Laryngeal electromyography and electroglottography in detail according to standard ENT textbook
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple standard ENT textbooks. Let me compile the detailed answer.
Laryngeal Electromyography (LEMG) and Electroglottography (EGG)
PART I: LARYNGEAL ELECTROMYOGRAPHY (LEMG)
Definition and Principle
Laryngeal electromyography (LEMG) measures the integrity of laryngeal innervation by means of percutaneous needle electrodes inserted into laryngeal muscles. It evaluates spontaneous and voluntary electrical activity of laryngeal muscles, thereby providing unambiguous evidence of denervation and re-innervation. Standard EMG equipment is used - no specialized laryngeal apparatus is required.
(Scott-Brown's Otorhinolaryngology Head & Neck Surgery; Cummings Otolaryngology Head and Neck Surgery)
Equipment and Setup
- Standard EMG machine with needle electrodes
- Topical anaesthetic is NOT used - it has been shown to affect the electrical signal
- The patient must be cooperative and able to phonate on command to verify needle placement
Muscles Sampled and Needle Technique
1. Thyroarytenoid (TA) Muscle - Recurrent Laryngeal Nerve (RLN)
The most commonly sampled muscle, supplied by the RLN.
Two approaches:
-
Midline transglottic approach: The needle is introduced between the thyroid and cricothyroid cartilages and directed superiorly. The needle enters the subglottic airspace in the midline, then is diverted into the right or left vocal fold. This approach frequently stimulates coughing because sensory receptors in the vocal fold mucosa are activated.
-
Off-midline cricothyroid approach (preferred): The needle enters the cricothyroid space off the midline, allowing the muscle to be entered without violating the mucosa - avoiding the cough reflex.
Verification of placement: Patient is asked to phonate - TA activation confirms correct positioning.
2. Cricothyroid (CT) Muscle - Superior Laryngeal Nerve (SLN)
- Needle is inserted in the midline, down to the superior edge of the cricoid cartilage
- The tip is "walked" over the cartilage superiorly and laterally to avoid the strap muscles
- A palpable "pop" is felt as the needle enters the CT muscle
- Verification: Patient asked to begin phonating at comfortable pitch, then glide to a higher (falsetto) pitch. The CT may be active or silent at comfortable pitch but is reliably activated at higher pitches.
Clinical Applications
1. Distinguishing Neural from Mechanical Vocal Fold Immobility
This is the most important and common application of LEMG.
- If EMG abnormalities are detected, a neural (neurogenic) lesion is confirmed
- A normal EMG supports (but does not confirm) mechanical fixation (e.g., cricoarytenoid joint fixation)
- LEMG definitively diagnoses paralysis vs. immobility - something neither laryngoscopy nor stroboscopy can achieve with certainty
2. Differentiating Vagus Nerve vs. RLN Injury
- Cricothyroid function (SLN) should be intact after an isolated RLN injury
- If CT is also denervated, a high vagal lesion is suspected
3. Prognosis in Vocal Fold Paralysis
LEMG is most useful when performed within 6 months of onset of paralysis. The literature suggests it is more reliable as a predictor of poor outcome than recovery:
| Study | N | Accurate prediction of recovery | Accurate prediction of no/impaired recovery |
|---|---|---|---|
| Munin et al. | 31 | 80% | 80% |
| Sittel et al. | 111 | 13% | 94% |
| Gupta & Bastian | 18 | 70% | 75% |
| Hirano et al. | 29 | 63% | 80% |
| Parnes & Satya-Murti | 18 | 80% | 100% |
(Table 78.3, Scott-Brown's)
Why LEMG predicts poor outcome better: Signs like fibrillation potentials and positive sharp waves indicate absence of re-innervation with no physiologic ambiguity. Re-innervation signs, by contrast, do not always translate to restored function (due to synkinesis).
4. Synkinesis
- When nerve regeneration occurs aberrantly (nerve fibers reconnecting to functionally inappropriate muscles), the vocal fold may remain immobile despite vigorous re-innervation
- Significant activation of the TA muscle with sniffing (a sign of aberrant innervation from the abductor branch) is considered a poor prognostic indicator
- Synkinesis alters prognosis in vocal fold paralysis and must be specifically identified on LEMG
5. Vocal Fold Paresis
LEMG assists in diagnosing subtle paresis, though quantification is controversial because signal amplitude varies with electrode impedance, position in muscle, and individual variation. Quantitative LEMG is an evolving technique offering more objective neurologic status assessment.
6. Neuromuscular Disease
- Myasthenia gravis: Fatigue recruitment of laryngeal/pharyngeal muscles may be detected; an edrophonium (Tensilon) test can confirm
- Motor neuron disease (ALS)
- Myopathy
EMG Findings Interpreted
| Finding | Significance |
|---|---|
| Normal insertional activity + normal voluntary motor units | Normal innervation; supports mechanical fixation if fold immobile |
| Fibrillation potentials | Denervation (appear ~3 weeks after complete nerve injury) |
| Positive sharp waves | Denervation |
| Absent voluntary activation (electrical silence) | Complete nerve section; recovery extremely unlikely |
| Polyphasic action potentials | Re-innervation (disordered nerve signals) - recovery possible but prognosis unclear |
| Synkinetic firing | Aberrant re-innervation - fold may remain immobile despite re-innervation |
When a patient shows denervation with poor motor unit recruitment, recovery is extremely unlikely and early surgical intervention is prudent.
Limitations and Controversies
- LEMG has been criticized as subjective, though this criticism applies equally to laryngoscopy and stroboscopy
- Signal quality depends heavily on electrode placement and operator skill
- Spontaneous re-innervation is common after nerve injury, and neuropathic signs can be subtle
- Polyphasic potentials indicate re-innervation potential, but the rate and functional outcome remain unpredictable
- LEMG can more reliably identify when a nerve will not recover rather than when it will
(Cummings Otolaryngology; Scott-Brown's)
PART II: ELECTROGLOTTOGRAPHY (EGG) / ELECTROLARYNGOGRAPHY (ELG)
Synonyms
Electroglottography (EGG) = Electrolaryngography (ELG/ELG) = Laryngography. The terms are interchangeable in clinical and research settings.
Principle and Physics
EGG measures the electrical conductance (or inversely, impedance) of a low-frequency electrical signal across the neck between two surface electrodes placed bilaterally over the thyroid cartilage.
The device (e.g., the Laryngograph®) applies a high-frequency current (3 megahertz) held at constant voltage across the two electrodes. Vocal fold vibration changes the electrical conductance between the electrodes:
- When the vocal folds contact each other → conductance increases → the slope of the EGG waveform trace is positive (rising limb)
- As vocal folds separate → conductance decreases → the slope is negative (falling limb)
The resulting waveform is called the Lx (laryngograph) waveform or EGG waveform.
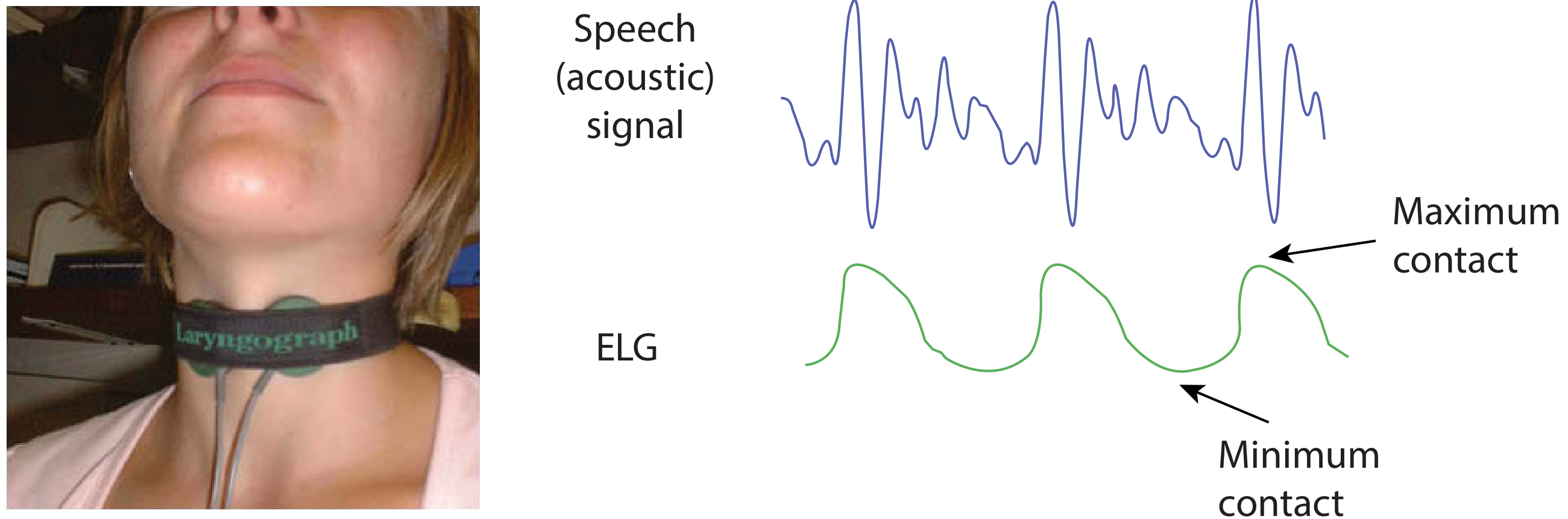
The EGG waveform (green, lower trace) shows maximum contact = peak of waveform, minimum contact = trough. In modal voice, vocal folds close more rapidly than they open, producing a sharper rise than fall. This is shown alongside the acoustic speech signal (blue, upper trace).
(Figure 62.6, Scott-Brown's)
Electrode Placement
Two electrodes placed bilaterally on the skin surface over the thyroid cartilage laminae, secured with a collar/strap around the neck. The level corresponds to the glottis.
Limitation: The technique may not work reliably when soft tissues of the neck are thick (e.g., obesity), as increased tissue impedance degrades signal quality.
What the EGG Waveform Represents
The EGG waveform shape reflects the pattern of vocal fold vibration:
- Results are relative, not absolute - the signal does not directly measure glottal area or actual degree of closure in absolute terms
- It reflects changes in vocal fold contact area during each vibratory cycle
- In modal (chest) voice: the vocal folds close more rapidly than they open, giving a sharper rise and more gradual fall in the waveform
- The waveform is unaffected by vocal tract resonances, making it particularly clean for frequency analysis
Derived Measurements and Quotients
Several quotients have been proposed to quantify the EGG waveform (though standardization is incomplete):
| Quotient | Description |
|---|---|
| Open Quotient (OQ) | Ratio of open phase to total period |
| Contact Quotient (CQ) | Ratio of closed phase to total period - reflects degree of glottal closure |
| Skewing Quotient | Ratio of increasing to decreasing slope - reflects asymmetry of open/close phases |
| Speed Quotient | Related to open/close velocity ratio |
Techniques for quantifying the waveform have not yet been standardized, largely due to technical challenges and difficulty correlating the EGG waveform to actual vocal fold motion.
Clinical Information Obtained
-
Fundamental frequency (F0 / Fx): One of the most accurate methods for measuring fundamental frequency, even in severely dysphonic voices, because the signal is unaffected by vocal tract resonances
-
Frequency perturbation (Jitter): Short-cycle-to-cycle variations in F0
-
Degree of vocal fold contact: The waveform shape gives information about the closed and open phases
-
Mean Speaking Fundamental Frequency (SFF): A 2-minute speech sample can be plotted as a frequency histogram showing the dynamic frequency range. The DFx2 histogram overlays pitch-pairs (two consecutive periods differing by no more than 10%) representing minimum consecutive periodic vibratory cycles
-
Voice quality characterization: Contributes to multidimensional voice assessment, especially when combined with laryngeal stroboscopy or other measures
Role in Multidimensional Voice Assessment
As stated in Scott-Brown's Table 62.1, electrolaryngography/EGG is one of several objective voice evaluation methods:
| Method | Basis | Examples |
|---|---|---|
| Acoustic analysis | Microphone near mouth | F0, jitter, shimmer, spectral measures |
| Electrolaryngography/EGG | Electrical conductance across neck | F0 measurement, degree of vocal fold contact, perturbation |
| Aerodynamic measures | Air volume/flow/pressure | Subglottal pressure, mean airflow rate |
| Voice accumulator | Prolonged sampling | Phonation time, frequency, intensity |
| Combined measures | Multidimensional | Dysphonia Severity Index, Cepstral Spectral Index |
No single measure fulfils all functions - a multidimensional approach is ideal.
EGG vs. Inverse Filtering
Both are techniques for estimating the voice "source" (output of vocal fold vibration and its interaction with subglottal/supraglottal pressures):
- EGG - measures conductance across the neck; non-invasive, simple, reflects contact patterns
- Inverse filtering - signal-processing technique that removes vocal tract formant effects from the acoustic/aerodynamic waveform to isolate the glottal flow waveform. Technically challenging, results difficult to validate, but provides the skewing quotient, open quotient, and spectral slope measures
Limitations of EGG
- Does not directly measure glottal area or provide absolute closure measurements
- Signal affected by thick neck soft tissues
- Waveform interpretation not fully standardized
- Cannot diagnose specific pathology on its own - must be used in context of other assessments
- Limited value in isolation; most useful as part of a multiparameter voice evaluation
Summary Comparison
| Feature | LEMG | EGG/ELG |
|---|---|---|
| Type | Invasive (percutaneous needle) | Non-invasive (surface electrodes) |
| Signal measured | Electrical activity of laryngeal muscles | Electrical conductance across glottis |
| Primary use | Innervation integrity, paralysis vs. fixation, prognosis | Fundamental frequency, vocal fold contact patterns, voice quality |
| Key finding | Fibrillation potentials, polyphasic potentials, synkinesis | Open/closed phase ratios, F0 accuracy |
| Main limitation | Operator-dependent; re-innervation ≠ function | Does not measure absolute glottal area; thick neck degrades signal |
| Best combined with | Laryngoscopy, stroboscopy | Acoustic analysis, stroboscopy, aerodynamics |
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (9th ed.), Chapter 78 (Vocal Fold Paralysis) and Chapter 62 (Objective Voice Assessment)
- Cummings Otolaryngology Head and Neck Surgery (7th ed.), Chapter 55 (Voice Evaluation) and Chapter 56 (Laryngeal Nerve Integrity Assessment)
- K.J. Lee's Essential Otolaryngology (12th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.