Caldwell luc approach and other sinus approaches
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive information from Cummings Otolaryngology and Scott-Brown's. Let me compile the full answer.
Sinus Surgical Approaches
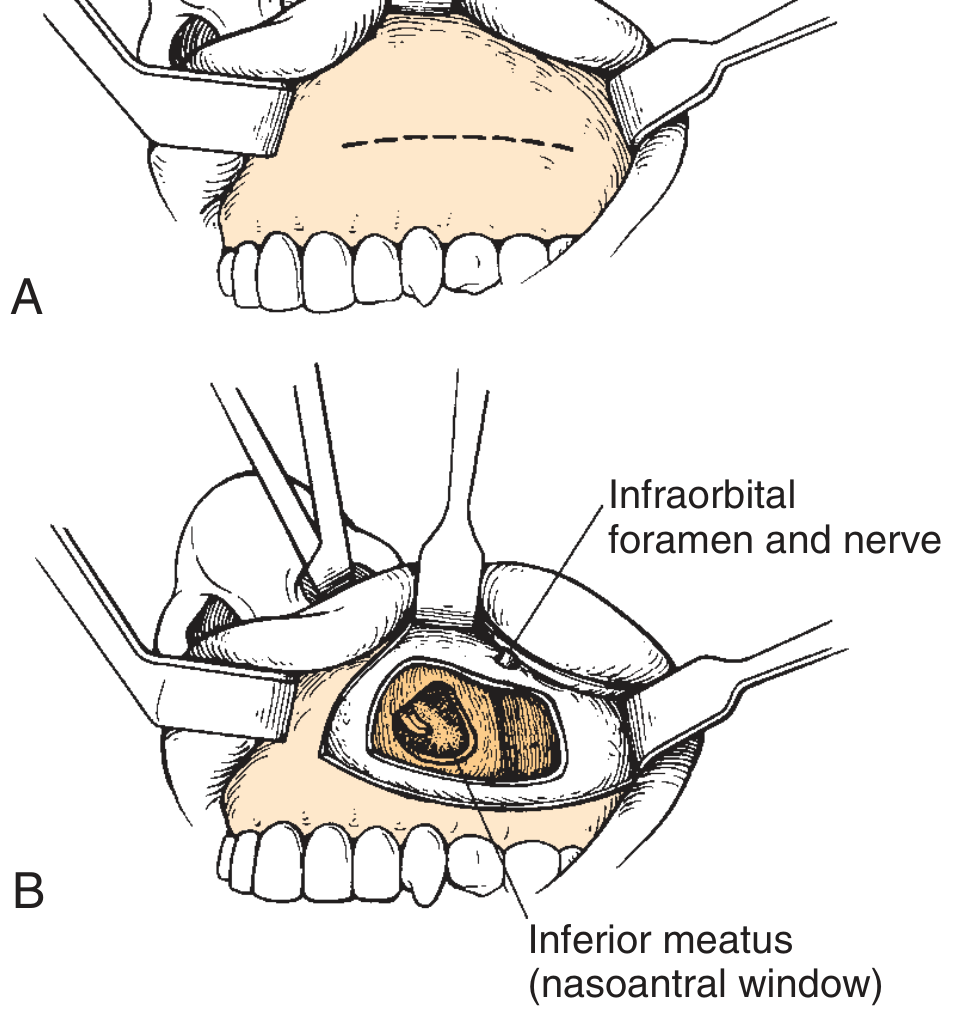
1. Caldwell-Luc Procedure (Canine Fossa Approach to the Maxillary Sinus)
History
First described by George Caldwell (1893) and Henry Luc (1897). Until the endoscope era, it was the primary approach to the maxillary sinus.
Principle
Creates an opening in the canine fossa (anterior wall of the maxillary sinus) via the gingivobuccal sulcus, combined with an intranasal antrostomy for dependent drainage.
Technique
- General anesthesia; inject gingivobuccal sulcus with 1% lidocaine + 1:100,000 epinephrine
- Incision in the gingivobuccal sulcus, above the canine fossa (in children, placed above secondary dentition using plain radiographs)
- Periosteum incised and elevated superiorly until the infraorbital nerve is identified and protected
- A 4-mm osteotome or drill outlines a window into the maxillary antrum; the anterior wall is thin and entered with gentle tapping
- Window enlarged with punch forceps or drill
- Intranasal antrostomy created by passing a curved hemostat under the inferior turbinate into the sinus - placed at least 1 cm posterior to the anterior end of the inferior turbinate (to avoid damage to the nasolacrimal duct and anterior superior alveolar nerve)
- Partial inferior turbinate removal or stenting prevents closure
- Gingivobuccal incision closed with absorbable sutures
Alternatively, commercially available canine fossa trephination sets can be used for a mini-trephine approach.
Current Indications (limited)
- Complicated acute or chronic rhinosinusitis not amenable to endoscopy
- Pterygomaxillary space surgery
- Facial trauma
- Foreign bodies
- Benign tumors (e.g., inverting papilloma in inaccessible locations)
- Canine fossa trephination: Samter's triad, allergic fungal sinusitis (removal of debris/polyps), combined with endoscopy for orbital decompression
Complications
In a review of 670 procedures, the most frequent complication was recurrent nasal obstruction (28%). Others include:
- Facial asymmetry
- Facial numbness (infraorbital/anterior superior alveolar nerve neuropraxia)
- Oroantral fistula
- Wound dehiscence
- Dacryocystitis
- Devitalized teeth
- Recurrent sinusitis / polyposis
Tip to reduce complications: Place canine fossa puncture at the intersection of the midpupillary line and a horizontal line through the floor of the nasal vestibule (Robinson and Wormald).
2. Intranasal Ethmoidectomy
- Classical open approach using a nasal speculum and headlamp (no endoscope)
- Largely replaced by endoscopic approaches
- Complication rates: 1.1-2.8%; few surgeons use it today
3. External Ethmoidectomy (Gull-Wing / Lynch Incision)
Indications
- Orbital complications of acute rhinosinusitis (subperiosteal abscess) where endoscopic visualization is limited by edema
- Access to the anterior ethmoidal artery
- Drainage of periorbital abscesses
Technique
- Temporary tarsorrhaphy on ipsilateral eye; nasal cavity decongested
- Gull-wing incision (reduces postoperative medial canthal contracture) made midway between the medial canthus and nasal midline
- Incision through periosteum; lacrimal sac elevated from its fossa
- Malleable retractor protects orbital contents
- Periosteum elevated posteriorly until anterior ethmoidal artery identified (in the frontoethmoid suture line) and ligated
- Ethmoidal complex entered through lacrimal fossa or dehiscent lamina papyracea
- Dissection guided by the basal lamella; skull base identified in posterior ethmoids
- Dissection must not go higher than the frontoethmoid suture line (skull base level)
- Periosteum formally reattached at the trochlea (non-dissolvable suture) to minimize diplopia
- Two-layer closure with external drain
Complications
Diplopia (trochlea/medial rectus injury), blindness (hematoma), exposure keratitis, corneal abrasion, skull base injury, CSF leak
4. External (Lynch-Howarth) Frontoethmoidectomy
- Historical procedure - largely replaced by endoscopic techniques
- ~1/3 of patients develop stenosis postoperatively
- Conceptually flawed: removed the bony support of the frontal recess, resulting in scarring/fibrosis obstructing the outflow tract
- Via a Lynch incision (slightly curved, halfway between nasal dorsum and medial canthus)
- Today, a Lynch incision is still used for: accessing the anterior ethmoidal artery, draining periorbital abscesses, and (if extended superolaterally) trephining the floor of the frontal sinus
5. Frontal Sinus Trephination
Acute setting
- For complicated acute frontal sinusitis not responding to medical management
- Small incision (1-1.5 cm) below medial eyebrow, through periosteum
- Drill makes a window at the junction of the floor and anterior wall of the frontal sinus
- Sinus irrigated and drain placed
Mini-trephine (chronic disease)
- Useful when the frontal sinus outflow tract is difficult to detect endoscopically
- Fluorescein-stained saline irrigation can guide frontal recess dissection
- Always aspirate before irrigating; caution if orbital dehiscence present
- Pre-op CT essential to define depth and extent of pneumatization
- Complications: intracranial penetration, CSF leak, periorbital trauma, incision infection
6. Osteoplastic Flap (With or Without Sinus Obliteration)
Indications
- Extensive osteomyelitis of the frontal sinus
- Endoscopically inaccessible tumors
- Loculated disease/post-traumatic collapse with surrounding bone loss
- Failed Draf III procedure
Technique
- Coronal flap (zigzag incision disguises scar in male-pattern baldness) or eyebrow / deep wrinkle incision
- Sterilized template of frontal sinus made from preoperative Caldwell view radiograph or 3D CT model (or guided by image-guided surgery / IGS)
- Periosteum dissected off frontal bone down to supraorbital margins
- Initial hole made into sinus in its medial third (not high in the midline - risk of venous sinus bleeding)
- Blunt-ended hook used to palpate the sinus limits; fissure burr follows the outline
- Miniplates fixed before full removal of anterior wall (for accurate replacement)
- All mucosa must be removed (including drilling the posterior wall to clear mucosa following the veins of Breschet); residual mucosa risks mucocele formation
- Sinus obliterated with fat (e.g., abdominal fat); frontal recess separated from nasal airway with fascia lata or calvarial bone pieces
- Anterior bony wall replaced and secured with miniplates
- Tight crepe bandage applied; prophylactic antibiotics given
7. Approaches to the Sphenoid Sinus
- Transseptal and transethmoid approaches
- Can be performed with headlamp or microscope, but now routinely done with endoscopic guidance
8. Endoscopic Sinus Surgery (FESS) - Reference Standard
Functional Endoscopic Sinus Surgery has replaced most open approaches for routine chronic rhinosinusitis. It preserves mucosa, restores sinus outflow tract function, and has lower complication rates. External approaches are now reserved for rare, specific situations.
Summary Table
| Approach | Target Sinus | Access | Status |
|---|---|---|---|
| Caldwell-Luc | Maxillary | Gingivobuccal sulcus | Limited indications; largely replaced by FESS |
| Intranasal ethmoidectomy | Ethmoid | Headlamp via nostril | Largely replaced by FESS |
| External ethmoidectomy | Ethmoid/Orbit | Gull-wing skin incision | For orbital complications / abscess drainage |
| Lynch-Howarth frontoethmoidectomy | Frontal/Ethmoid | Lynch skin incision | Abandoned; high stenosis rate |
| Frontal trephination | Frontal | Sub-brow incision | Acute complicated frontal sinusitis; adjunct to FESS |
| Osteoplastic flap | Frontal | Coronal/eyebrow incision | Failed FESS, osteomyelitis, inaccessible tumors |
| Transseptal/transethmoid | Sphenoid | Endonasal | Now done endoscopically |
- Cummings Otolaryngology Head and Neck Surgery, Ch. 44, pp. 897-899
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1, Ch. 99, pp. 1144-1145
When is caldwell luc preferred over fess
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
Caldwell-Luc preferred over FESS indications maxillary sinus
Here is a focused, evidence-based answer:
When is Caldwell-Luc Preferred Over FESS?
FESS is the current standard for virtually all routine maxillary sinus disease. Caldwell-Luc is reserved for specific situations where the endoscope either cannot physically reach the pathology or cannot adequately clear it.
Core Principle
The endoscope accesses the maxillary sinus primarily through the natural ostium (middle meatal antrostomy). The anterior wall, floor, and anteroinferior/lateral recesses of the maxillary sinus are the areas hardest to visualize and instrument endoscopically. When disease is located there - or when bulk/nature of disease demands complete extirpation - Caldwell-Luc provides direct anterior access that the endoscope cannot replicate.
Specific Situations Where Caldwell-Luc is Preferred (or Used as Adjunct)
1. Massive/Refractory Maxillary Polyposis or Fungal Concretions
- In severe allergic fungal sinusitis, endoscopic antrostomy alone may not allow complete removal of densely packed fungal concretions or mucin, especially from the anterior and inferior recesses
- Samter's triad (aspirin sensitivity + nasal polyposis + asthma): canine fossa trephination helps debulk polyps and debris inaccessible endoscopically
- Radiopaedia notes: "Failure to clear the maxillary mucosa completely could result in early postoperative recurrence of disease. The anterior and inferior regions of the maxillary antrum are especially difficult to access endoscopically"
2. Inverting Papilloma with Maxillary Sinus Involvement
- Inverting papillomas require complete removal at the attachment site to prevent recurrence (recurrence rates are high if any residual mucosa is left)
- When the attachment is on the anterior wall, floor, or anterolateral wall, endoscopic access is inadequate
- Caldwell-Luc combined with FESS allows direct visualization and drilling/resection of the bony attachment site
3. Orbital Decompression
- Used as an adjunct to endoscopic surgery when additional access to the orbital floor/medial wall is needed from the anterior direction
- Canine fossa trephination combined with FESS improves access and visualization
4. Pterygomaxillary Space Surgery
- Lesions of the pterygopalatine fossa or pterygomaxillary space (e.g., juvenile nasopharyngeal angiofibroma extension, schwannomas) may require the Caldwell-Luc approach for adequate access to the posterior maxillary wall
5. Trauma
- Maxillary floor (blow-out) fractures: Caldwell-Luc provides direct access to reduce and stabilize the orbital floor from below
- Foreign bodies in the maxillary sinus, particularly those lodged anteriorly or in the floor
6. Benign Tumors
- Tumors within the maxillary antrum that cannot be adequately approached endoscopically (due to size, position, or attachment)
7. Complicated Acute Rhinosinusitis
- Severe acute maxillary sinusitis not responding to antibiotics, where drainage is urgently needed and the natural ostium cannot be safely/adequately accessed
8. Failed FESS / Revision Surgery
- Scarring from prior FESS may distort anatomy, making endoscopic access to anterior recesses impossible
- Caldwell-Luc can be added to clear residual anterior disease
Caldwell-Luc vs FESS: Key Comparison
| Factor | Caldwell-Luc | FESS |
|---|---|---|
| Access | Anterior maxillary wall (direct) | Via natural ostium (middle meatus) |
| Best for | Anterior wall, floor, lateral recesses | Ostiomeatal complex, main antrum |
| Mucosa | Traditionally stripped (radical) | Preserved (mucosal sparing) |
| Reoperations | Lower in severe disease (7% vs 18-27% for FESS in heavily diseased sinuses) | Higher when used for severe disease |
| Complications | 4.4% (facial numbness, oroantral fistula, devitalized teeth) | 2.6% (lower) |
| Patient preference | Less preferred (external scar, numbness) | Strongly preferred |
| Current role | Adjunct/specific indications only | Gold standard for routine CRS |
Bottom Line
Caldwell-Luc is not a primary alternative to FESS but a targeted adjunct for:
- Anteroinferior/lateral maxillary lesions that an endoscope cannot physically reach
- Complete mucosal extirpation when bulk of disease (massive fungal, polyp disease) makes endoscopic clearance incomplete
- Structural/surgical access indications - orbital floor fractures, pterygomaxillary tumors, foreign bodies
- Inverting papilloma resection at anterior/floor attachments
In most of these settings today, it is used in combination with FESS rather than as a standalone procedure, since FESS simultaneously addresses the ostiomeatal complex for ongoing drainage.
- Cummings Otolaryngology Head and Neck Surgery, Ch. 44, p. 897
- Radiopaedia: Caldwell-Luc operation
- Medscape: Surgical Treatment of Chronic Maxillary Sinusitis
This is a shared conversation. Sign in to Orris to start your own chat.