Deviated nasal septum
Reading File
Finding Sources
Finding Sources
Searching PubMed
"deviated nasal septum" AND septoplasty
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
I now have sufficient information from authoritative textbooks to compose a comprehensive answer. Let me compile everything:
Deviated Nasal Septum (DNS)
Definition
A deviated nasal septum (DNS) is a displacement of the nasal septum from the midline, resulting in asymmetry of the two nasal passages. It is one of the most common causes of unilateral nasal airway obstruction.
- Cummings Otolaryngology, p. 567
Anatomy of the Nasal Septum
The nasal septum is composed of:
- Quadrangular (septal) cartilage - the main anterior cartilaginous component
- Perpendicular plate of ethmoid - superior bony support
- Vomer - posterior and inferior bony support
- Maxillary crest and palatine bone - inferior bony floor
The septum serves to divide the nasal cavity into two chambers, support the nasal dorsum, and maintain the shape of the columella and tip. Airflow through the nasal cavity (50% along the nasal floor) depends critically on septal position.
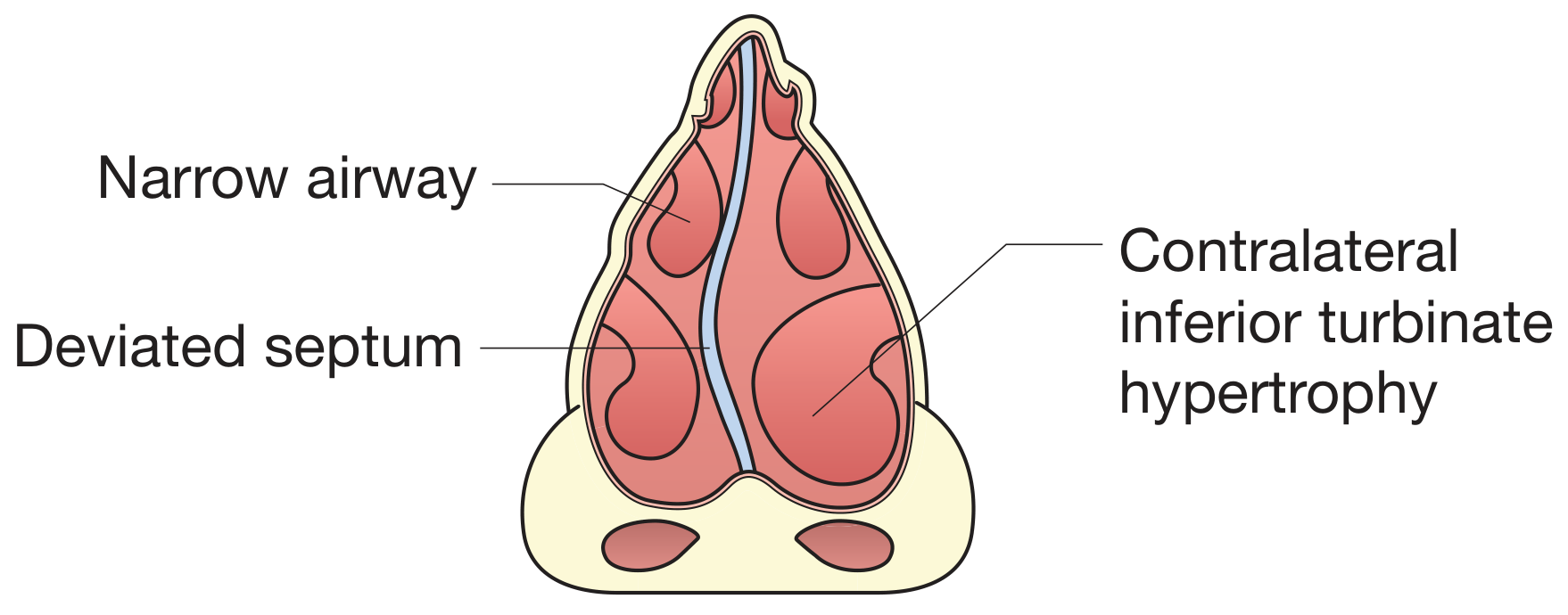
Coronal section through the anterior nasal fossae with deviated nasal septum to the right side, showing compensatory contralateral inferior turbinate hypertrophy (Bailey & Love's Surgery, Fig. 51.40)
Etiology
| Cause | Details |
|---|---|
| Trauma | Most common - nasal or midfacial injury, forceps delivery, passage through narrow pelvic canal |
| Birth trauma | Forceps or pressured delivery can cause microfractures that become evident at puberty |
| Developmental | Asymmetric chondrocyte growth due to early injury; uneven growth of facial skeleton |
| Idiopathic | Up to 50% of individuals without significant nasal injury have a DNS |
Minor trauma early in life causes microfractures of septal cartilage; healing leads to bending of cartilage away from the site of injury. When occurring in childhood, this may lead to asymmetric growth of the entire nasal structure.
- Cummings Otolaryngology, p. 567
Classification
DNS can be classified by shape and location:
- C-shaped - single curve to one side
- S-shaped - double curve, bilateral obstruction
- Septal spur - sharp angulation into the nasal passage
- Caudal dislocation - caudal end of septum displaced into one nostril
- High septal deviation - at the nasal valve area (most functionally significant)
Clinical Features
Symptoms
- Nasal obstruction - unilateral or bilateral, chronic, non-fluctuating (unlike allergic rhinitis)
- Recurrent sinusitis - impaired drainage of paranasal sinuses; septal deviation is a recognized predisposing factor for chronic rhinosinusitis
- Headache - from contact between deviated septum and turbinates
- Epistaxis - deviated cartilage disrupts laminar airflow, causing drying and irritation of mucosa with development of septal varices
- Snoring and sleep-disordered breathing - DNS contributes to nasal airway obstruction in OSA
- Impaired olfaction - from disrupted airflow
- Reduced humidification and filtration
Paradoxical Nasal Obstruction
An important concept: patients with unilateral septal deviation often complain of obstruction on the contralateral (open) side. This occurs because compensatory turbinate hypertrophy develops in the wider passage. Decongesting the nose and testing each nostril separately or showing endoscopic images helps the patient understand this phenomenon.
- Cummings Otolaryngology, p. 567-568
Examination
| Method | Findings |
|---|---|
| Anterior rhinoscopy | Direct visualization of deviation; most evident with nasal speculum and headlight |
| Nasal endoscopy | Gold standard for detailed assessment; identifies posterior deviations, spurs, turbinate size, and mucosal disease |
| Cottle maneuver | Lateral traction of cheek to open internal nasal valve - limited specificity; cotton-tipped applicator more specific |
| CT sinuses | Coronal CT identifies anatomical variants (concha bullosa, paradoxical turbinates), assesses sinuses, and delineates bony vs. cartilaginous deviation |
Objective Measurement
- Acoustic rhinometry - measures nasal cavity cross-sectional area using reflected sound waves; non-invasive
- Rhinomanometry - measures nasal airflow and resistance
- NOSE score (Nasal Obstruction Symptom Evaluation) - validated patient-reported outcome tool
- Visual Analog Scale (VAS) - for symptom severity
Differential Diagnosis
- Allergic/vasomotor rhinitis (bilateral, fluctuating, decongestion helps)
- Nasal polyps (pale, glistening masses)
- Hypertrophic inferior turbinate
- Nasal valve collapse
- Neoplasm (unilateral, progressive)
- Adenoidal hypertrophy (children)
Management
Medical (Non-surgical)
- Nasal saline irrigation - symptomatic relief, mucosal hydration
- Intranasal corticosteroids - reduce mucosal edema; most insurers require 6 weeks of documented failure before approving surgery
- Antihistamines + decongestants - for any concurrent allergic component
- External nasal dilators (e.g., Breathe Right strips) - increase internal nasal valve angle
A 2025 systematic review and meta-analysis (Taha et al., PMID 39230606) confirmed that septoplasty provides superior outcomes over non-surgical management in RCTs.
Surgical
1. Septoplasty (Preferred)
The current standard of care. The deformed septal cartilage is reshaped and repositioned rather than removed, preserving structural support.
Key principles:
- Elevate bilateral mucoperichondrial flaps
- Correct the anatomical abnormalities causing deformity (twisted cartilage, maxillary crest deviation, bony septum inclination)
- Preserve a minimum 1 cm dorsal strut and 1 cm caudal strut (L-strut) to maintain nasal support
- Often combined with turbinate reduction when compensatory hypertrophy is present
- Can be combined with rhinoplasty (septorhinoplasty)
Incision options:
- Hemitransfixion or Killian incision (standard)
- Open approach for complex/caudal deviations
2. Submucous Resection (SMR)
Older technique - deformed septal cartilage is excised, leaving only dorsal and caudal struts for support. Risk of saddle nose deformity if too much cartilage is removed.
3. Endoscopic Septoplasty
Used for limited or posterior deviations; provides magnified visualization.
- Bailey & Love's Surgery, p. 787; Cummings Otolaryngology, p. 568-572
Complications of Septal Surgery
| Complication | Notes |
|---|---|
| Septal perforation | Most common serious complication; from bilateral mucosal tears at same site |
| Saddle nose deformity | Excessive cartilage removal in SMR; loss of dorsal support |
| Tip ptosis / drooping | Loss of caudal support |
| Persistent obstruction | Under-resection, unaddressed turbinate hypertrophy, or nasal valve collapse |
| Septal hematoma | Requires prompt drainage to prevent cartilage avascular necrosis and abscess |
| CSF leak | Rare; from damage to cribriform plate |
| Anosmia | Rare; from cribriform damage |
| Columellar retraction | After endorotation during septoplasty |
DNS and Associated Conditions
- Chronic Rhinosinusitis (CRS): DNS impairs sinus ostial drainage; identified as an important anatomical variant on CT. Combined with concha bullosa or paradoxical turbinates, it significantly narrows the middle meatus. (Grainger & Allison's Diagnostic Radiology)
- Obstructive Sleep Apnea: Nasal obstruction from DNS contributes to OSA; assessment for DNS is part of the sleep-disordered breathing workup. (Scott-Brown's Otorhinolaryngology)
- Epistaxis: Kiesselbach's plexus (Little's area) is particularly vulnerable when laminar airflow is disrupted by a deviated septum.
- Allergic Rhinitis: DNS combined with allergic rhinitis worsens outcomes; a 2024 meta-analysis (PMID 39572690) found septoplasty in this group significantly improves nasal symptom scores.
Recent Evidence
- Septoplasty vs. non-surgical management (Taha et al. 2025, PMID 39230606): Systematic review of RCTs - septoplasty shows significantly better nasal obstruction symptom scores and objective airflow measures vs. conservative treatment.
- Septoplasty + allergic rhinitis (Wu et al. 2024, PMID 39572690): Meta-analysis confirms significant improvement in TNSS and VAS scores post-septoplasty in patients with concurrent allergic rhinitis.
- Sphenopalatine ganglion block post-septoplasty (Albazee et al. 2024, PMID 39323198): Effective for post-operative pain management.
Sources: Cummings Otolaryngology Head and Neck Surgery (Ch. 29); Bailey & Love's Short Practice of Surgery, 28th Ed. (Ch. 51); Scott-Brown's Otorhinolaryngology; Grainger & Allison's Diagnostic Radiology; Gray's Anatomy for Students.
This is a shared conversation. Sign in to Orris to start your own chat.