Adrenal medullary, hormones of AM, biosynthesis, secretion, MOA, regulation and metabolic effects of AM hormones with Clicnical disorders this is my lecture topic for tommorow give a brief summary
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from multiple textbooks. Let me compile the full lecture summary.
Adrenal Medulla (AM) - Lecture Summary
1. Structure and Overview
The adrenal medulla (AM) is a modified sympathetic ganglion - it bridges the endocrine and sympathetic nervous systems. Its cells, called chromaffin cells, derive from neural crest cells that migrate into the center of the adrenal cortex (which is mesodermal). They are the structural and functional equivalents of postganglionic sympathetic neurons.
The AM has a unique portal blood supply: blood flows from a subcapsular plexus through the adrenal cortex first, then into the medulla - exposing chromaffin cells to the highest glucocorticoid concentrations of any tissue in the body (a crucial point for epinephrine synthesis).
- Costanzo Physiology, p. 58
- Medical Physiology (Boron & Boulpaep), p. 1511
2. Hormones of the Adrenal Medulla
| Hormone | Proportion Secreted |
|---|---|
| Epinephrine (adrenaline) | ~80% |
| Norepinephrine (noradrenaline) | ~20% |
| Dopamine | Trace |
Also co-released: ATP, Ca²+, and chromogranins (especially chromogranin B in humans; chromogranin A is used as a marker of AM activity).
3. Biosynthesis of Catecholamines
The pathway proceeds from the amino acid Tyrosine through four enzymatic steps:
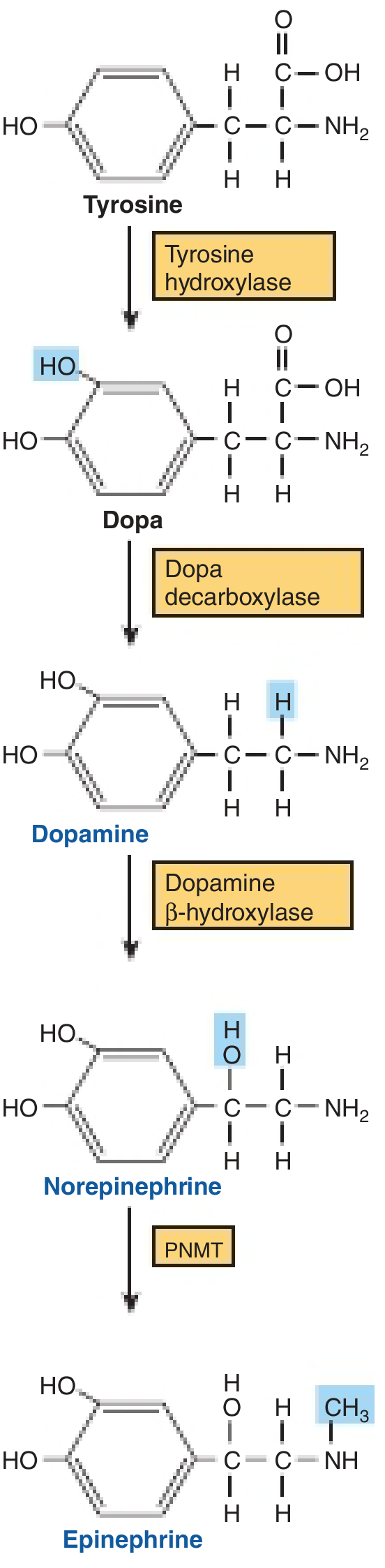
Tyrosine → L-DOPA → Dopamine → Norepinephrine → Epinephrine
| Step | Enzyme | Location | Key Notes |
|---|---|---|---|
| Tyrosine → L-DOPA | Tyrosine hydroxylase | Cytosol | Rate-limiting step; requires tetrahydropteridine cofactor; feedback-inhibited by catecholamines |
| L-DOPA → Dopamine | Dopa decarboxylase (AAAD) | Cytosol | Requires pyridoxal phosphate; inhibited by α-methyldopa |
| Dopamine → Norepinephrine | Dopamine β-hydroxylase (DBH) | Inside secretory granule | Monooxygenase; uses ascorbate, Cu²+, fumarate |
| Norepinephrine → Epinephrine | PNMT (phenylethanolamine-N-methyltransferase) | Cytosol | Adds methyl group from S-adenosylmethionine; present only in adrenal medulla (+ tiny amounts in heart ganglia and CNS) |
Key transport steps: Dopamine enters the granule via VMAT1 (vesicular monoamine transporter 1). Norepinephrine exits the granule → converted to epinephrine by cytosolic PNMT → re-enters granule via VMAT1 for storage.
- Harper's Illustrated Biochemistry 32e, p. 511
- Medical Physiology (Boron & Boulpaep), p. 1512-1513
4. Secretion
Secretion is triggered by ACh released from preganglionic splanchnic nerve fibers acting on nicotinic receptors on chromaffin cells. This causes depolarization → opens voltage-gated Ca²+ channels → rise in [Ca²+] → exocytosis of dense-core secretory granules.
- Catecholamines are stored at very high concentrations (~0.5 M) bound to chromogranins (so they're not osmotically active)
- Exocytosis releases catecholamines + ATP + chromogranin A simultaneously
- The hormones dissociate from the binding complex once in the circulation
Degradation (half-life ~10 seconds for epinephrine):
- COMT (catechol-O-methyltransferase) - in endothelial cells, heart, liver, kidneys - converts:
- Epinephrine → Metanephrine
- Norepinephrine → Normetanephrine
- MAO (monoamine oxidase) converts these to VMA (vanillylmandelic acid)
- Liver/gut conjugate to sulfate or glucuronide → excreted in urine
Urinary catecholamines, metanephrines, and VMA measure total AM + sympathetic output - important for diagnosing pheochromocytoma.
5. Mechanism of Action (MOA)
Catecholamines bind adrenergic receptors (GPCRs) on cell surfaces:
| Receptor | G Protein | Signal | Key Effects |
|---|---|---|---|
| α₁ | Gαq | ↑PLC → ↑IP₃ → ↑Ca²+ | Vasoconstriction, smooth muscle contraction |
| α₂ | Gαi | ↓Adenylyl cyclase → ↓cAMP | Inhibits NE release (presynaptic), inhibits insulin secretion |
| β₁ | Gαs | ↑Adenylyl cyclase → ↑cAMP | ↑Heart rate, ↑contractility |
| β₂ | Gαs | ↑cAMP | Bronchodilation, vasodilation in muscle, glycogenolysis |
| β₃ | Gαs | ↑cAMP | Lipolysis in adipose tissue |
Epinephrine acts on all α and β receptors. Norepinephrine acts mainly on α receptors and β₁ (minimal β₂ effect).
(Robert Lefkowitz and Brian Kobilka received the 2012 Nobel Prize in Chemistry for their work on GPCRs/adrenoceptors.)
- Medical Physiology (Boron & Boulpaep), p. 1513-1514
6. Regulation of AM Secretion
Central nervous system is the primary regulator - there is NO endocrine feedback loop for AM hormones.
| Stimulus | Mechanism |
|---|---|
| Stress / fear / exercise | CNS activates splanchnic preganglionic neurons → ACh release → chromaffin cell exocytosis |
| Hypoglycemia (blood glucose < 3.5 mM) | Sensed by CNS → ↑sympathetic outflow → ↑epinephrine release → hepatic glycogenolysis → restores blood glucose |
| Cortisol (from adrenal cortex portal blood) | Upregulates PNMT → ensures continued epinephrine synthesis; synergy between ACTH-cortisol axis and sympathetic-epinephrine axis |
| ACTH | Stimulates synthesis of L-DOPA and norepinephrine |
This cortisol-PNMT link explains why pheochromocytomas (which are distant from the cortex) secrete mainly norepinephrine - they lack sufficient cortisol to induce PNMT.
7. Metabolic Effects of AM Hormones
The catecholamines are counterregulatory (contrainsular) hormones - they mobilize fuels during stress and suppress insulin.
Carbohydrate Metabolism
- Glycogenolysis in liver and muscle (via β receptors → ↑cAMP → ↑glycogen phosphorylase)
- Gluconeogenesis stimulated
- ↓Insulin secretion (via α₂ receptors on pancreatic β cells) → net hyperglycemia
- ↑Glucagon secretion (via β receptors on α cells)
Fat Metabolism
- Lipolysis in adipose tissue (via β₃ → ↑cAMP → activates hormone-sensitive lipase)
- Increases free fatty acids and glycerol availability for fuel
Other Metabolic Actions
- ↑Basal metabolic rate (thermogenesis, especially via β₃ in brown adipose tissue)
- ↑Oxygen consumption
- ↓Peripheral glucose uptake (to spare glucose for the brain)
Cardiovascular and Other Effects (Fight-or-Flight)
-
↑Heart rate and contractility (β₁)
-
Vasoconstriction in skin/kidneys/splanchnic (α₁)
-
Vasodilation in skeletal muscle (β₂)
-
Bronchodilation (β₂)
-
Pupillary dilation
-
↓GI motility and secretion
-
↑Sphincter tone (bowel and bladder)
-
Piloerection
-
Basic Medical Biochemistry 6e, p. key concepts
-
Costanzo Physiology, p. 58
8. Clinical Disorders
Pheochromocytoma
A tumor of chromaffin cells of the adrenal medulla (or extra-adrenal paraganglia). All pheochromocytomas are considered potentially malignant - the term "metastatic pheochromocytoma" is now preferred over "malignant."
Epidemiology:
- 30-40% harbor germline mutations (RET, VHL, NF1, SDH genes)
- Associated syndromes: MEN-2, von Hippel-Lindau (VHL), neurofibromatosis type 1
Genetics:
- Two gene classes: (1) Growth factor receptor pathway (RET, NF1) and (2) Hypoxia/HIF pathway (VHL, EPAS1/HIF-2α) - the "pseudohypoxia" phenotype
Clinical Features ("5 Ps"): Paroxysmal hypertension, Palpitations, Perspiration, Headache, Pallor/Pain
- Hypertension in 90% (paroxysmal in 2/3)
- Tachycardia, tremor, anxiousness, glucose intolerance
- Episodes precipitated by: emotional stress, exercise, posture change, palpation, micturition (bladder paraganglioma)
- Serious complications: catecholamine cardiomyopathy, MI, pulmonary edema, CVA, VF
Histology: Polygonal chromaffin cells in nests called "zellballen" surrounded by sustentacular cells; positive for chromogranin, synaptophysin (chief cells) and S-100 (sustentacular cells); electron microscopy shows membrane-bound electron-dense secretory granules.
Lab Diagnosis:
- ↑Urinary free catecholamines, metanephrines, VMA (24-hour urine)
- ↑Plasma metanephrines (most sensitive test)
Treatment:
-
α-adrenergic blocker first (phenoxybenzamine) to control hypertension preoperatively
-
Then β-blocker (never give β-blocker first - can cause unopposed α-vasoconstriction crisis)
-
Surgical excision
-
Robbins & Cotran Pathologic Basis of Disease, p. 1040-1041
-
Costanzo Physiology, Box 2.1
Quick Comparison: AM vs Sympathetic Postganglionic Neurons
| Feature | Adrenal Medulla | Sympathetic Neurons |
|---|---|---|
| Main secretion | Epinephrine (80%) | Norepinephrine only |
| Why different? | Has PNMT (needs cortisol) | No PNMT |
| Route | Hormonal (blood) | Synaptic (neurotransmitter) |
| Trigger | ACh → nicotinic receptor | ACh → nicotinic receptor |
Key Buzz-Words for Exam
- Rate-limiting enzyme: Tyrosine hydroxylase
- Only in AM: PNMT (requires cortisol from portal blood)
- Storage: Dense-core granules, VMAT1 transporter, chromogranins
- Degradation: COMT → metanephrines; MAO → VMA
- MOA: GPCRs (α₁/Gq, α₂/Gi, β/Gs)
- Fight-or-flight: central CNS control, no hormonal feedback loop
- Hypoglycemia response: CNS senses → ↑splanchnic firing → ↑Epi → glycogenolysis
- Pheo rule of 10s (older): 10% bilateral, 10% malignant, 10% extra-adrenal, 10% children (now updated - up to 40% have germline mutations)
- Pheo diagnosis: Plasma/urine metanephrines, VMA
- Pheo pre-op: α-blocker FIRST, then β-blocker
Good luck with your lecture tomorrow!
This is a shared conversation. Sign in to Orris to start your own chat.