I have my university exam of 1 st year of subject physiology These are the important long answer give me answer of this question "Describe the mechanism of secretion of insulin. Mention the functions of insulin. Add a note on Diabetes Mellitus." and remeber it's a long question
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have all the content needed for a comprehensive exam answer. Let me compile everything into a well-structured, detailed long-answer format.
Mechanism of Secretion of Insulin, Functions of Insulin, and Diabetes Mellitus
INTRODUCTION
Insulin is a polypeptide hormone secreted by the beta (B) cells of the islets of Langerhans in the pancreas. It was first isolated in 1921 by Frederick Banting and Charles Best at the University of Toronto. It is the principal anabolic hormone in the body, regulating carbohydrate, fat, and protein metabolism.
PART 1: MECHANISM OF SECRETION OF INSULIN
Structure of Insulin
Insulin is synthesized as a preprohormone. It is first cleaved to proinsulin, which is then cleaved to release the active insulin molecule (consisting of an A chain and B chain linked by disulfide bonds) and a biologically inactive C-peptide. Both insulin and C-peptide are secreted in equimolar amounts, making C-peptide a useful marker for endogenous insulin secretion.
Glucose-Stimulated Insulin Secretion (Primary Mechanism)
The primary stimulus for insulin secretion is a rise in blood glucose. The sequence of events is as follows:
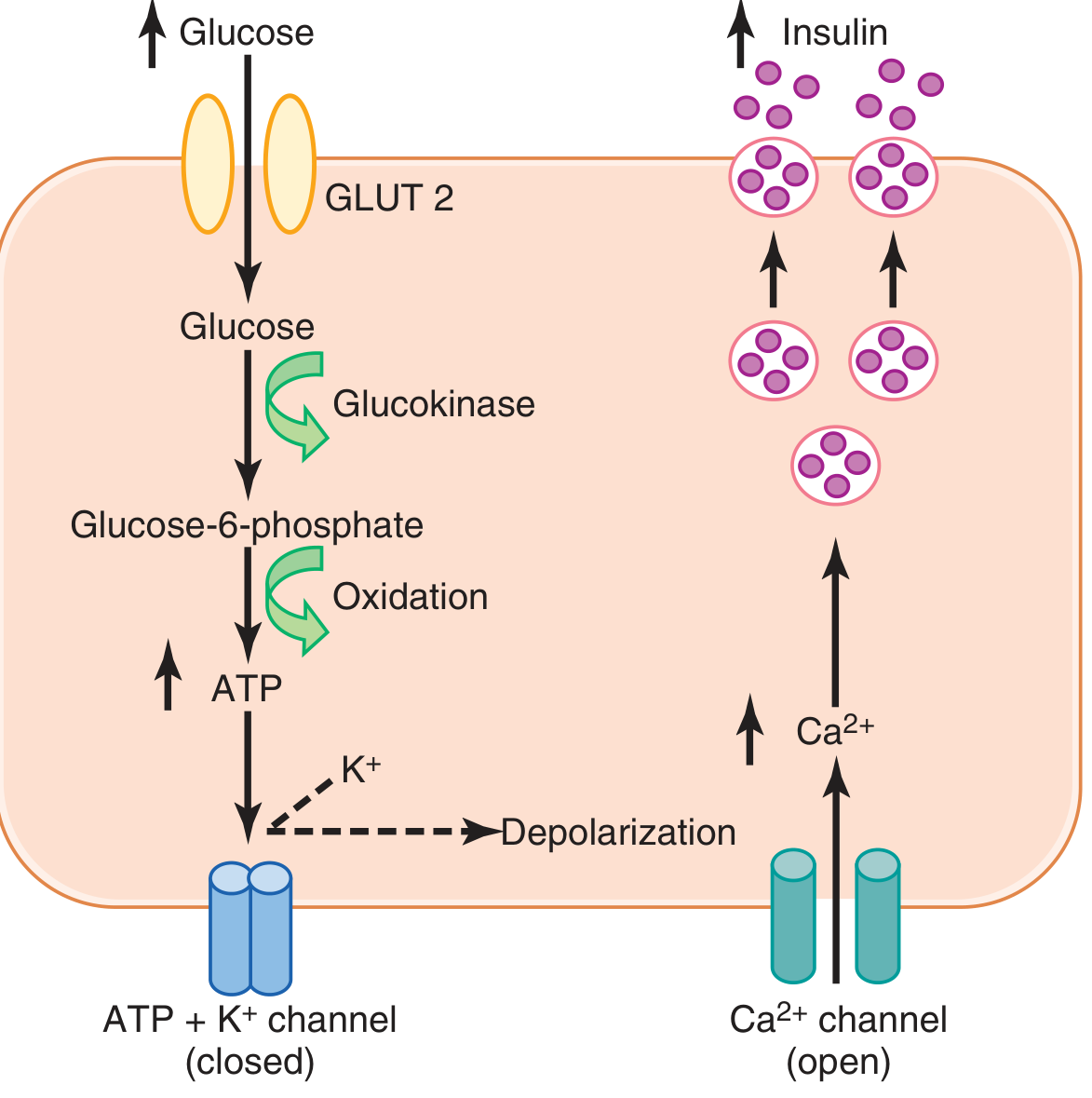
Step 1 - Glucose Entry via GLUT2
Beta cells possess a large number of GLUT2 transporters (glucose transporter type 2). These allow glucose to enter the beta cell at a rate proportional to blood glucose concentration in the physiological range.
Step 2 - Phosphorylation by Glucokinase (Glucose Sensor)
Inside the beta cell, glucose is phosphorylated to glucose-6-phosphate by the enzyme glucokinase. This phosphorylation step is rate-limiting and acts as the glucose sensor - it is the primary mechanism by which the beta cell detects and responds to changes in blood glucose.
Step 3 - ATP Production
Glucose-6-phosphate is oxidized through glycolysis and the TCA cycle, generating ATP. This raises the intracellular ATP:ADP ratio.
Step 4 - Closure of ATP-sensitive K+ Channels
Elevated intracellular ATP inhibits (closes) the ATP-sensitive potassium channels (K-ATP channels) on the beta cell membrane. Since K+ normally flows outward through these channels, their closure causes accumulation of K+ inside the cell, leading to depolarization of the membrane.
Step 5 - Opening of Voltage-Gated Ca2+ Channels
Membrane depolarization opens voltage-gated calcium (L-type Ca2+) channels, allowing a large influx of Ca2+ from the extracellular space into the beta cell. Intracellular Ca2+ rises sharply.
Step 6 - Exocytosis of Insulin
Elevated intracellular Ca2+ acts as the final trigger, causing fusion of the insulin-containing secretory vesicles (granules) with the plasma membrane and release of insulin into the extracellular fluid by exocytosis.
Biphasic Pattern of Insulin Secretion
When blood glucose suddenly rises to 2-3 times normal, insulin secretion occurs in two phases:
-
First phase (rapid): Plasma insulin rises almost 10-fold within 3-5 minutes due to immediate release of pre-formed, stored insulin from granules already docked at the cell membrane. This phase is transient and falls back halfway within 5-10 minutes.
-
Second phase (sustained): Beginning around 15 minutes, a second rise occurs over 2-3 hours, reaching even higher levels. This represents additional release of stored insulin plus new insulin synthesis from activated enzyme systems.
Other Stimulants of Insulin Secretion
| Factor | Effect |
|---|---|
| Elevated blood glucose | Strong stimulant (primary) |
| Elevated blood amino acids (arginine, lysine) | Potentiate glucose-induced secretion |
| Free fatty acids | Stimulate secretion |
| Gastrointestinal hormones: GLP-1, GIP, gastrin, secretin, CCK | Enhance secretion (incretin effect) |
| Glucagon | Enhances secretion |
| Acetylcholine (parasympathetic) | Stimulates secretion |
| Beta-2 adrenergic stimulation | Mildly stimulates |
Inhibitors of Insulin Secretion
| Factor | Effect |
|---|---|
| Hypoglycemia / fasting | Reduces secretion |
| Somatostatin | Strongly inhibits secretion |
| Norepinephrine (via alpha-adrenergic receptors) | Inhibits exocytosis |
| Leptin | Inhibits secretion |
Pharmacological Note (Sulfonylureas)
Sulfonylurea drugs stimulate insulin secretion by directly blocking K-ATP channels, which causes membrane depolarization and Ca2+ influx by the same mechanism as glucose. This is the basis of their use in Type 2 diabetes mellitus.
PART 2: FUNCTIONS OF INSULIN
Insulin is the principal anabolic hormone. Its effects span carbohydrate, fat, and protein metabolism, acting through the insulin receptor (a tyrosine kinase receptor) on target tissues including liver, muscle, and adipose tissue.
A. Effects on Carbohydrate Metabolism
- Facilitates glucose uptake into skeletal muscle and adipose tissue by promoting translocation of GLUT4 transporters to the cell surface. (Note: glucose uptake in brain, liver, and RBCs is insulin-independent.)
- Promotes glycogenesis - stimulates glycogen synthase, increasing glycogen storage in liver and muscle.
- Inhibits glycogenolysis - suppresses glycogen phosphorylase, reducing breakdown of glycogen.
- Inhibits gluconeogenesis - reduces formation of glucose from amino acids and other substrates in the liver.
- Stimulates glycolysis - increases utilization of glucose for energy.
- Net effect: lowers blood glucose toward normal.
B. Effects on Fat Metabolism
- Promotes lipogenesis - stimulates synthesis of fatty acids and triglycerides in the liver and adipose tissue.
- Inhibits lipolysis - strongly inhibits lipase in adipose tissue, preventing breakdown of stored fat and reducing plasma free fatty acids.
- Inhibits ketogenesis - by reducing fatty acid availability for beta-oxidation in the liver. Without insulin, massive lipolysis leads to ketone body accumulation (ketoacidosis).
- Increases VLDL synthesis - promotes triglyceride packaging and export from the liver.
C. Effects on Protein Metabolism
- Promotes amino acid uptake into cells, especially muscle.
- Stimulates protein synthesis (anabolic effect) - promotes translation and gene expression for proteins.
- Inhibits protein catabolism - reduces breakdown of intracellular proteins.
- Works synergistically with growth hormone to promote body growth.
D. Effects on Potassium
- Stimulates Na+-K+ ATPase - drives K+ into cells.
- This is physiologically important for handling dietary K+ after a meal, preventing hyperkalemia.
- Clinical application: Insulin is used to treat hyperkalemia acutely by driving K+ intracellularly.
E. Effects on the Brain (CNS)
- Insulin stimulates POMC neurons of the hypothalamus to reduce food intake.
- May regulate hepatic glucose production and systemic lipolysis via central pathways.
Summary Table of Insulin Functions
| System | Effect |
|---|---|
| Liver | Glycogenesis, inhibit gluconeogenesis, lipogenesis |
| Muscle | Glucose uptake (GLUT4), glycogenesis, protein synthesis, K+ uptake |
| Adipose | Glucose uptake (GLUT4), lipogenesis, inhibit lipolysis |
| Blood | Lowers glucose, lowers K+, lowers fatty acids |
| Growth | Synergizes with GH for anabolism |
PART 3: NOTE ON DIABETES MELLITUS
Definition
Diabetes mellitus (DM) is a syndrome of impaired carbohydrate, fat, and protein metabolism caused by either:
- Lack of insulin secretion, or
- Decreased sensitivity of tissues to insulin (insulin resistance), or both.
The word "diabetes" comes from Greek meaning to pass through (polyuria), and "mellitus" means honey-sweet, referring to glucosuria.
Classification
Type 1 Diabetes Mellitus (IDDM - Insulin-Dependent DM)
- Pathogenesis: Autoimmune destruction of beta cells in the islets of Langerhans, leading to absolute insulin deficiency.
- Prevalence: ~3-5% of all diabetes; typically presents in children and young adults.
- Mechanism: T-cell mediated destruction of beta cells; autoantibodies (anti-islet cell antibodies, anti-GAD antibodies) are found.
- Key feature: Patients are completely dependent on exogenous insulin for survival.
- Without insulin, patients develop diabetic ketoacidosis (DKA).
Type 2 Diabetes Mellitus (NIDDM - Non-Insulin-Dependent DM)
- Pathogenesis: Combination of insulin resistance in peripheral tissues and progressive beta cell failure (insufficient compensatory insulin secretion).
- Prevalence: ~90-95% of all diabetes; presents typically in overweight/obese adults, but increasingly in children due to rising obesity.
- Mechanism: Insulin resistance is linked to obesity (especially visceral/abdominal fat), reduced GLUT4 activity, impaired insulin signaling pathways (lipotoxicity).
- Over time, beta cells fail to keep up with the demand, and relative insulin deficiency develops.
- Metabolic syndrome is often associated: obesity + insulin resistance + hyperglycemia + dyslipidemia + hypertension.
Gestational Diabetes Mellitus (GDM)
- Defined as hyperglycemia first detected during pregnancy.
- Due to placental hormones causing insulin resistance.
Pathophysiology (Consequences of Insulin Deficiency)
The core problem is described as "starvation in the midst of plenty" - the blood is flooded with glucose but cells cannot take it in.
Two fundamental defects:
- Reduced glucose entry into peripheral tissues (muscle, adipose) - cellular glucose deficiency despite hyperglycemia.
- Increased hepatic glucose output via gluconeogenesis and glycogenolysis.
This leads to:
a. Carbohydrate disturbance:
- Hyperglycemia - elevated blood glucose
- When blood glucose exceeds the renal threshold (~180 mg/dL), glucose spills into urine = glycosuria
- Glycosuria causes osmotic diuresis = polyuria (large urine volumes)
- Polyuria leads to dehydration = polydipsia (excessive thirst)
b. Fat disturbance:
- Without insulin, lipolysis increases dramatically, releasing large amounts of free fatty acids.
- Liver converts these to ketone bodies (acetoacetic acid, beta-hydroxybutyric acid, acetone) = ketonemia and ketonuria
- Accumulation of ketones (which are acids) causes metabolic acidosis = diabetic ketoacidosis (DKA) - primarily in Type 1 DM.
- Fat loss causes weight loss despite eating.
c. Protein disturbance:
- Reduced amino acid uptake and increased protein catabolism.
- Results in muscle wasting, weakness, and cachexia (in untreated Type 1).
- Increased amino acids feed gluconeogenesis.
Clinical Features (The "Polys")
| Symptom | Mechanism |
|---|---|
| Polyuria | Osmotic diuresis from glycosuria |
| Polydipsia | Dehydration from polyuria |
| Polyphagia | Cellular starvation triggers hunger |
| Weight loss | Fat and protein catabolism |
| Weakness | Muscle protein breakdown |
| Glycosuria | Blood glucose exceeds renal threshold |
| Ketonuria | Excess ketone body formation |
Diagnosis
- Fasting plasma glucose >= 126 mg/dL (on two separate occasions)
- Random plasma glucose >= 200 mg/dL with symptoms
- 2-hour OGTT (oral glucose tolerance test) >= 200 mg/dL
- HbA1c >= 6.5%
In diabetes, the oral glucose tolerance test (OGTT) shows a higher rise and slower return of blood glucose to baseline compared to normal individuals.
Complications
Acute Complications:
- Diabetic ketoacidosis (DKA) - mainly Type 1
- Hyperosmolar hyperglycemic state (HHS) - mainly Type 2
- Hypoglycemia (from insulin overdose)
Chronic Complications (due to sustained hyperglycemia damaging blood vessels and nerves):
| Complication | Description |
|---|---|
| Diabetic nephropathy | End-stage renal disease (leading cause) |
| Diabetic retinopathy | Leading cause of blindness |
| Diabetic neuropathy | Peripheral numbness/pain, autonomic dysfunction |
| Diabetic macroangiopathy | Atherosclerosis - heart attack, stroke |
| Diabetic foot | Neuropathy + peripheral vascular disease |
The mechanism of these complications involves: advanced glycation end products (AGEs), sorbitol accumulation (polyol pathway), oxidative stress, and protein kinase C activation - all due to chronic hyperglycemia.
Treatment
| Type | Treatment |
|---|---|
| Type 1 DM | Insulin replacement (mandatory) - multiple daily injections or insulin pump |
| Type 2 DM | Lifestyle modification (diet + exercise) + oral hypoglycemics (metformin first-line, sulfonylureas, DPP-4 inhibitors, SGLT2 inhibitors) + insulin when needed |
| GDM | Dietary control, insulin if needed |
SUMMARY
- Insulin secretion from beta cells is primarily triggered by glucose through the GLUT2 → Glucokinase → ATP → K-ATP channel closure → Membrane depolarization → Ca2+ influx → Exocytosis pathway.
- Insulin secretion is biphasic: an immediate first phase and a sustained second phase.
- Insulin's main functions are glucose uptake, glycogenesis, lipogenesis, protein synthesis, and anti-lipolysis - all anabolic effects.
- Diabetes mellitus results from insulin deficiency (Type 1) or insulin resistance (Type 2), leading to the classic triad of polyuria, polydipsia, and polyphagia, along with hyperglycemia, glycosuria, and potentially ketoacidosis.
- Long-term complications target the kidney, retina, nerves, and blood vessels.
Sources: Guyton and Hall Textbook of Medical Physiology (14th Ed.), Ganong's Review of Medical Physiology (26th Ed.), Costanzo Physiology (7th Ed.), Medical Physiology - Boulpaep & Boron
This is a shared conversation. Sign in to Orris to start your own chat.