Give me a detailed answer on Erthropoeitin with relevant simple diagrams
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Generating Image
Simple clean medical diagram showing Erythropoietin (EPO) physiology with two panels: Left panel shows the production pathway - kidney (peritubular fibroblasts) detecting hypoxia → HIF-1α activation → EPO gene transcription → EPO release into blood. Right panel shows EPO action in bone marrow - EPO binds EPO receptor on proerythroblast → JAK2/STAT5 signaling → differentiation to mature red blood cells (RBCs). Include a feedback loop arrow showing increased RBCs correcting hypoxia. Use clean arrows, labeled boxes, and simple icons. White background, medical textbook style.
I now have all the information and images needed for a thorough, well-illustrated answer. Let me compile the complete response.
Erythropoietin (EPO) - A Comprehensive Overview
1. What Is Erythropoietin?
Erythropoietin (EPO) is a glycoprotein hormone - the major regulator of red blood cell (erythrocyte) production. It contains 165 amino acid residues and four oligosaccharide chains, giving it a molecular weight of approximately 30.4-39 kDa (the glycosylation chains are essential for its activity in vivo). It was the first human hematopoietic growth factor to be isolated, originally purified from the urine of patients with severe anemia.
2. Where Is EPO Produced? (Sources)
| Source | Contribution |
|---|---|
| Kidney (peritubular interstitial fibroblasts, renal cortex) | ~85% in adults |
| Liver (perivenous hepatocytes) | ~15% in adults |
| Brain | Small amount (neuroprotective role) |
| Uterus/oviducts | Induced by estrogen; involved in angiogenesis |
The kidney is the dominant and physiologically most important source. Renal peritubular fibroblasts (located in the renal cortex) are the primary EPO-producing cells. When renal mass is reduced by disease or nephrectomy, the liver cannot compensate - anemia develops as a result.
- Ganong's Review of Medical Physiology, 26th Ed.
- Brenner and Rector's The Kidney
3. How Is EPO Produced? The Hypoxia Sensing Mechanism
The key trigger for EPO synthesis is hypoxia (reduced oxygen delivery to the kidneys). This occurs when:
- Hemoglobin concentration falls (anemia)
- Arterial PO2 falls (pulmonary disease, high altitude)
The pathway (step by step):
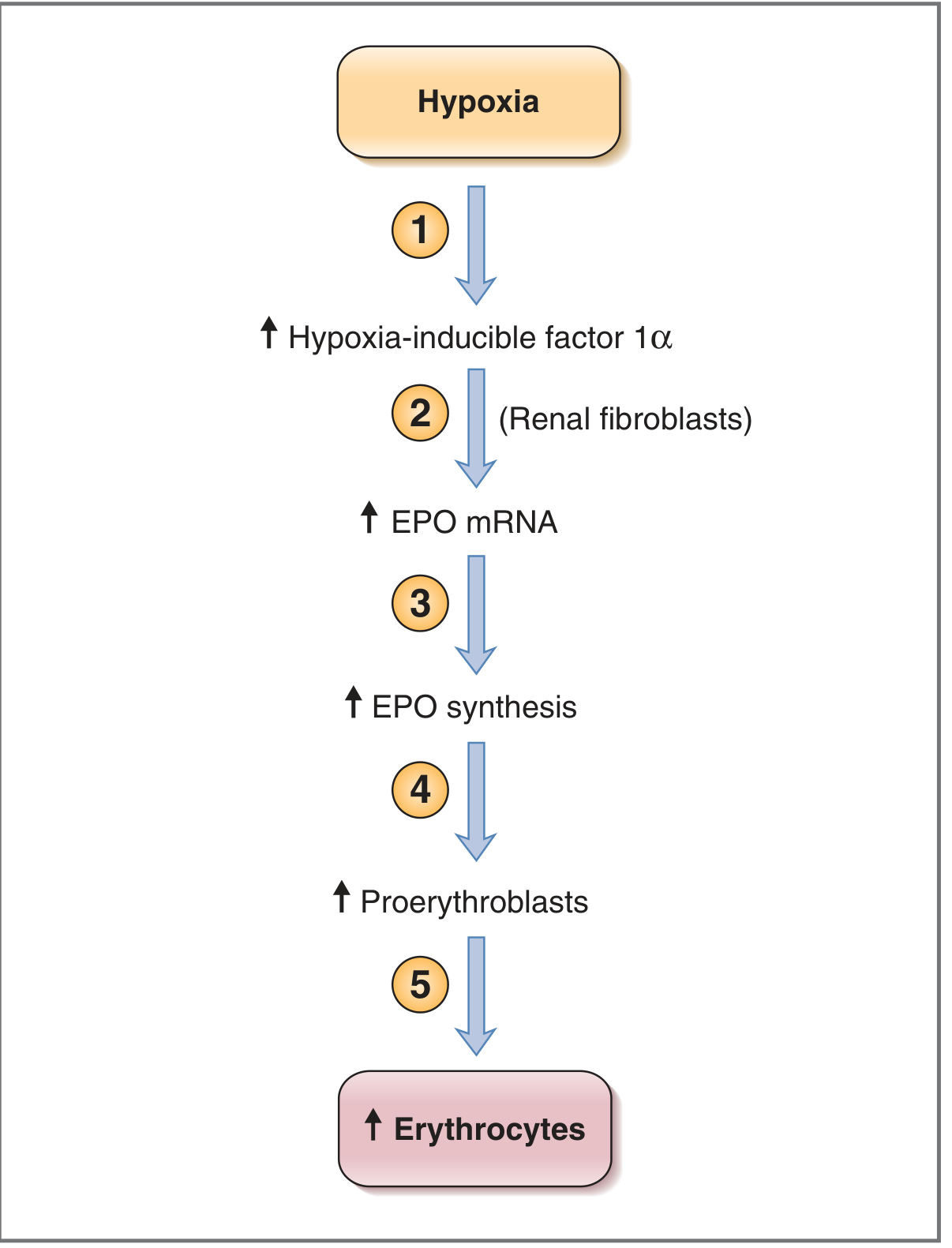
Step-by-step:
- Hypoxia detected in the kidney
- Hypoxia stabilizes the alpha subunit of Hypoxia-Inducible Factor 1 (HIF-1α) - under normoxia, HIF-1α is hydroxylated by prolyl hydroxylases (PHDs) and rapidly degraded; under hypoxia, this degradation is blocked
- HIF-1α acts on renal peritubular fibroblasts → stimulates transcription of the EPO gene → increases EPO mRNA
- Increased EPO mRNA → increased EPO synthesis and secretion into the bloodstream
- EPO acts on the bone marrow → proerythroblast differentiation → mature erythrocytes
- More RBCs → improved O2 delivery → negative feedback reduces HIF-1α → EPO production falls
Key insight: The kidney distinguishes between decreased blood flow (which also reduces Na+ reabsorption and O2 consumption equally) vs. decreased O2 content of blood. Only the latter triggers EPO - a very elegant oxygen-sensing system. - Costanzo Physiology, 7th Ed.
4. Mechanism of Action (EPO Receptor Signaling)
EPO binds to the EPO receptor (EPOR) on erythroid progenitor cells in the bone marrow.
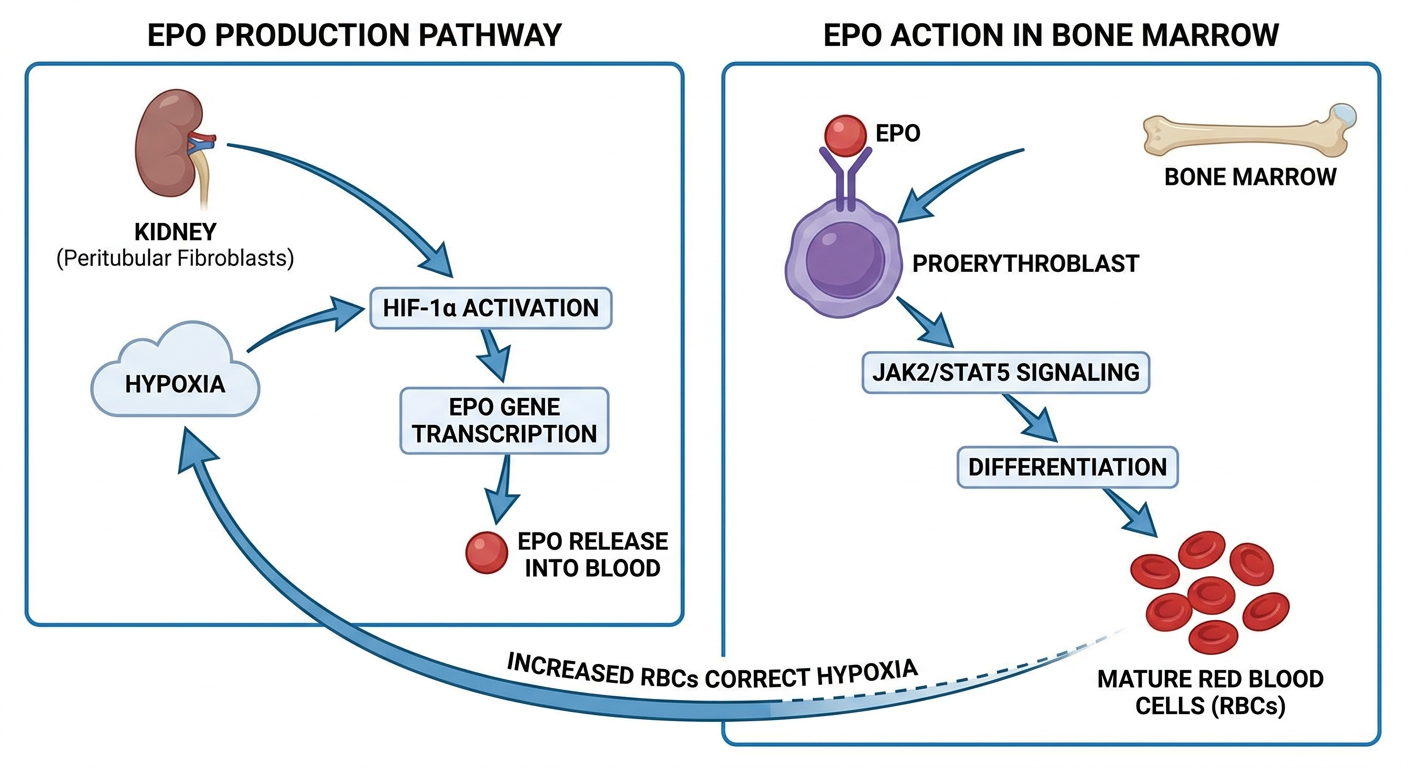
The receptor and signaling cascade:
- EPOR is a linear protein with a single transmembrane domain, a member of the cytokine receptor superfamily (JAK/STAT superfamily)
- When EPO binds → receptor dimerization → activation of JAK2 (Janus Kinase 2)
- JAK2 phosphorylates STAT5 (Signal Transducer and Activator of Transcription 5)
- STAT5 dimerizes, enters the nucleus, and drives gene transcription
- This activates a cascade of serine and threonine kinases → inhibits apoptosis of erythroid progenitors + promotes their growth and differentiation
Effects of EPO on erythroid cells:
-
Stimulates proliferation and differentiation of erythroid progenitors (CFU-E, BFU-E)
-
Causes proerythroblasts to differentiate into mature erythrocytes
-
Induces release of reticulocytes from the bone marrow
-
Later maturation steps (reticulocyte → mature RBC) do NOT require EPO
-
Katzung's Basic and Clinical Pharmacology, 16th Ed.
-
Ganong's Review of Medical Physiology, 26th Ed.
5. EPO Levels vs. Hematocrit - The Inverse Relationship
There is a classic inverse, exponential relationship between hematocrit/hemoglobin and serum EPO:
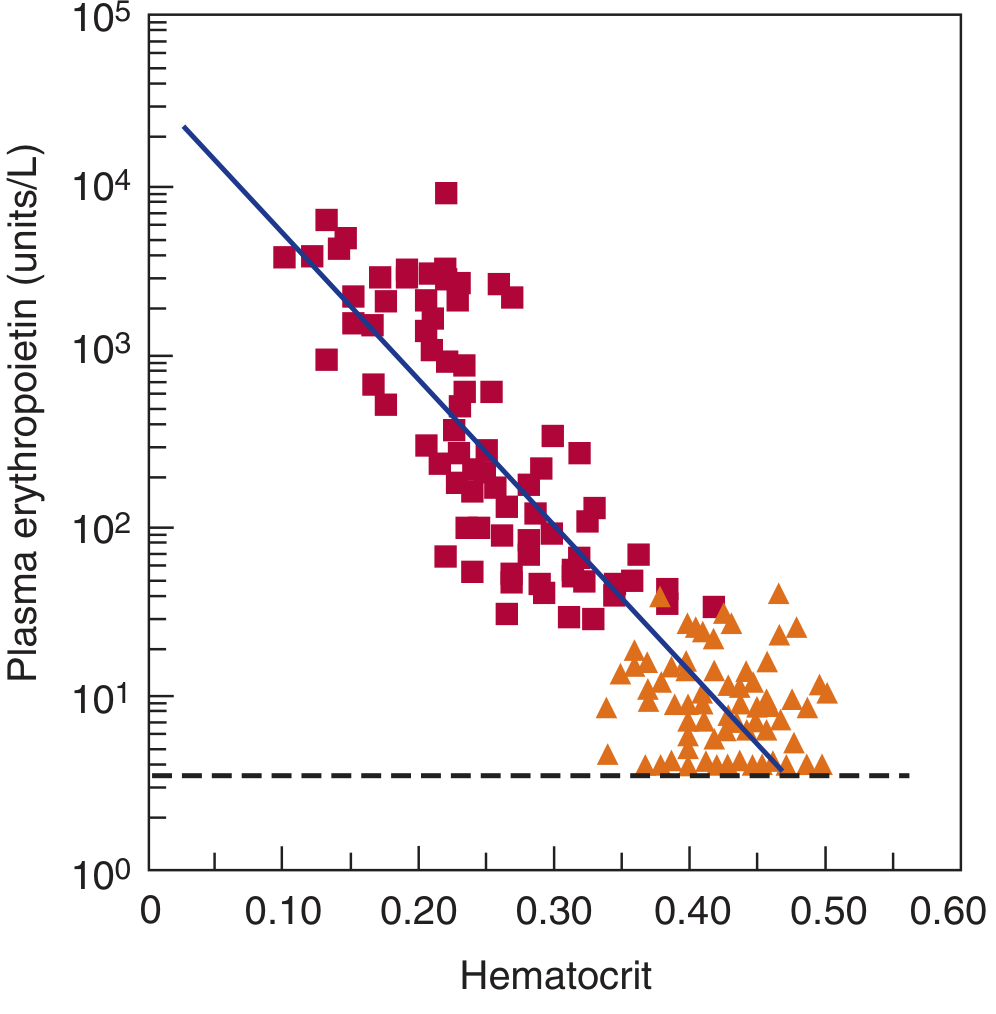
| Condition | Serum EPO Level |
|---|---|
| Normal (non-anemic) | < 20 IU/L |
| Moderately severe anemia | 100-500 IU/L |
| Severe anemia | Thousands of IU/L |
| Chronic renal failure | Low (despite anemia) |
Exception: In chronic kidney disease (CKD), EPO levels are inappropriately low despite anemia, because the damaged kidneys cannot produce adequate EPO. This is the principal cause of anemia in CKD.
6. EPO Pharmacokinetics
| Property | Epoetin alfa (rHuEPO) | Darbepoetin alfa | Methoxy PEG-epoetin beta |
|---|---|---|---|
| Half-life (IV) | 4-13 hours | 2-3x longer than epoetin | Much longer (weeks) |
| Glycosylation | Standard | Hyperglycoylated (2 extra chains) | PEGylated |
| Dosing | 3x/week | Weekly | 2-weekly or monthly |
| Not cleared by | Dialysis | Dialysis | Dialysis |
The principal site of inactivation is the liver. Despite the short half-life, the clinical effect (increased RBCs) takes 2-3 days to appear because red cell maturation is slow. - Ganong's, Katzung's
7. Clinical Uses (Erythropoiesis-Stimulating Agents - ESAs)
| Indication | Notes |
|---|---|
| Anemia of CKD (primary use) | 90% of end-stage renal disease patients on dialysis are EPO-deficient |
| Cancer chemotherapy-induced anemia | When Hb < 10 g/dL; NOT for curative-intent chemotherapy |
| HIV patients on zidovudine | Zidovudine suppresses marrow |
| Elective non-cardiac, non-vascular surgery | Reduce need for transfusions |
| Low-risk myelodysplastic syndrome | Selected patients |
Treatment monitoring:
- Reticulocyte count rises in ~10 days
- Hematocrit/Hb rises in 2-6 weeks
- Target Hb: 10-11 g/dL (do NOT exceed 12 g/dL in CKD)
- Nearly all CKD patients also need iron supplementation (oral or IV), and some need folate
Patients most likely to respond: those with endogenous EPO < 100 IU/L relative to their degree of anemia (i.e., EPO-deficient states). - Katzung's Basic and Clinical Pharmacology, 16th Ed.
8. Adverse Effects and Toxicity
| Adverse Effect | Details |
|---|---|
| Hypertension | Most common; mechanism involves increased blood viscosity and vasoconstriction |
| Thrombotic complications | Increased risk of stroke, MI, PE, DVT - especially at Hb > 11 g/dL |
| Pure Red Cell Aplasia (PRCA) | Rare; due to neutralizing antibodies against EPO; mainly seen with subcutaneous administration in CKD patients |
| Allergic reactions | Infrequent |
Meta-analysis of 51 trials in cancer patients showed increased all-cause mortality and venous thrombosis with ESAs - hence the conservative guidelines. - Katzung's, 16th Ed.
9. Anemia of Chronic Kidney Disease - The Big Picture
CKD causes EPO deficiency because:
- Loss of functioning renal mass → loss of peritubular EPO-producing fibroblasts
- Uremic toxins may also impair bone marrow response
- Dialysis does NOT clear EPO (but it also doesn't help produce it)
Iron, folate, and vitamin B12 deficiency further impair the bone marrow's ability to respond to EPO. Even with adequate EPO, these cofactors must be present for effective erythropoiesis. - Brenner and Rector's The Kidney
10. Emerging Therapies - HIF-PHD Inhibitors
A newer pharmacological approach exploits the HIF pathway:
- Prolyl hydroxylase domain (PHD) inhibitors (e.g., Roxadustat) block the enzyme that degrades HIF-1α under normoxia
- This artificially mimics hypoxia → increases endogenous EPO production
- Already banned in competitive sport
- In clinical trials for CKD anemia
This research led to the 2019 Nobel Prize in Physiology or Medicine (William Kaelin, Peter Ratcliffe, Gregg Semenza). - Katzung's Basic and Clinical Pharmacology, 16th Ed.
Quick Summary
HYPOXIA (↓O2 delivery to kidneys)
↓
HIF-1α stabilized (PHDs blocked)
↓
EPO gene transcription (renal fibroblasts)
↓
EPO released into bloodstream
↓
EPO binds EPOR on bone marrow progenitors
↓
JAK2 → STAT5 → anti-apoptosis + differentiation
↓
More RBCs → O2 delivery restored → EPO falls (negative feedback)
Key facts to remember:
- EPO = 165 aa glycoprotein, ~30-39 kDa
- 85% kidney (peritubular fibroblasts), 15% liver
- Trigger = hypoxia via HIF-1α
- Receptor = JAK/STAT superfamily (JAK2/STAT5)
- Normal serum EPO < 20 IU/L
- Main clinical use = anemia of CKD
- Main danger = hypertension + thrombosis at high Hb targets
- New approach = HIF-PHD inhibitors (roxadustat)
This is a shared conversation. Sign in to Orris to start your own chat.