Hypersensitivity reactions - classify, Type III* hypersensitivity - describe 2. Hypersensitivity - define*, Type IV hypersensitivity - describe 3. Anaphylaxis - briefly describe LAQ 1. Hypersensitivity - define**, three types of Immediate Hypersensitivity reactions with examples 2. Type I hypersensitivity - describe 3. Hypersensitivity - classify, pathogenesis, Type IV hypersensitivity 2 MBBS REFER APURB SHASTRI MUHS EXAM ORITNTED detail answer of questions colour diagrams as well for exam important points for muhs exam cover all
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Here is the complete, MUHS 2nd MBBS exam-oriented answer covering all your questions. Diagrams from Roitt's Essential Immunology (13th Ed.) and Jawetz Medical Microbiology (28th Ed.) are included.
HYPERSENSITIVITY REACTIONS - COMPLETE 2nd MBBS ANSWER
(MUHS Exam Oriented | Apurba Shastri Pattern)
⭐ DEFINITION OF HYPERSENSITIVITY (***)
Hypersensitivity is a condition in which an exaggerated or augmented immune response occurs that is harmful to the host. It requires a presensitized (sensitized) state - reactions typically occur after the second encounter with a specific antigen (allergen).
"Hypersensitivity responses lead to tissue damage: immunopathology. The mechanisms underlying hypersensitivity reactions are the same as those normally employed by the body in combating infection - the problem is that they are occurring with much too high intensity, directed against antigens that pose no threat, and/or at inappropriate locations." - Roitt's Essential Immunology, 13th Ed.
Key points for exam:
- Requires prior sensitization
- Exaggerated immune response
- Causes tissue damage (immunopathology)
- Can be antibody-mediated or cell-mediated
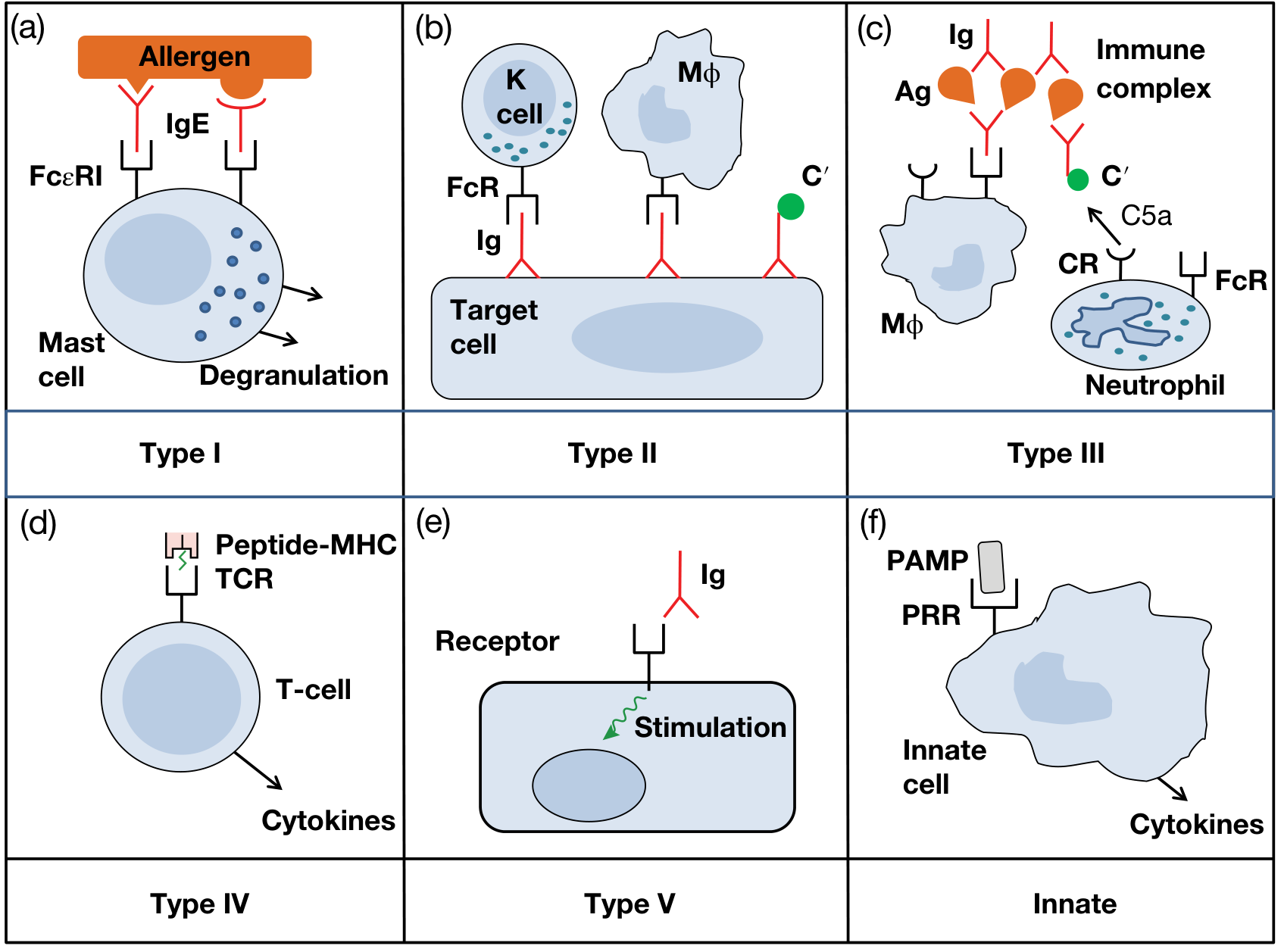
⭐⭐ CLASSIFICATION OF HYPERSENSITIVITY (Gell and Coombs, 1963)
In 1963, Coombs and Gell classified hypersensitivity into four types:
| Type | Name | Mediator | Onset | Mechanism |
|---|---|---|---|---|
| Type I | Immediate / Anaphylactic | IgE | Seconds - minutes | IgE on mast cells → degranulation |
| Type II | Cytotoxic / Antibody-mediated | IgG, IgM | Hours | Antibody to cell surface → complement/ADCC |
| Type III | Immune Complex | IgG, IgM | 3-8 hours | Immune complex deposition → complement |
| Type IV | Delayed Type / Cell-mediated (DTH) | T cells | 24-72 hours | Sensitized T cells → cytokines → macrophages |
Memory Aid: "IgE Cytotoxic Complexes Delay" = Immediate, Cytotoxic, Complex, Delayed
Types I, II, III = Antibody mediated | Type IV = Cell mediated
A Type V (stimulatory hypersensitivity) is sometimes added - antibodies stimulate receptors (e.g. Graves' disease).
⭐⭐⭐ TYPE I HYPERSENSITIVITY (Immediate / Anaphylactic)
Definition
Type I reactions manifest within seconds to minutes after antigen combines with specific IgE antibody on mast cells/basophils.
Mechanism (Step-by-step - MUHS Favorite)
STEP 1: Sensitization Phase (First Exposure)
- Antigen (allergen) enters the body
- Processed by APCs → presented to Th2 cells
- Th2 cells release IL-4 and IL-13 → B cells switch to produce IgE
- IgE binds via its Fc portion to high-affinity FcεRI receptors on mast cells and basophils
- Person is now "sensitized" - no symptoms yet
STEP 2: Elicitation Phase (Second Exposure)
- Same allergen enters again
- Allergen cross-links two or more IgE molecules on mast cell surface
- This cross-linking triggers mast cell degranulation
STEP 3: Release of Mediators
Preformed (Primary) Mediators - Released immediately:
| Mediator | Effect |
|---|---|
| Histamine | Vasodilation, increased capillary permeability, bronchospasm |
| Tryptase, Chymase | Tissue damage, matrix breakdown |
| Heparin | Anticoagulant |
| Eosinophil Chemotactic Factor (ECF-A) | Attracts eosinophils |
| Neutrophil Chemotactic Factor (NCF-A) | Attracts neutrophils |
Newly Formed (Secondary) Mediators - Synthesized from arachidonic acid:
| Mediator | Effect |
|---|---|
| Leukotrienes C4, D4 (= SRS-A) | Bronchoconstriction, increased vascular permeability (1000x more potent than histamine) |
| Leukotriene B4 | Chemotaxis of neutrophils and eosinophils |
| Prostaglandins (PGD2) | Bronchoconstriction, vasodilation, edema |
| PAF (Platelet Activating Factor) | Platelet aggregation, bronchoconstriction |
| Cytokines (TNF-α, IL-4, IL-5) | Inflammation, eosinophil activation |
Clinical Manifestations
Systemic (Anaphylaxis):
- Bronchospasm, urticaria, hypotension, angioedema
- Life-threatening
Local (Atopy):
- Hay fever (Allergic rhinitis) - pollens
- Bronchial asthma - house dust mites, animal dander
- Atopic dermatitis (Eczema)
- Urticaria (hives)
- Food allergy - peanuts, shellfish
Atopy = Familial predisposition to type I reactions, associated with elevated IgE levels. Strong genetic component.
Diagnosis
- Skin prick test (wheal and flare reaction - maximal at 30 minutes)
- Serum total IgE (elevated)
- RAST (radioallergosorbent test) / ELISA for specific IgE
- Blood eosinophilia
Treatment
- Epinephrine (first line for anaphylaxis)
- Antihistamines (H1 blockers)
- Corticosteroids (for late phase)
- Bronchodilators (salbutamol)
- Desensitization / Allergen immunotherapy (repeated small doses)
- Omalizumab - anti-IgE monoclonal antibody (for severe asthma)
THREE TYPES OF IMMEDIATE HYPERSENSITIVITY WITH EXAMPLES (LAQ)
The term "immediate hypersensitivity" broadly refers to Type I, but the three clinical forms are:
| Form | Mechanism | Examples |
|---|---|---|
| 1. Anaphylaxis (Systemic) | Systemic mast cell/basophil degranulation | Penicillin injection, bee sting, IV contrast dye |
| 2. Atopy (Local) | Local IgE-mediated reactions | Hay fever, asthma, eczema, food allergy |
| 3. Wheal and Flare (Skin) | Local intradermal antigen injection | Positive allergy skin test |
⭐⭐ TYPE II HYPERSENSITIVITY (Cytotoxic / Antibody-dependent)
Mechanism
- IgG or IgM antibodies bind to cell surface antigens or extracellular matrix antigens
- This leads to cell destruction by:
- Complement activation → MAC (membrane attack complex) → cell lysis
- ADCC (Antibody-Dependent Cell-mediated Cytotoxicity) via NK cells (K cells)
- Opsonization → phagocytosis by macrophages
- Antibody-mediated cellular dysfunction (without cell death) - e.g. Graves' disease
Examples
| Disease | Target Antigen | Effect |
|---|---|---|
| ABO transfusion reaction | RBC surface antigens | Complement-mediated lysis |
| Rh hemolytic disease of newborn | Rh(D) antigen on fetal RBCs | IgG-mediated hemolysis |
| Autoimmune hemolytic anemia | RBC antigens | Hemolysis |
| Myasthenia gravis | Acetylcholine receptor | Receptor blockade (weakness) |
| Goodpasture syndrome | Type IV collagen (GBM + lung BM) | Nephritis + pulmonary hemorrhage |
| Graves' disease | TSH receptor | Stimulation → hyperthyroidism (Type V) |
| Pemphigus vulgaris | Desmoglein 1 & 3 (desmosome) | Skin blistering |
⭐⭐⭐ TYPE III HYPERSENSITIVITY (Immune Complex Mediated)
Definition
Type III hypersensitivity is caused by the deposition of soluble antigen-antibody (immune) complexes in tissues, leading to complement activation and subsequent inflammation.
Mechanism (Pathogenesis)
STEP 1: Immune Complex Formation
- IgG (or IgM) antibodies combine with circulating soluble antigens → form immune complexes
- Normally, immune complexes are rapidly cleared by:
- C3b attachment → erythrocyte CR1 receptor → liver/spleen macrophages for destruction
- If this system is overloaded or defective → complexes persist
STEP 2: Immune Complex Deposition
- Complexes deposit in:
- Kidneys (glomeruli)
- Joints (synovium)
- Blood vessel walls
- Skin
- Choroid plexus
- Deposition is favored by:
- Antigen excess (soluble complexes form)
- Increased vascular permeability
- Anatomical filtration sites (glomeruli)
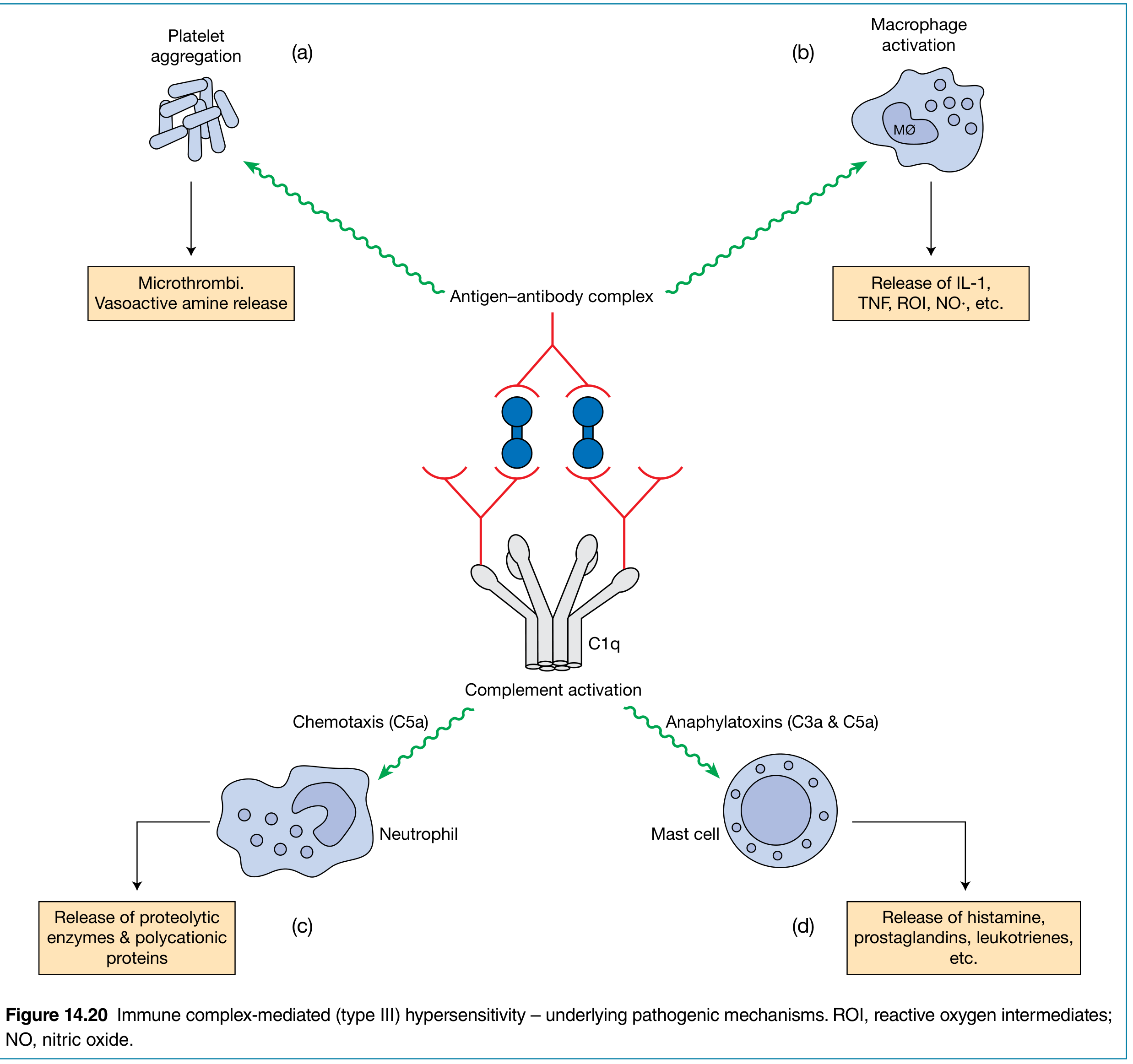
STEP 3: Complement Activation and Inflammation
- Immune complexes activate complement (Classical pathway via C1q)
- C5a → chemotaxis of neutrophils (the key cells in Type III)
- C3a, C5a (anaphylatoxins) → mast cell degranulation → histamine release → increased vascular permeability
- Neutrophils attempt to phagocytose complexes → release lysosomal enzymes and proteases → tissue damage
- Platelet aggregation → microthrombi → ischemia
- Macrophage activation → IL-1, TNF, ROI, NO release
Two Classic Forms
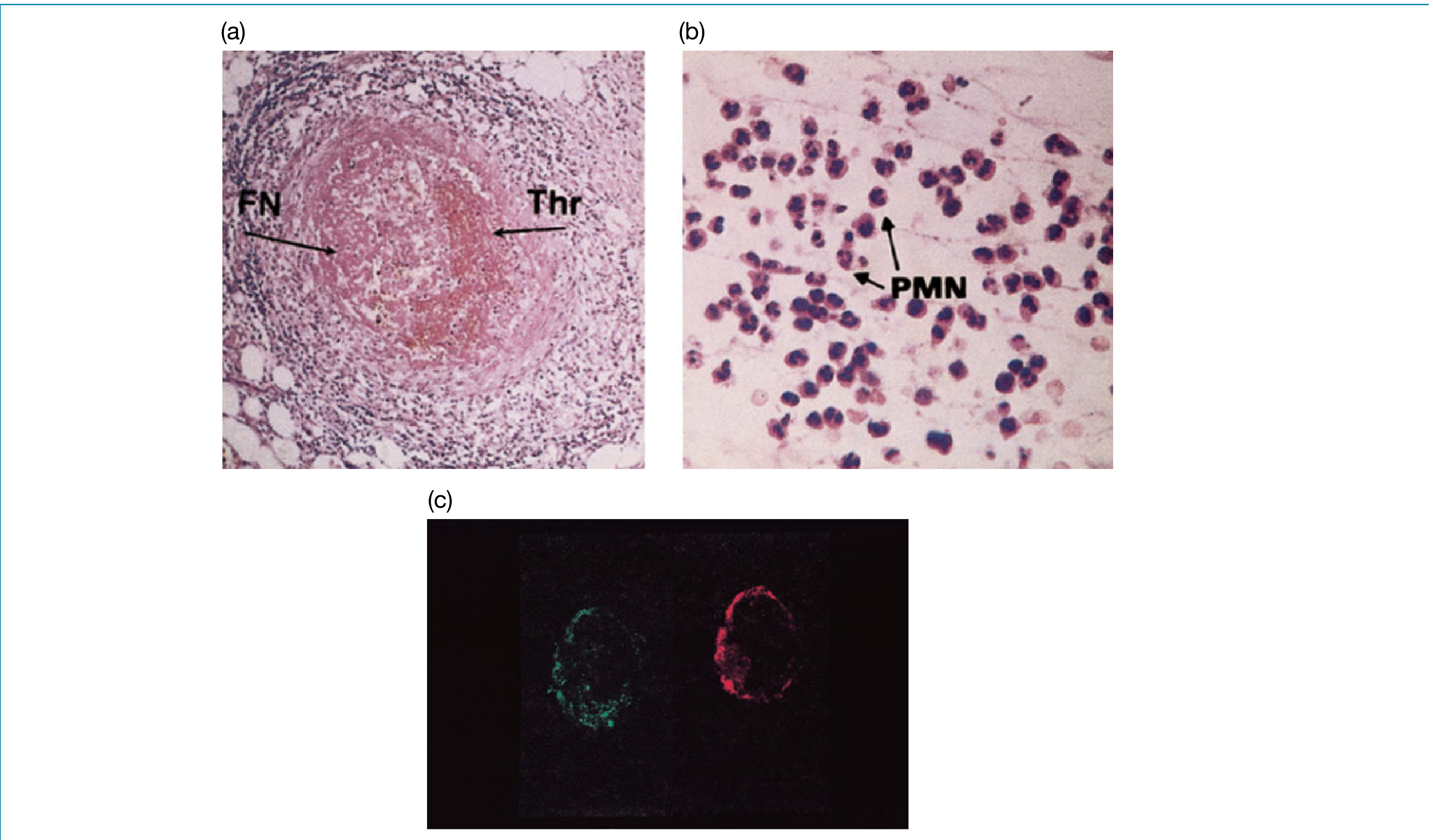
A. ARTHUS REACTION (Local Type III)
- Definition: Local immune complex reaction after intradermal injection of antigen into a hyperimmunized individual with high levels of precipitating IgG antibody
- Antigen precipitates with antibody within the venule wall → complement activation → intense neutrophil infiltration
- Peak reaction at 3-8 hours → erythema and edema → usually resolves
- Detected as: antigen + immunoglobulin + complement all demonstrable by immunofluorescence
B. SERUM SICKNESS (Systemic Type III)
- Injection of large amounts of foreign protein (e.g., heterologous serum/antitoxin)
- After 7-10 days (time needed to make antibody) → immune complexes form in antigen excess → deposit systemically
- Features: fever, urticaria, arthralgia (joint pain), lymphadenopathy, glomerulonephritis
- Self-limiting
Examples of Type III Diseases
| Disease | Antigen | Site of Deposition |
|---|---|---|
| Post-streptococcal glomerulonephritis | Streptococcal antigens | Glomerular basement membrane |
| SLE (systemic lupus) | dsDNA (nuclear antigens) | Kidney, skin, joints |
| Rheumatoid arthritis | IgG (Rheumatoid Factor = anti-IgG) | Joints |
| Serum sickness | Foreign serum proteins | Systemic - kidneys, vessels |
| Polyarteritis nodosa | Hepatitis B surface antigen | Blood vessel walls |
| Farmer's lung | Fungal spores | Lung (Type III + IV) |
| Arthus reaction | Injected antigen | Skin |
Histological/Lab Features (MUHS exam important)
- "Lumpy-bumpy" (granular) immunofluorescence pattern on GBM (vs. linear in Goodpasture syndrome - Type II)
- Low complement levels (C3, C4) - consumed by reaction
- Detection of immune complexes in serum/tissue
- Immunofluorescence: IgG + C3 deposits along GBM
⭐⭐⭐ TYPE IV HYPERSENSITIVITY (Delayed-Type / Cell-Mediated / DTH)
Definition
Type IV hypersensitivity is T-cell mediated (not antibody mediated). It is called "delayed type hypersensitivity (DTH)" because the reaction appears only after 24-72 hours of antigen contact, due to the time required for T-cell proliferation and cytokine synthesis.
Mechanism
Phase 1: Sensitization (First exposure)
- Antigen is processed by Langerhans cells / dendritic cells (APCs)
- Presented to CD4+ Th1 cells via MHC Class II
- Th1 cells become sensitized (memory T cells formed)
Phase 2: Elicitation (Second exposure, 24-72 hours)
- Antigen re-enters tissues
- Memory Th1 cells (CD4+) recognize antigen-MHC II on APCs
- T cells proliferate and release cytokines:
- IFN-γ → macrophage activation (the most important cytokine)
- IL-2 → T cell proliferation
- TNF-β (Lymphotoxin) → tissue damage
- IL-17 → neutrophil recruitment
- MCP-1 (CCL2) → monocyte chemotaxis
- Activated macrophages form the dominant effector cells → phagocytosis, tissue damage
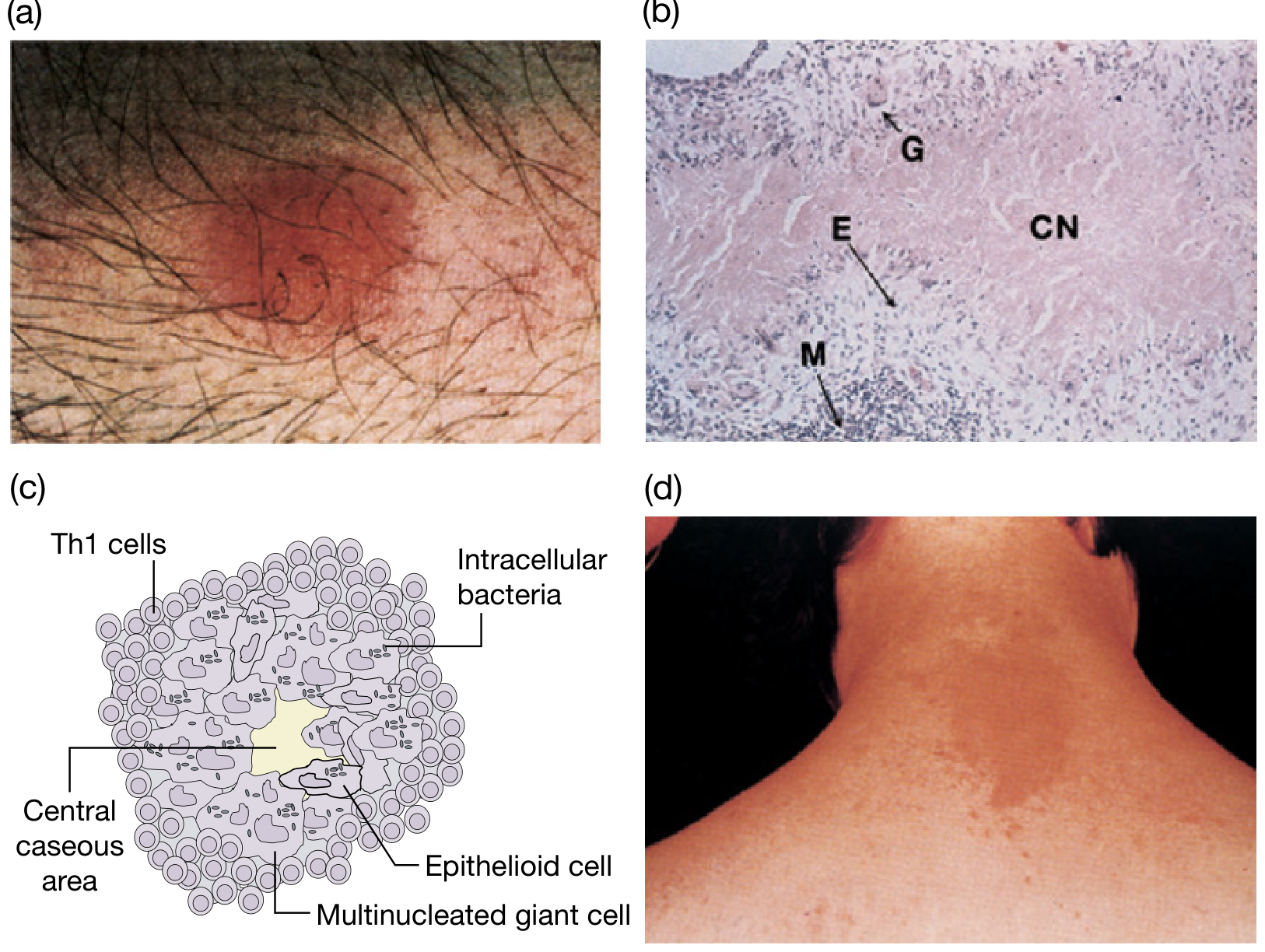
- If antigen not cleared → granuloma formation (epithelioid cells + multinucleated giant cells)
CD8+ Cytotoxic T cells also contribute - direct killing of antigen-bearing cells (important in contact dermatitis, graft rejection, virus-infected cells)
Histology (MUHS Exam Important)
- Predominantly mononuclear cell infiltrate (lymphocytes + macrophages) - contrast with Type III which has neutrophils
- Perivascular cuffing with mononuclear cells
- Granuloma: epithelioid cells, giant cells, caseous necrosis (in TB)
Classic Examples
| Clinical Example | Antigen | Features |
|---|---|---|
| Mantoux (Tuberculin) Test | PPD (tuberculoprotein) | Induration + erythema at 48-72h; maximal at 24-48h |
| Contact Dermatitis | Nickel, poison ivy, formaldehyde, topical drugs (sulfonamides) | Skin eczema 48-72h after contact |
| Transplant Rejection | Foreign MHC antigens | Graft cell destruction by CTLs |
| Tuberculosis | Mycobacterium Tb antigens | Caseous granuloma (classic Type IV) |
| Leprosy (tuberculoid) | M. leprae | Granuloma, nerve damage |
| Celiac disease | Gliadin (wheat protein) | Villous atrophy by Th1 cells |
| Type 1 Diabetes | Pancreatic beta cell antigens | Beta cell destruction by CTLs |
Mantoux Reaction: Injection of tuberculin (PPD) intradermally → Induration + erythema at 24-48 hours → characterized by perivascular mononuclear cuffing → mononuclear infiltrate (lymphocytes + macrophages). Positive = ≥10 mm induration. Negative in advanced TB, HIV, malnutrition.
Subtypes of Type IV Hypersensitivity (Advanced)
| Subtype | Key Cells | Examples |
|---|---|---|
| DTH (Classic) | CD4+ Th1 → macrophages | Tuberculin test, leprosy |
| Contact hypersensitivity | CD4+ + CD8+ | Contact dermatitis |
| Granulomatous hypersensitivity | Macrophages + Th1 | TB, sarcoidosis, schistosomiasis |
| T-cell mediated cytolysis | CD8+ CTL | Viral infections, graft rejection |
⭐ ANAPHYLAXIS (Brief Description)
Definition
Anaphylaxis is a life-threatening, acute systemic Type I hypersensitivity reaction characterized by intense constriction of bronchioles, contraction of smooth muscle, and dilatation of capillaries, occurring in a previously sensitized individual upon re-exposure to antigen.
Mechanism
- Re-exposure to antigen in a sensitized person → cross-linking of IgE on mast cells and basophils → massive systemic degranulation → release of histamine, leukotrienes, PAF, prostaglandins
- Occurs within seconds to minutes of exposure
Causes
- Injected drugs (penicillin - most common drug cause), IV contrast agents
- Insect stings (bee, wasp venom)
- Foods (peanuts, shellfish, tree nuts)
- Blood transfusion (in IgA-deficient individuals)
- Latex
Clinical Features (ABC-mnemonic)
- Airway: bronchospasm, laryngeal edema, stridor
- Breathing: dyspnea, wheeze
- Circulation: hypotension, tachycardia, cardiovascular collapse
- Skin: urticaria (hives), angioedema, flushing, pruritus
- GI: nausea, vomiting, diarrhea, abdominal cramps
Treatment (MUHS Exam - Must Know)
- Epinephrine (Adrenaline) 1:1000 - 0.3-0.5 mg IM (thigh) - FIRST AND MOST IMPORTANT
- Reverses bronchospasm (β2), vasoconstriction (α1), inhibits further mediator release
- Oxygen + airway management
- IV fluids (for hypotension)
- Antihistamines (H1 + H2 blockers - diphenhydramine + ranitidine)
- Corticosteroids (IV hydrocortisone) - for late/biphasic reactions
- Bronchodilators (salbutamol nebulization)
COMPARISON TABLE - ALL FOUR TYPES (MUHS Favorite Summary)
| Feature | Type I | Type II | Type III | Type IV |
|---|---|---|---|---|
| Name | Immediate/Anaphylactic | Cytotoxic/Antibody-dependent | Immune Complex | Delayed-Type (DTH) |
| Mediator | IgE | IgG, IgM | IgG, IgM + Complement | T cells (Th1/CTL) |
| Antigen | Soluble (exogenous) | Cell surface / BM | Soluble (circulating) | Intracellular/contact |
| Complement | No | Yes | Yes (classical pathway) | No |
| Key cells | Mast cells, Basophils, Eosinophils | NK cells, Macrophages | Neutrophils | CD4+ Th1, CD8+ CTL, Macrophages |
| Onset | Seconds-minutes | Minutes-hours | 3-8 hours | 24-72 hours |
| Transfer | Serum (IgE) | Serum (IgG) | Serum | Lymphocytes (not serum) |
| Classic example | Anaphylaxis, Hay fever | Hemolytic anemia, Transfusion rxn | Post-strep GN, SLE | Mantoux test, Contact dermatitis, TB |
| Histology | Eosinophil infiltrate | Cell lysis | Neutrophil infiltrate | Mononuclear infiltrate |
| Wheal/flare | Yes (15-30 min) | No | Erythema at 3-8h | Induration at 48-72h |
| Immunofluorescence | N/A | Linear pattern | Granular/lumpy-bumpy | N/A |
KEY EXAM POINTS FOR MUHS (⭐ Star items)
- Sensitization requires prior exposure - first exposure sensitizes, second exposure causes reaction
- Type I = IgE + Mast cells + Histamine - immediate (seconds); anaphylaxis treated with epinephrine
- Type II = IgG/IgM + complement - example: Goodpasture (linear IF), hemolytic anemia
- Type III = Immune complexes + Complement + Neutrophils - "lumpy-bumpy" IF; Arthus reaction (local), serum sickness (systemic); low complement levels
- Type IV = T cells, NO antibody, NO complement - delayed 24-72h; ONLY type transferable by lymphocytes (not serum); Mantoux test; granuloma formation
- Mantoux positive = ≥10mm induration at 48-72h
- SRS-A = Slow Reacting Substance of Anaphylaxis = Leukotrienes C4+D4+E4
- Atopy = familial predisposition to Type I; elevated total IgE
- Arthus reaction = LOCAL Type III; Serum sickness = SYSTEMIC Type III
- Omalizumab = anti-IgE monoclonal antibody - treatment for severe asthma
- Type IV granuloma: epithelioid cells + multinucleated Langhans giant cells + central caseation (TB)
Sources: Roitt's Essential Immunology, 13th Ed. (Delves, Martin, Burton, Roitt) | Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.