widomakers artery
Reading File
Finding Sources
Searching the Web
widow maker artery left anterior descending coronary anatomy clinical significance
Reading File
Finding Sources
Searching Images
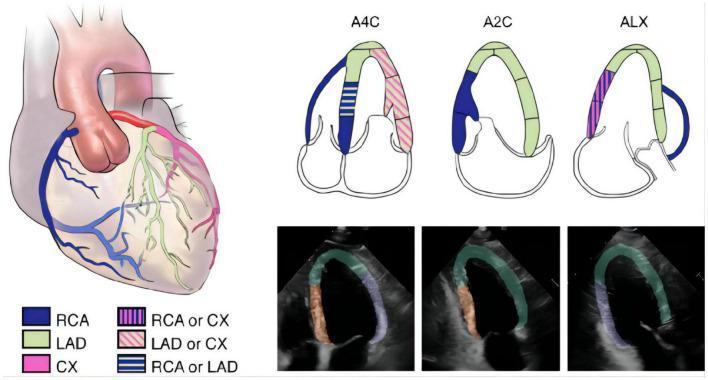
left anterior descending coronary artery anatomy diagram
Loading Image
Loading Image
I have comprehensive information to provide a thorough answer. Here it is:
The "Widowmaker" Artery — Left Anterior Descending (LAD) Artery
What Is It?
The widowmaker is the colloquial name for the left anterior descending (LAD) coronary artery — the largest and most clinically critical of the three major coronary arteries. The nickname comes from the high lethality of its sudden occlusion.
Anatomy
- Origin: Arises from the left main coronary artery (left coronary sinus of the aorta), along with the left circumflex (LCx) artery. In ~0.4% of people, the LAD and LCx have separate ostia.
- Course: Runs in the anterior interventricular groove (anterior interventricular sulcus), descending toward the apex of the heart. It typically wraps around the apex onto the inferior surface.
- Key branches:
- Septal perforators — supply the anterior 2/3 of the interventricular septum (~90% of hearts), including the bundle branches of the conducting system
- Diagonal branches — supply the anterolateral wall of the left ventricle
- Territory supplied (~50% of total cardiac output territory):
- Anterior and apical walls of the left ventricle
- Anterolateral wall
- Anterior 2/3 of the interventricular septum
- Right and left bundle branches
- Anterior papillary muscle of the mitral valve
Harrison's Principles of Internal Medicine 22E — The LAD and LCx arise from the left main; ~85% of individuals are right dominant (the RCA supplies the posterior descending artery and AV node branch). A ramus intermedius branch from the left main is a normal variant.
Why It's the Widowmaker
The LAD is the most commonly occluded coronary artery. When the proximal LAD is suddenly blocked:
- Massive myocardial territory is lost — ~50% of the heart's blood supply is cut off
- Septal perforators are occluded → the bundle branches infract → left or right bundle branch block can develop
- Anterior papillary muscle ischemia → acute mitral regurgitation
- Risk of ventricular tachycardia / ventricular fibrillation — the mechanism of sudden death
- Cardiogenic shock from acute LV failure
The result is an anterior STEMI (ST-elevation in V1–V4 on ECG). Proximal LAD occlusion produces wider, deeper ST changes than distal occlusion, affecting more leads and carrying worse prognosis.
Tintinalli's Emergency Medicine lists proximal LAD occlusion among the highest-risk features: impaired ejection fraction, extensive infarct, multivessel disease.
Cause
Occlusion is almost always due to atherosclerotic plaque rupture followed by acute thrombus formation — a process called coronary artery disease (CAD). Less commonly, spontaneous coronary artery dissection (SCAD) or coronary spasm can cause occlusion.
Myocardial bridging — where a segment of the LAD dips intramyocardially — can mimic stenosis on angiography but characteristically normalizes in diastole.
ECG Hallmarks of Proximal LAD Occlusion
| Finding | Leads |
|---|---|
| ST elevation (anterior STEMI) | V1–V4 (often V1–V6) |
| New LBBB | Diffuse |
| ST depression (reciprocal) | Inferior leads (II, III, aVF) |
| De Winter T-waves (proximal LAD) | V1–V6 (hyperacute variant without classic elevation) |
Treatment
A widowmaker heart attack is a time-critical emergency — "door-to-balloon" time matters enormously:
- Primary PCI (percutaneous coronary intervention) — emergent catheterization, balloon angioplasty, and stent placement to restore flow. Goal: <90 minutes from first medical contact.
- Fibrinolysis — if PCI is unavailable within 120 minutes
- Coronary artery bypass grafting (CABG) — for select multivessel or left main disease
- Post-MI: dual antiplatelet therapy, ACE inhibitor, beta-blocker, statin, cardiac rehab
Key Clinical Points
- Despite the name, widowmaker MI strikes women too — it is a leading cause of death in both sexes
- Proximal LAD occlusion is far worse than distal (more myocardium at risk)
- The LAD is the most common site of myocardial bridging — a normal variant where the vessel tunnels through muscle
- Coronary dominance (~85% right dominant) does not change the LAD's territory
- Immediate recognition and reperfusion is the only thing that changes outcomes
does coronary artery is direct branch of aorta
Yes — the coronary arteries are direct branches of the aorta, specifically arising from the ascending aorta at the very beginning of the aortic root.
How They Arise
The aortic root has three outpouchings called the sinuses of Valsalva (aortic sinuses):
| Sinus | Vessel Arising |
|---|---|
| Left aortic sinus (left coronary sinus) | Left main coronary artery → LAD + LCx |
| Right aortic sinus (right coronary sinus) | Right coronary artery (RCA) |
| Posterior aortic sinus (non-coronary sinus) | Nothing (no coronary artery) |
The ostia (openings) of the coronary arteries sit just above the aortic valve leaflets, at the level of the sinotubular junction. This is the very first place blood goes after leaving the left ventricle — which is why the coronaries receive well-oxygenated blood directly.
Why This Position Matters Clinically
- Aortic stenosis → elevated LV afterload + reduced aortic root pressure → decreased coronary perfusion → angina even without obstructive CAD
- Aortic dissection (Type A) can extend retrograde into the coronary ostia → acute MI
- Aortic root aneurysm / Marfan syndrome can distort coronary ostia
- Coronary angiography works by threading a catheter into the aortic root and selectively cannulating each coronary ostium
- Coronary perfusion occurs mainly in diastole — when the aortic valve is closed and the sinuses of Valsalva fill with blood, directing it into the coronary ostia
Summary
The coronary arteries are the first branches of the aorta — arising from the aortic sinuses at the root of the ascending aorta, immediately above the aortic valve.
No other major artery branches off before them. This makes them unique: they supply the very organ (the heart) that pumps blood into the aorta in the first place.
send diagram of its origin
Searching Images
coronary artery origin aortic sinus of Valsalva aortic root diagram
Loading Image
Finding Sources
Here is the diagram:
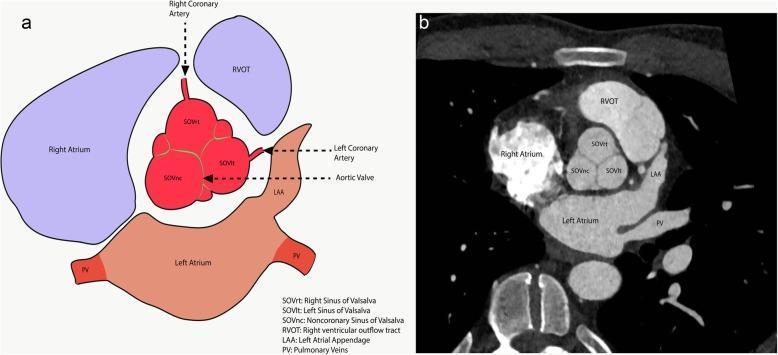
What the diagram shows (panel a — anatomical illustration, panel b — CT angiography cross-section):
-
The aortic root (red central structure) has three sinuses of Valsalva:
- SOVrt (Right Sinus) → gives rise to the Right Coronary Artery (RCA) — shown arising superiorly
- SOVlt (Left Sinus) → gives rise to the Left Coronary Artery (LCA/left main) — shown arising to the right
- SOVnc (Non-coronary Sinus) → no coronary artery arises here
-
The aortic valve sits just below these sinuses — the coronary ostia are located right above the valve leaflets
-
Surrounding structures: Right Atrium (lateral to SOVrt), Left Atrium (posterior), RVOT (Right Ventricular Outflow Tract, anterior), Left Atrial Appendage (LAA), and Pulmonary Veins (PV)
So yes — the coronary arteries open directly into the aorta from these sinuses, making them the very first branches the aorta gives off.
This is a shared conversation. Sign in to Orris to start your own chat.