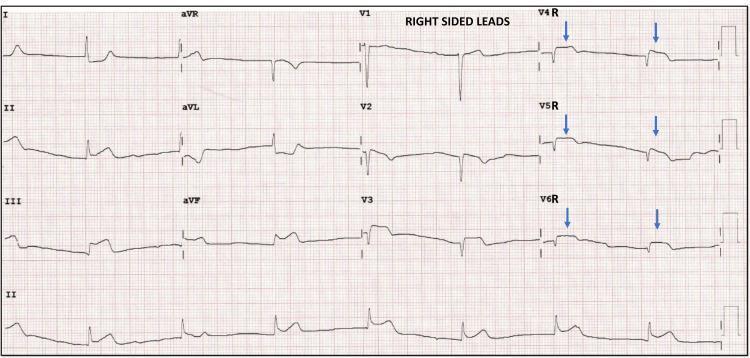
Inferior STEMI + right ventricular involvement: ST elevation in II/III/aVF and right-sided leads V4R–V6R (blue arrows). Proximal RCA occlusion.
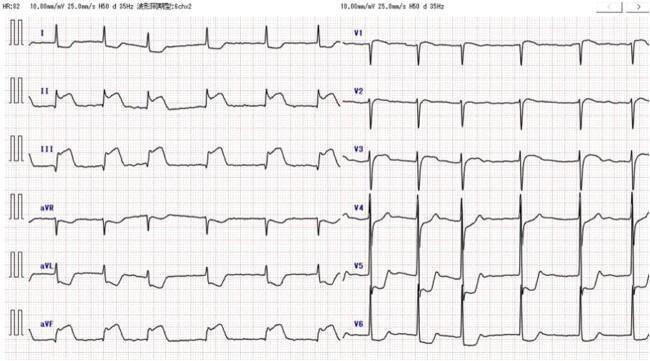
5. Inferior + Posterior STEMI
Artery: RCA (posterior descending branch) or LCx
Leads (direct): V7–V9 (posterior leads placed behind the heart)
Mirror image in standard leads: ST depression in V1–V3 + tall, upright T waves (reciprocal = mirror of posterior ST elevation)
Inferior + posterior STEMI: elevation in II/III/aVF + ST depression/tall T waves in V1–V3 (posterior mirror). Reciprocal changes in aVL.
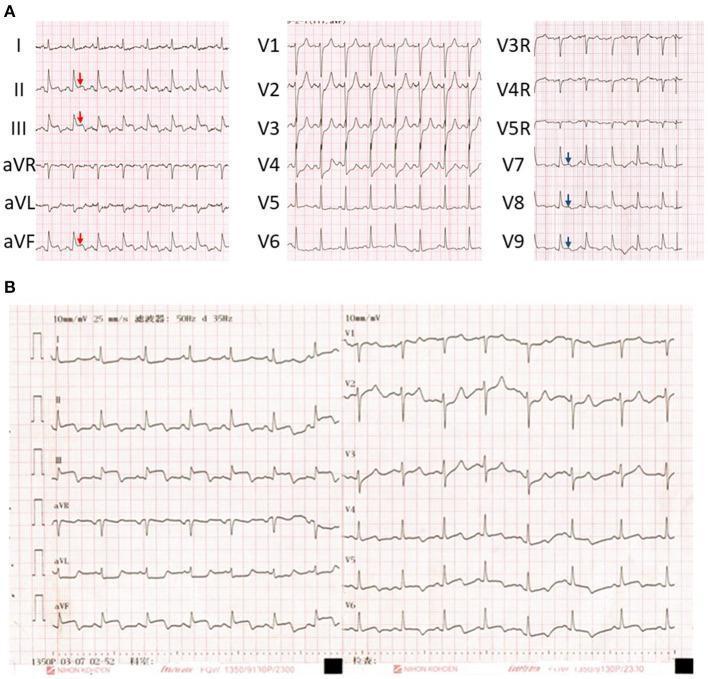
Panel A (admission) vs. Panel B (day 2): inferior STEMI (red arrows) + posterior leads V7–V9 (blue arrows), with reciprocal depression V1–V4.
6. Lateral STEMI
Artery: Left Circumflex (LCx) or diagonal branch of LAD
Leads: I, aVL (high lateral) and/or V5–V6 (low lateral)
Reciprocal changes: ST depression in II, III, aVF (when high lateral)
High lateral STEMI (I, aVL, V5–V6) + posterior extension (reciprocal depression V1–V3). LCx distribution.
7. Inferolateral STEMI
Artery: LCx (dominant or large)
Leads: II, III, aVF + V5–V6 ± I, aVL
Inferolateral STEMI: elevation in V4–V6 + inferior leads, hyperacute T waves, reciprocal depression in aVL and I.
NSTEMI — ECG Patterns
NSTEMI produces no ST elevation. Instead, look for:
| Pattern | Description |
|---|---|
| ST depression | Horizontal or downsloping ≥0.5 mm in ≥2 contiguous leads |
| T-wave inversion | Symmetric, deep T-wave inversion, especially V1–V4 |
| Nonspecific changes | Flat T waves, subtle changes — ECG may even be normal |
| Wellens' syndrome | T-wave pattern indicating critical proximal LAD stenosis (pre-infarction warning) |
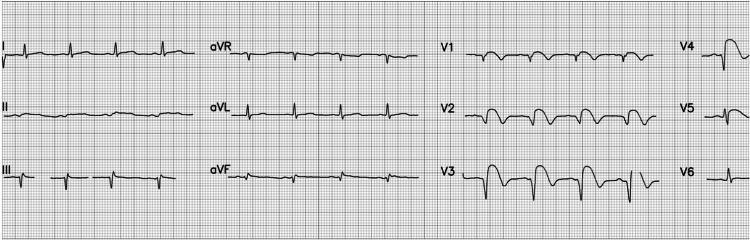
NSTEMI — Serial ECG Progression
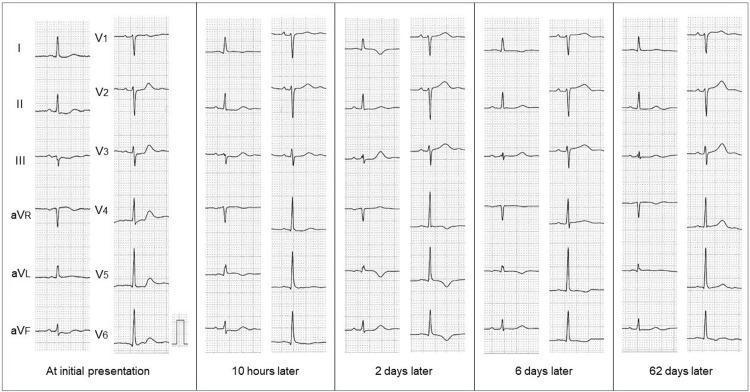
Serial ECGs in NSTEMI: initial ST depression (inferior + precordial leads) → dynamic T-wave inversions (I, aVL, V4–V6) at 2–6 days → resolution by 62 days. Classic anterolateral subendocardial ischemia.
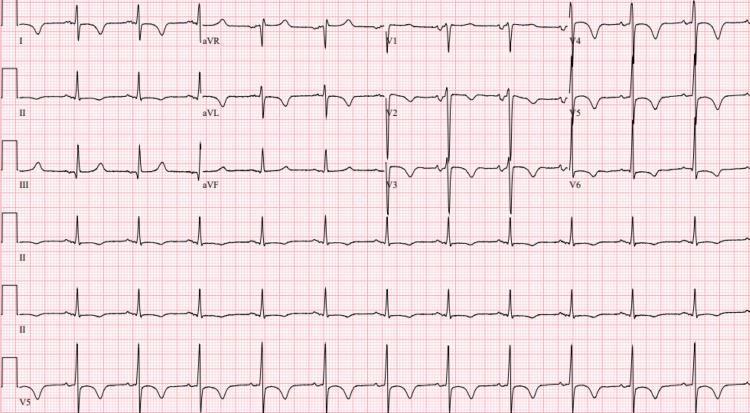
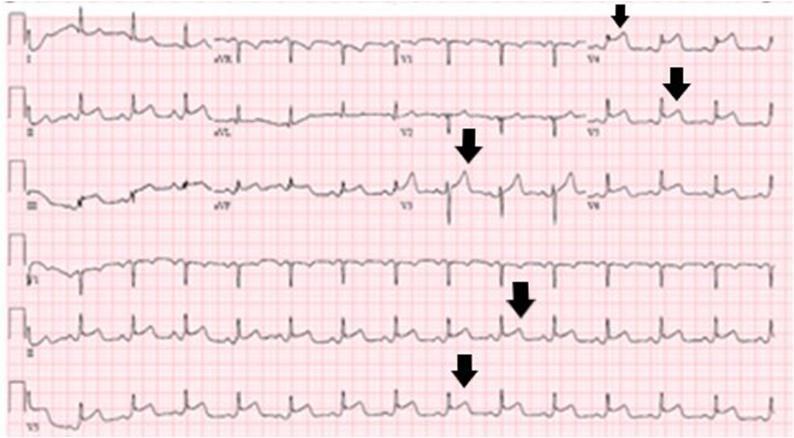
NSTEMI: widespread ST-segment depression and deep symmetric T-wave inversions in V1–V6, I, aVL — may indicate multi-vessel disease. QTc prolonged at 497 ms.
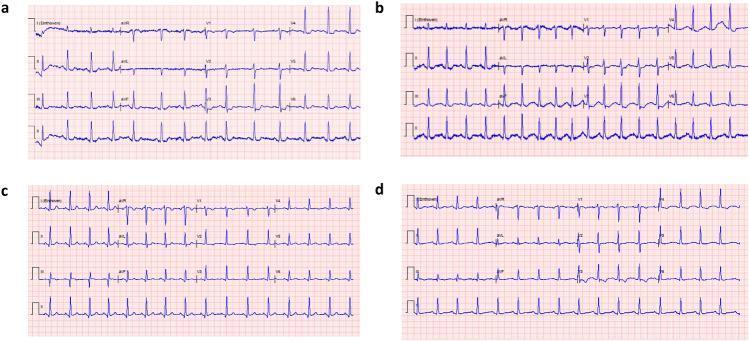
Serial NSTEMI ECGs: horizontal ST depression V3–V5 (panel a) improving after nitrates (panel b–c) and fully normalizing before discharge (panel d).
Wellens' Syndrome (High-Risk NSTEMI Equivalent)
A pattern of T-wave changes in V2–V3 during a pain-free period — indicates critical proximal LAD stenosis and impending anterior STEMI. Do NOT stress test — requires urgent angiography.
Type A (Biphasic T waves):
Wellens' Type A: biphasic T waves in V2–V3 — initial upward deflection followed by deep terminal inversion. Highly specific for proximal LAD stenosis.
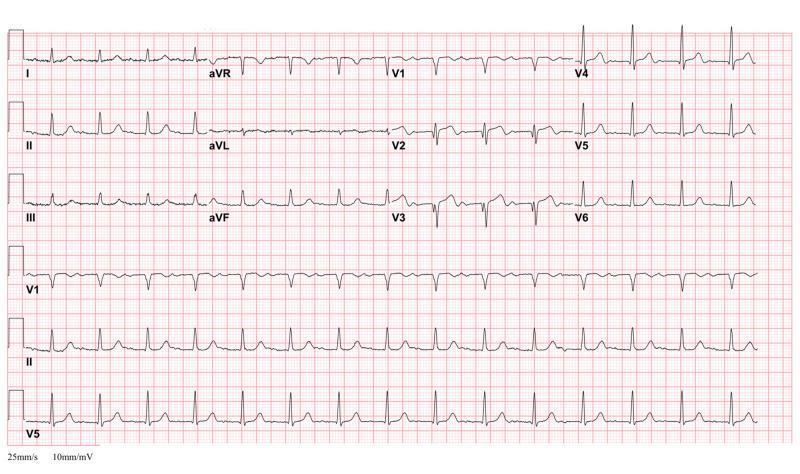
Type B (Deep symmetric T-wave inversion):

Wellens' Type B: deep, symmetric T-wave inversion V1–V6 with isoelectric ST and preserved R-wave progression. Pain-free at time of ECG. Critical LAD stenosis.
Summary Table
| Type | Territory | Culprit Artery | Leads with ST Elevation | Reciprocal Leads |
|---|---|---|---|---|
| Anterior STEMI | Anterior wall | LAD (mid-distal) | V1–V4 | II, III, aVF |
| Anterolateral STEMI | Anterior + Lateral | Proximal LAD / Left main | V1–V6, I, aVL | II, III, aVF |
| Inferior STEMI | Inferior wall | RCA (80%), LCx (20%) | II, III, aVF | I, aVL |
| Inferior + RV STEMI | Inferior + RV | Proximal RCA | II, III, aVF + V3R–V4R | I, aVL |
| Posterior STEMI | Posterior wall | RCA or LCx | V7–V9 (or mirror: V1–V3 depression) | V1–V3 (ST elevation) |
| Lateral STEMI | Lateral wall | LCx / Diagonal | I, aVL, V5–V6 | II, III, aVF |
| Inferolateral STEMI | Inferior + Lateral | LCx | II, III, aVF, V5–V6 | I, aVL |
| NSTEMI | Subendocardial | Partial any vessel | None (ST depression, T inversion) | N/A |
| Wellens' syndrome | Proximal LAD at risk | Proximal LAD stenosis | Biphasic or inverted T V2–V3 | N/A |
Key clinical points:
- All STEMI types require immediate reperfusion (PCI < 90 min or thrombolytics < 30 min)
- RV infarction: avoid nitrates and diuretics; give IV fluids
- Posterior STEMI is frequently missed on standard 12-lead — always get posterior leads (V7–V9) when inferior changes + ST depression in V1–V3
- NSTEMI diagnosis requires elevated troponin + symptoms/ECG changes — ECG alone may be normal in up to 30%
- Wellens' syndrome is a pre-infarction warning — urgent catheterization, no stress testing
This is a shared conversation. Sign in to Orris to start your own chat.