Mechanism of diffuse axonal injury
Reading File
Finding Sources
Searching PubMed
"diffuse axonal injury" mechanism pathophysiology
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed for a comprehensive, well-sourced answer. Here it is:
Diffuse Axonal Injury (DAI) - Mechanism
Definition and Terminology
DAI - also called traumatic axonal injury (TAI) or shear injury - is widespread disruption of axonal fibers in white matter and brainstem resulting from rapid acceleration-deceleration or rotational forces. It accounts for up to 50% of cases of post-traumatic coma that occur even without visible cerebral contusions. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Biomechanical Trigger
The initiating event is rotational angular acceleration-deceleration, not direct impact. The brain's gray matter (neurons, cortex) and white matter (axonal tracts) have different densities and move at different speeds during impact. The resulting shear strain tears axons at tissue interfaces. High-velocity road traffic accidents and blast injuries are classic causes; in infants, the same forces occur in abusive head trauma (shaken baby syndrome). - Grainger & Allison's Diagnostic Radiology; Sabiston Textbook of Surgery
Pathophysiological Cascade
DAI is now understood to be primarily a secondary biochemical injury following an initial mechanical deformation, not simply immediate axon tearing. The sequence unfolds in two phases:
Phase 1 - Primary Axotomy (Mechanical)
At the moment of injury, rapid stretching of axons causes:
- Axolemmal disruption - the axon membrane is physically breached, creating transient pores (mechanoporation)
- Ionic flux - unregulated influx of Na⁺ and Ca²⁺ into the axoplasm
- Neurofilament compaction - the cytoskeletal intermediate filaments collapse and compact
- Microtubule disassembly - Ca²⁺ influx directly destabilizes microtubules within 6-24 hours of injury
- Disruption of axoplasmic flow - anterograde and retrograde transport along the axon halts
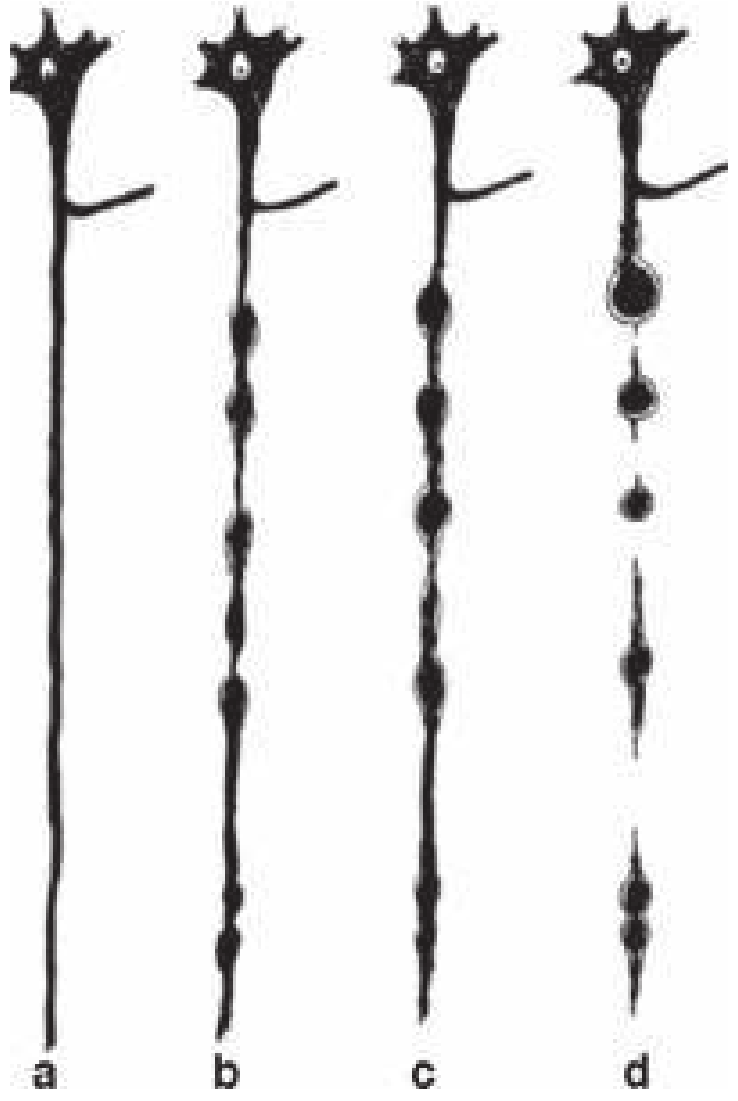
This produces the characteristic axonal swellings along the full length of the axon, evolving into retraction balls - rounded aggregates of dammed-up axoplasmic material. - Rosen's Emergency Medicine
Phase 2 - Secondary Axotomy (Biochemical, delayed 6-12 hours)
In cases that do not immediately transect, a delayed biochemical cascade completes the injury:
| Step | Event |
|---|---|
| Ca²⁺ accumulation | Activates calpains (calcium-dependent proteases) |
| Calpain activation | Degrades cytoskeletal proteins (spectrin, neurofilaments, MAP2) |
| Mitochondrial damage | Ca²⁺ overload impairs oxidative phosphorylation |
| Axonal transport failure | Proteins, organelles, and Aβ precursor protein accumulate at swelling sites |
| Complete transection | The axon disconnects; the distal segment undergoes Wallerian degeneration |
In severe cases, apoptotic pathways are also triggered, culminating in delayed neuronal cell death. - Bradley and Daroff's Neurology in Clinical Practice; Sabiston Textbook of Surgery
Neurometabolic Cascade (Concurrent)
Alongside axonal injury, a broader neurometabolic crisis unfolds:
- Neuronal membrane disruption releases glutamate, causing excitotoxicity
- Massive Na⁺/K⁺ flux activates the Na⁺/K⁺-ATPase, consuming ATP at a high rate
- Demand outstrips supply: cerebral blood flow falls ~50% while metabolic demand is elevated - a state of metabolic depression lasting days (animals) to weeks (humans)
- Ca²⁺-mediated vasoconstriction reduces CBF further, potentiating the energy crisis
- This "metabolic vulnerability window" renders the brain highly susceptible to a second injury (second impact syndrome) - Bradley and Daroff's Neurology in Clinical Practice
Grading of DAI (Adams/Gennarelli Classification)
| Grade | Location of lesions | Severity |
|---|---|---|
| I | Subcortical and deep white matter of cerebral hemispheres (gray-white junction) | Mild |
| II | Grade I + corpus callosum | Moderate |
| III | Grade II + dorsolateral rostral brainstem / cerebral peduncles / superior colliculi | Severe |
Lesions preferentially occur where density differences are greatest - the gray-white matter interface, corpus callosum (tethered centrally while hemispheres rotate), and brainstem. - Grainger & Allison's Diagnostic Radiology; Robbins
Morphological Findings
- Gross: Petechial hemorrhages in deep white matter, corpus callosum, and brainstem. May be invisible on initial CT.
- Microscopy (within 1-2 hours): Axonal swellings and retraction balls in brainstem and subcortical regions; best demonstrated with:
- Silver impregnation stains
- Immunoperoxidase stains for amyloid beta precursor protein (AβPP) or alpha-synuclein (transported proteins that accumulate at blockage sites)
- Later: Increased microglia in damaged cortex, then degeneration of involved fiber tracts (Wallerian degeneration)
Note: Visible lesions on both MRI and CT represent only the "tip of the iceberg" of actual axonal injury. - Sabiston; Robbins
Imaging Correlates
- CT: Often normal or shows only subtle punctate hyperdensities at gray-white junction / corpus callosum / brainstem. The finding of hemorrhagic foci in the corpus callosum and dorsolateral brainstem is highly suggestive.
- MRI: Far more sensitive. FLAIR and DWI show non-hemorrhagic lesions; gradient-echo (GRE) and susceptibility-weighted imaging (SWI) are the most sensitive sequences, detecting microbleeds at DAI sites. - Grainger & Allison's Diagnostic Radiology
Key Biomarkers
Elevated serum/CSF levels of these proteins reflect ongoing axonal damage:
- AβPP (accumulates at injury sites within hours)
- Neurofilament light chain (NfL) - released from disrupted axons
- GFAP and S-100β - astrocyte injury markers co-occurring with DAI
Long-Term Consequences
Persistent DAI contributes to:
- Chronic traumatic encephalopathy (CTE) - with tau and Aβ accumulation following repetitive injury
- Increased risk of Alzheimer disease - TBI-associated Aβ elevation and tau aggregation mirror AD pathology
- Cognitive impairment, personality change, and vegetative states in severe cases - Bradley and Daroff's Neurology in Clinical Practice
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease | Rosen's Emergency Medicine | Bradley and Daroff's Neurology in Clinical Practice | Sabiston Textbook of Surgery | Grainger & Allison's Diagnostic Radiology | Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.