Explain heart murmurs in detail (easily)
Reading File
Finding Sources
Searching the Web
heart murmurs types causes explained simply
Reading File
Finding Sources
Searching Images
heart murmur diagram cardiac cycle sounds
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have thorough content from Harrison's and the Harriet Lane Handbook. Let me compile a comprehensive, easy-to-understand explanation.
🫀 Heart Murmurs — A Clear, Detailed Guide
What Is a Heart Murmur?
Your heart makes two normal sounds — "lub" (S1) and "dub" (S2) — as its valves snap shut with each beat. A heart murmur is an extra whooshing, swishing, or rumbling sound heard between those two normal sounds. It is caused by turbulent blood flow — similar to the sound of water rushing through a narrow garden hose.
Murmurs are not diseases themselves; they are sounds that may (or may not) indicate an underlying problem.
Why Does Turbulence Happen?
Three main mechanisms create turbulence:
| Mechanism | Example |
|---|---|
| Blood forced through a narrowed opening | Aortic stenosis (stiff aortic valve) |
| Blood leaking backward through a faulty valve | Mitral regurgitation |
| Blood flowing through an abnormal hole | Ventricular septal defect (VSD) |
| Increased speed of normal flow | Fever, pregnancy, anemia |
Innocent vs. Pathological Murmurs
✅ Innocent (Benign) Murmurs
Also called functional murmurs — the heart is structurally normal, but blood is moving faster than usual.
Causes: fever, pregnancy, anemia, hyperthyroidism, exercise, childhood growth spurts.
Features that suggest a murmur is innocent:
- Soft (grade 1–2/6)
- Mid-systolic (heard in the middle of the heartbeat)
- No other symptoms
- No radiation to the neck or axilla
- Normal ECG and chest X-ray
These murmurs require no treatment and often disappear on their own.
⚠️ Pathological (Abnormal) Murmurs
Caused by a structural problem in the heart. Red flags include:
- Loud murmur (grade ≥ 3/6) or harsh quality
- Diastolic murmur (diastolic murmurs are almost always pathological)
- Holosystolic (pan-systolic) — lasts the entire heartbeat
- Associated symptoms: chest pain, breathlessness, fainting, cyanosis (bluish lips)
- Abnormal ECG or chest X-ray
Timing — The Most Important Feature
The cardiac cycle has two phases:
- Systole = ventricles contract, blood is pumped out
- Diastole = ventricles relax, filling with blood
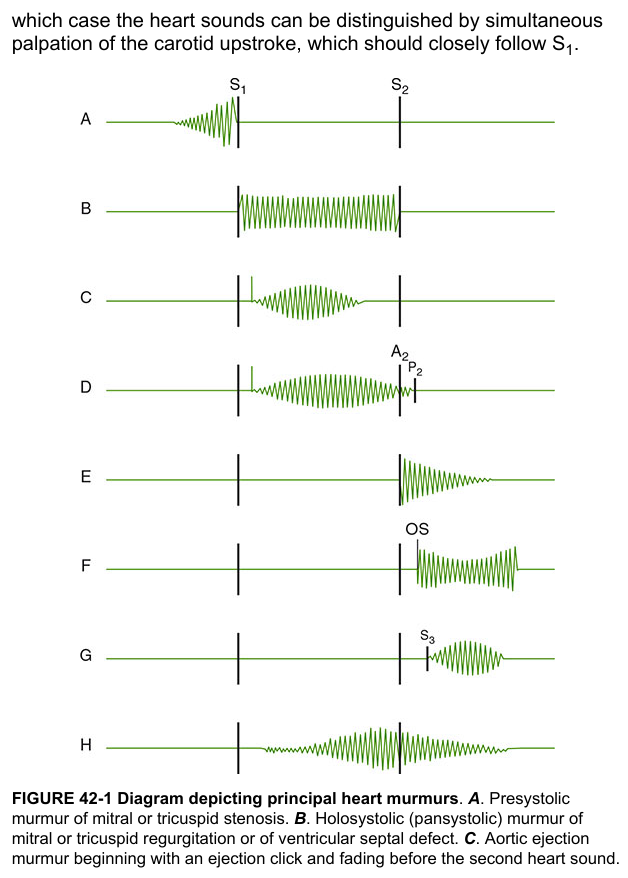
Murmurs are classified by when they occur:
1. Systolic Murmurs
Heard during the heartbeat (between lub and dub).
| Type | When it occurs | Classic Cause |
|---|---|---|
| Mid-systolic (ejection) | Peaks in mid-systole; crescendo-decrescendo shape | Aortic stenosis, pulmonic stenosis |
| Holosystolic (pansystolic) | Entire systole, same intensity throughout | Mitral regurgitation, tricuspid regurgitation, VSD |
| Late systolic | Starts mid-systole and continues to S2 | Mitral valve prolapse |
2. Diastolic Murmurs
Heard between heartbeats (between dub and next lub). Always pathological.
| Type | Classic Cause |
|---|---|
| Early diastolic (high-pitched, blowing, decrescendo) | Aortic regurgitation, pulmonary regurgitation |
| Mid-diastolic (low rumble) | Mitral stenosis, tricuspid stenosis |
| Presystolic (crescendo just before S1) | Mitral stenosis (in sinus rhythm) |
3. Continuous Murmurs
Start in systole and continue through S2 into diastole — never stops. Classic cause: Patent Ductus Arteriosus (PDA) — described as a "machinery murmur."
Grading — How Loud Is It?
Murmurs are graded on a scale of 1 to 6:
| Grade | Description |
|---|---|
| 1/6 | Very faint — barely audible, only in a quiet room |
| 2/6 | Soft but clearly heard |
| 3/6 | Moderate, no thrill (vibration on chest wall) |
| 4/6 | Loud + thrill present |
| 5/6 | Very loud, heard with stethoscope barely on chest |
| 6/6 | Heard without a stethoscope |
Grades 1–2 are usually innocent. Grades ≥3 warrant further investigation.
Key Murmurs You Should Know
Aortic Stenosis (AS)
- Type: Mid-systolic ejection murmur
- Sound: Harsh, crescendo-decrescendo
- Location: Right upper sternal border (2nd intercostal space)
- Radiates to: Neck (carotid arteries)
- Cause: Stiffened/calcified aortic valve; blood can't flow out easily
- Associated: Weak, slow-rising carotid pulse ("pulsus parvus et tardus")
Mitral Regurgitation (MR)
- Type: Holosystolic (pansystolic)
- Sound: Blowing, uniform intensity throughout systole
- Location: Apex (left side of chest)
- Radiates to: Axilla (armpit)
- Cause: Leaky mitral valve; blood jets backward into left atrium
Mitral Stenosis (MS)
- Type: Mid-diastolic rumble
- Sound: Low-pitched, rumbling, follows an "opening snap"
- Location: Apex, best heard with the bell of the stethoscope with the patient in left lateral decubitus
- Cause: Narrowed mitral valve (often from rheumatic fever); blood can't flow from left atrium to left ventricle
Aortic Regurgitation (AR)
- Type: Early diastolic
- Sound: High-pitched, blowing, decrescendo
- Location: Left sternal border, 3rd/4th intercostal space
- Cause: Leaky aortic valve; blood leaks back from aorta into left ventricle during diastole
Mitral Valve Prolapse (MVP)
- Type: Mid-to-late systolic murmur preceded by a click
- Trick: Standing/Valsalva → click moves earlier, murmur lengthens; squatting → click moves later, murmur shortens
Patent Ductus Arteriosus (PDA)
- Type: Continuous "machinery" murmur
- Location: Left upper sternal border/infraclavicular area
- Cause: A fetal blood vessel (ductus arteriosus) fails to close after birth
Murmur Patterns at a Glance
Bedside Maneuvers That Change Murmur Intensity
These tricks help doctors identify the cause:
| Maneuver | Effect on blood volume | What increases |
|---|---|---|
| Valsalva (bearing down) | ↓ venous return | HOCM, MVP |
| Standing | ↓ preload | HOCM, MVP |
| Squatting | ↑ preload & afterload | AS, MR, AR (most others louder) |
| Inspiration | ↑ right-sided flow | Right-sided murmurs (tricuspid, pulmonic) |
| Expiration | ↑ left-sided flow | Left-sided murmurs (mitral, aortic) |
When to Get Further Tests
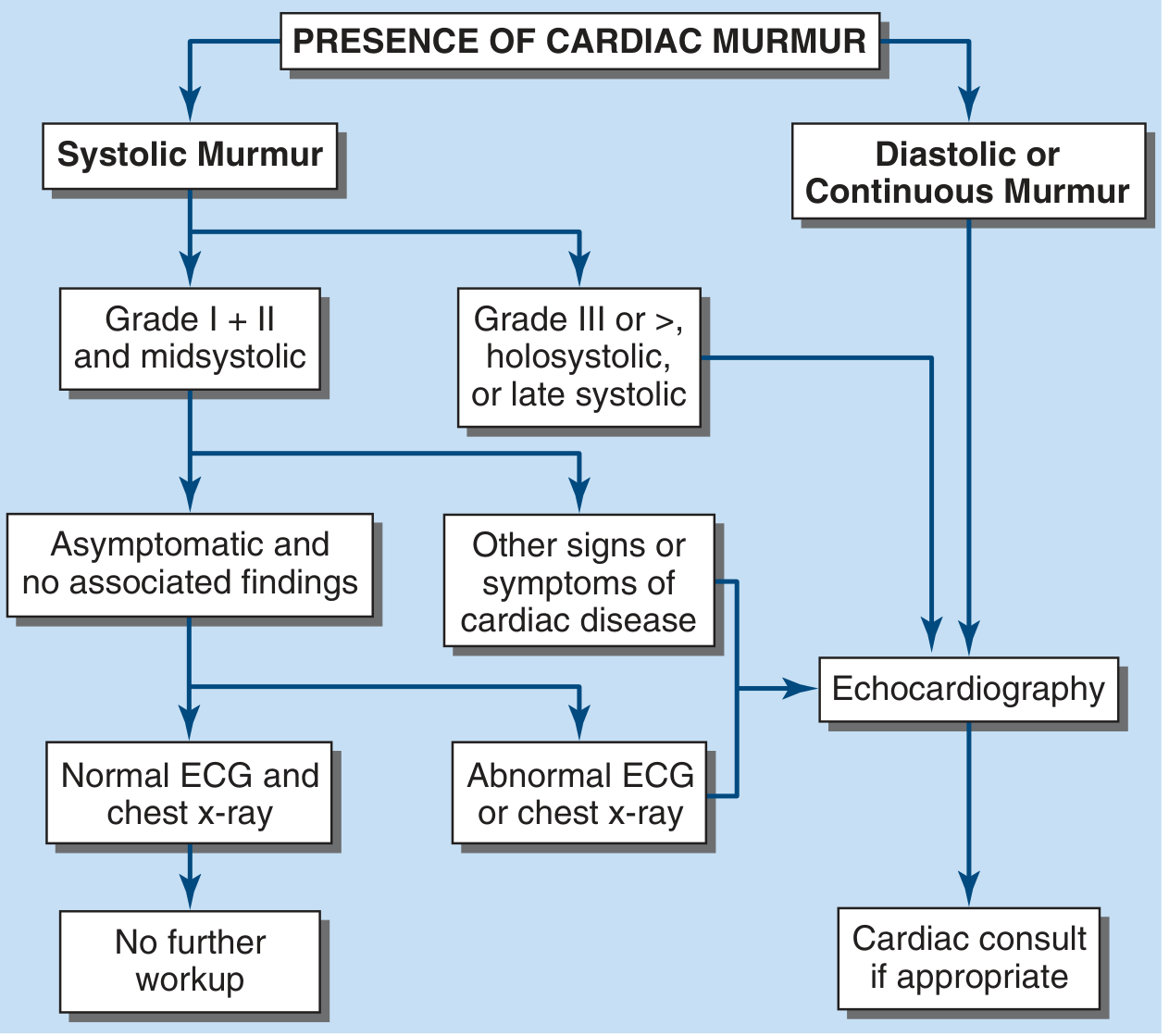
The key decision points:
- Soft systolic murmur + no symptoms + normal ECG/CXR → No further workup needed
- Loud systolic (≥3/6), holosystolic, or diastolic/continuous → Echocardiogram (ultrasound of the heart)
- Echocardiography confirms valve anatomy, measures pressure gradients, and quantifies regurgitation
Summary Table
| Feature | Innocent | Pathological |
|---|---|---|
| Grade | 1–2/6 | ≥3/6 (often) |
| Timing | Mid-systolic | Diastolic, holosystolic, or late systolic |
| Quality | Soft, musical | Harsh, blowing, rumbling |
| Symptoms | None | Dyspnea, chest pain, syncope |
| Treatment | None needed | Treat underlying cause |
Sources: Harrison's Principles of Internal Medicine, 22nd Ed. (2025); The Harriet Lane Handbook, 23rd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.