Turp
Reading File
Finding Sources
Finding Sources
Searching PubMed
"transurethral resection of the prostate" AND "benign prostatic hyperplasia"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks. Here is a detailed overview of TURP:
Transurethral Resection of the Prostate (TURP)
Overview
TURP has long been considered the "gold standard" surgical treatment for benign prostatic hyperplasia (BPH). It involves inserting a resectoscope through the urethra and resecting or vaporizing prostatic tissue in the transition zone - the region that surrounds the prostatic urethra and is the primary site of BPH. Nodular expansion of this zone causes urethral compression and partial bladder outlet obstruction.
- Miller's Anesthesia, 10e | Smith & Tanagho General Urology, 19e | Campbell-Walsh Urology
Indications
TURP is indicated for:
- Moderate-to-severe LUTS attributed to BPH, refractory to medical therapy (the most common indication)
- Acute urinary retention (AUR) - especially recurrent or at high volume (>900 mL retained)
- Recurrent gross hematuria from prostatic origin (other causes excluded)
- Bladder calculi / diverticula with signs of end-stage bladder decompensation
- Recurrent UTIs from elevated post-void residual (after excluding bacterial prostatitis)
- Bilateral hydronephrosis with renal impairment from bladder outlet obstruction
- Campbell-Walsh Urology
Surgical Techniques
The resectoscope is inserted transurethrally. Several techniques exist:
| Technique | Description |
|---|---|
| Monopolar TURP (M-TURP) | Traditional electrocautery cutting/coagulating loop; requires non-conductive irrigant |
| Bipolar TURP (B-TURP) | Newer; allows normal saline irrigation, eliminating TUR syndrome from hyponatremia |
| HoLEP | Holmium laser enucleation of the prostate |
| Laser vaporization | Photoselective vaporization; reduced bleeding, less fluid absorption |
| Aquablation | Robotic, image-guided, high-velocity saline stream; heat-free tissue removal |
Care must be taken not to violate the prostatic capsule. If the capsule is perforated, large amounts of irrigation fluid can be absorbed into the periprostatic or retroperitoneal spaces - the procedure must be quickly terminated and hemostasis established.
- Miller's Anesthesia, 10e | Barash Clinical Anesthesia, 9e
Irrigation Solutions (Monopolar TURP)
Monopolar TURP requires a non-conductive, non-electrolytic irrigant because isotonic saline would disperse the high-frequency cutting current. The ideal fluid does not exist; commonly used solutions are:
| Solution | Osmolality (mOsm/L) | Advantages | Disadvantages |
|---|---|---|---|
| 1.5% Glycine | 200 | Widely used, less hemolysis | Transient visual disturbance, hyperammonemia, hyperoxaluria |
| 3.3% Sorbitol | 165 | Similar to glycine | Hyperglycemia, lactic acidosis, osmotic diuresis |
| 5% Mannitol | 275 | Near-isosmolar, not metabolized | Osmotic diuresis, volume expansion |
| Distilled water | 0 | Clear visualization | Massive hemolysis, hemoglobinemia, renal failure - rarely used now |
Bipolar TURP and laser techniques use isotonic normal saline, which eliminates the hyponatremia component of TUR syndrome.
- Barash Clinical Anesthesia, 9e | Miller's Anesthesia, 10e
TUR Syndrome
The most feared complication of monopolar TURP. It results from systemic absorption of large volumes of hypotonic irrigating fluid (typically >2 L) through open venous sinuses or prostatic capsule perforations.
Incidence: 0.78-1.4% (mild-moderate); complicates up to 10-15% of procedures in some series. Onset can be 15 minutes to 24 hours after the start of resection.
Pathophysiology:
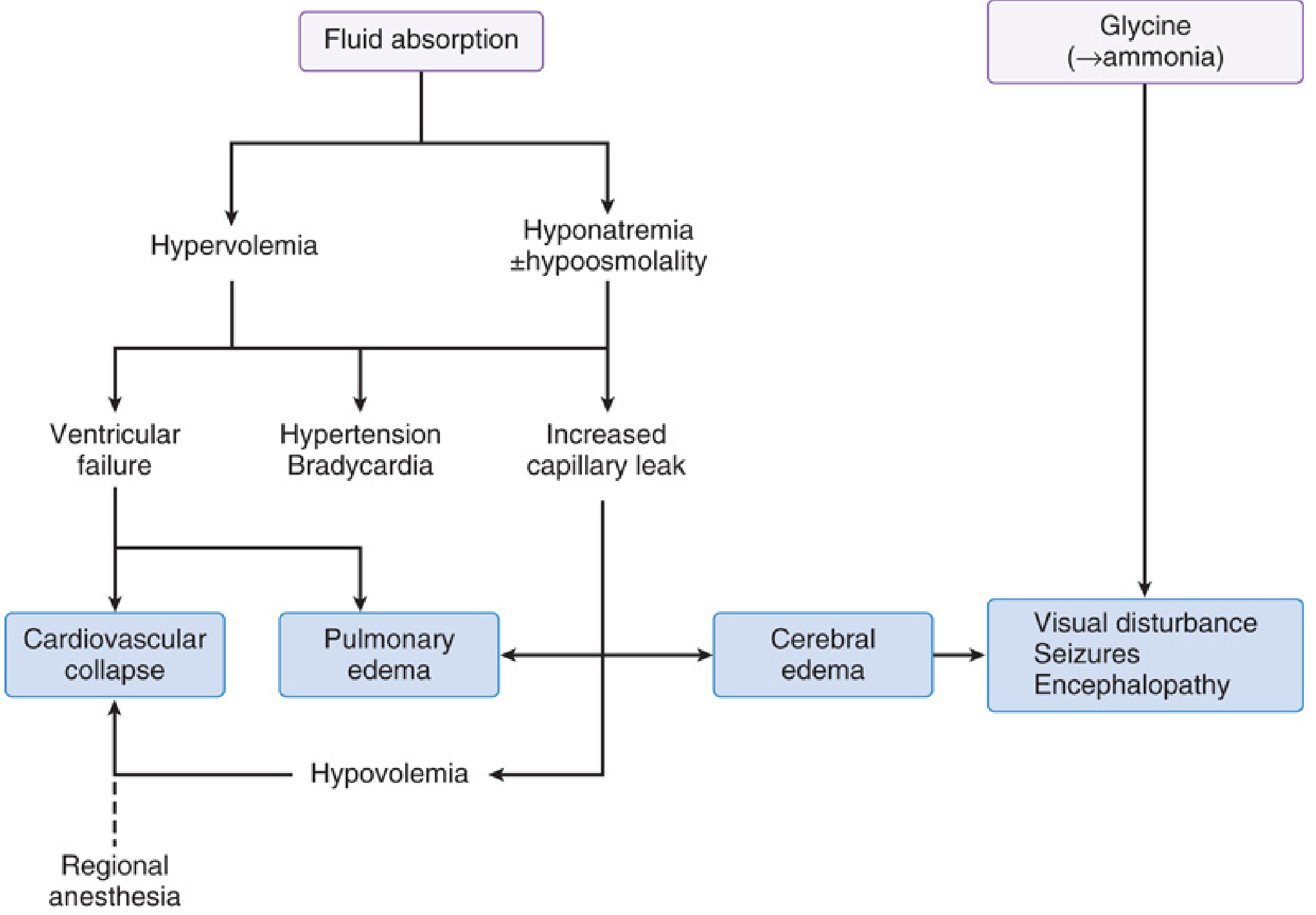
The two main drivers are:
- Hypervolemia → hypertension, bradycardia, pulmonary edema, ventricular failure, cardiovascular collapse
- Hyponatremia ± hypoosmolality → cerebral edema, seizures, encephalopathy
Glycine-specific effects: Glycine is metabolized to ammonia (hepatic deamination), causing encephalopathy lasting 24-48 hours. It also causes blurred vision or transient blindness via brainstem/cranial nerve inhibition (structural similarity to GABA), and allosteric NMDA receptor activation can cause seizures.
Mortality: Up to 25% for severe TUR syndrome (serum Na⁺ <120 mEq/L).
Risk factors:
- Increased intravesical pressure
- Prolonged resection (>90 min)
- Large gland size
- Hypotonic irrigants
- Open venous sinuses
Prevention measures:
-
Limit resection time (<90 minutes ideally)
-
Keep irrigation bag height low (minimize hydrostatic pressure)
-
Monitor serum sodium intraoperatively
-
Use bipolar/laser technique (allows saline irrigation)
-
Miller's Anesthesia, 10e | Barash Clinical Anesthesia, 9e
Complications Summary
| Complication | Incidence |
|---|---|
| Retrograde ejaculation | ~75% |
| Erectile dysfunction | 5-10% |
| Urinary incontinence | >1% |
| Bleeding requiring transfusion | ~2.5% |
| TUR syndrome (mild-moderate) | 0.78-1.4% |
| Urethral stricture / bladder neck contracture | Variable |
| 30-day mortality | 0.2-0.8% |
- Smith & Tanagho General Urology | Miller's Anesthesia, 10e
Anesthesia Considerations
Regional (spinal/neuraxial) anesthesia is preferred over general anesthesia for TURP:
- Allows early detection of TUR syndrome symptoms (agitation, confusion) in an awake patient - impossible under GA
- A large ACS-NSQIP study (2010-2016, n=28,486) showed neuraxial anesthesia associated with lower 30-day mortality, less sepsis, and fewer re-operations than GA (though UTI rate was marginally higher with neuraxial: 2.5% vs 0.9%)
- A T10 sensory block level is adequate (bladder fills at T10)
Positioning: Lithotomy with slight Trendelenburg - causes decreased pulmonary compliance, cephalad diaphragm shift, reduced FRC/TV/VC, and increased cardiac preload. Risk of common peroneal, sciatic, and femoral nerve injury.
Special patient population: TURP patients are typically elderly with multiple comorbidities. Postoperative cognitive dysfunction is a concern; one prospective study found significant cognitive decline in elderly patients at 6 hours regardless of anesthetic type, with no difference between spinal and GA at 30 days.
- Miller's Anesthesia, 10e | Barash Clinical Anesthesia, 9e
TURP vs. Alternative Surgical Options
TURP provides the greatest and most durable improvement in IPSS and urinary flow rate compared to any minimally invasive therapy, but at the cost of longer hospitalization. Newer alternatives (HoLEP, bipolar TURP, aquablation, laser vaporization) offer comparable efficacy with reduced bleeding, shorter catheterization time, and in the case of bipolar/laser, no TUR syndrome from hyponatremia.
A 2025 systematic review and meta-analysis (PMID 40348823) compared endoscopic enucleation of the prostate (EEP) vs. TURP and found EEP superior in several outcomes. A 20-year meta-analysis of TURP RCTs (PMID 39547977) provides updated evidence on long-term efficacy.
- Smith & Tanagho General Urology, 19e | Campbell-Walsh Urology
This is a shared conversation. Sign in to Orris to start your own chat.