Para umbilical Hernia and procedure
paraumbilical hernia anatomy repair surgical procedure
"umbilical hernia" AND repair
Paraumbilical Hernia
Definition
- Bailey and Love's Short Practice of Surgery, p. 1094
- S Das: A Manual on Clinical Surgery, p. 5808
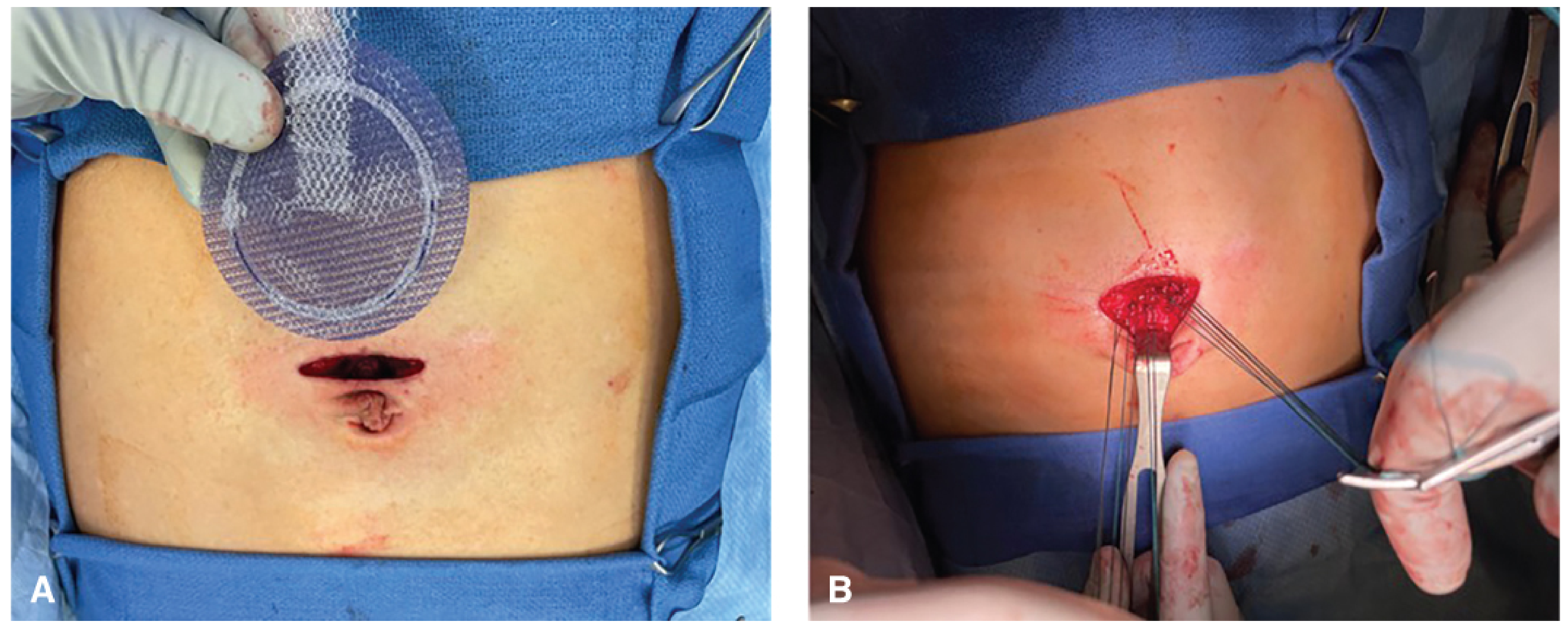
Clinical Photo

Epidemiology & Predisposing Factors
- The commonest acquired umbilical hernia in adults
- Affects obese middle-aged and elderly women predominantly (women > men)
- Conditions causing stretching/thinning of the linea alba:
- Pregnancy
- Obesity (most important)
- Liver cirrhosis with ascites
- Large ovarian cysts or fibroids
- Raised intra-abdominal pressure from any cause
Anatomy of the Defect
- The defect lies in the linea alba, between the two rectus muscles, just superior to the true umbilical ring
- The neck is characteristically narrow relative to the sac - this is why these hernias are prone to complications
- Contents: omentum (firm, dull to percussion) or small/large bowel (soft, resonant to percussion)
- Many become irreducible due to adhesions within the sac or a narrow neck
Clinical Features
| Feature | Description |
|---|---|
| Site | Above or adjacent to the umbilicus; bulge is crescent-shaped/paraumbilical |
| Onset | Middle to old age |
| Sex | Women > Men |
| Symptoms | Pain and swelling; pain can precede visible swelling in small hernias |
| Reducibility | Often irreducible due to adhesions or narrow neck |
| Consistency | Firm (omental content) or soft/resonant (bowel) |
| Complications | Intermittent obstruction; strangulation less common but serious |
Complications
- Incarceration - contents trapped but viable
- Obstruction - most common complication
- Strangulation - omentum or bowel; gangrene can develop rapidly due to narrow neck
- Skin ulceration - over very large, thin-skinned hernias
- Spontaneous rupture - extremely rare
Because of the narrow neck and fibrous edge, delay to surgery in an emergency can lead to gangrene of omentum or bowel. Large hernias may be multiloculated with strangulation in one loculus while other areas feel soft.
Investigations
- Usually clinical diagnosis
- USS / CT abdomen if:
- Diagnosis uncertain
- Suspected incarceration
- Liver disease/ascites evaluation pre-operatively
Treatment
Conservative Management
- Asymptomatic very small hernias
- High operative risk patients
- Pre-operatively: weight loss, smoking cessation (reduces cough-related intra-abdominal pressure)
- Hernia contains bowel (high strangulation risk due to narrow neck)
- Enlarging or symptomatic hernias
- Incarcerated/obstructed/strangulated (emergency)
Surgical Repair
1. Open Repair - Mayo's "Waistcoat-over-Trousers" Technique
- A transverse (curved) skin incision is made just below/around the umbilicus, overlying the hernia
- The hernia sac is dissected down to the fascial level; surrounding fascia is cleared circumferentially
- The sac is opened and contents reduced to the peritoneal cavity
- The sac may be excised or inverted; the peritoneum is closed
- The fascial defect is extended transversely to create proper fascial flaps
- The fascial edges are closed in an overlapping "vest-over-pants" (waistcoat-over-trousers) fashion - the superior flap is sutured on top of the inferior flap, creating a double layer
- Non-absorbable sutures (e.g., Prolene/nylon) are used
- Redundant skin may need excision for cosmetic result; skin closed routinely
- Bailey and Love's Short Practice of Surgery, p. 1095
2. Open Mesh Repair (Tension-free Hernioplasty) - Procedure of Choice
- Same initial dissection as above - transverse incision, sac dissection, contents reduced, sac excised/inverted, peritoneum closed
- A synthetic polypropylene mesh (Prolene mesh) is fashioned to cover the defect with adequate overlap (at least 3-5 cm in all directions)
- Mesh is placed in the preperitoneal/retromuscular or onlay position over the defect
- Fixed with non-absorbable sutures or tacks
- Wound closure in layers
- Tension-free - no tissue stress
- Significantly lower recurrence rate (near zero vs. 10-20% with Mayo's)
- No recurrences in series where mesh was used
"Current evidence advises the use of mesh even in small defects, and certainly for all defects larger than 2 cm, owing to the high likelihood of recurrence." - Bailey and Love, p. 1095
3. Laparoscopic Repair
- Camera port and two working ports placed laterally, well away from the defect
- Hernia contents reduced by traction + external pressure
- Falciform ligament (above) and median umbilical fold (below) may be taken down to create a smooth surface for mesh placement
- A disc of non-adherent intraperitoneal mesh (anti-adhesion coating on visceral side) is introduced and positioned on the undersurface of the abdominal wall, centred on the defect with generous overlap
- Fixed to peritoneum and posterior rectus sheaths using staples, tacks, or sutures
- Fewer wound complications than open repair
- Allows use of large mesh pieces
- Better for obese patients
-
Requires specialised equipment and expensive intraperitoneal mesh
-
Risk of bowel adhesion, erosion, fistulation with intraperitoneal mesh
-
Post-operative pain (24-48 h) can mimic peritonitis due to mesh/tacks
-
Potential chronic pain from fixing tacks/sutures
-
Bailey and Love's Short Practice of Surgery, p. 1095
4. Emergency Repair
- Performed under general anaesthesia (cannot use local)
- Same open approach but:
- Bowel/omentum viability assessed
- Non-viable bowel: resection and primary anastomosis
- Non-viable omentum: omentectomy
- Mesh use is relative contraindication in contaminated field - primary tissue repair preferred if contamination present; or use biologic mesh
Anaesthesia Options
| Hernia Size/Situation | Preferred Anaesthesia |
|---|---|
| Small, elective | Local anaesthetic + sedation |
| Routine elective | General anaesthesia (most common) |
| Selected cases | Regional/spinal anaesthesia |
| Emergency | General anaesthesia |
Special Situations
- Pregnancy: Surgery strongly discouraged during pregnancy; advise conservative management until postpartum
- Cirrhosis with ascites: Very high mortality/morbidity, especially Child's B and C. Fascial repair with fine continuous sutures minimises risk of post-operative ascites leakage; hepatology input essential
- Post-partum women: Advise exercise, weight loss, abdominal muscle tone improvement before elective repair
Post-operative Complications
| Complication | Management |
|---|---|
| Wound infection | Antibiotics, drainage |
| Seroma formation | Aspiration/drainage, dressings |
| Haematoma | Conservative vs. evacuation |
| Recurrence | More common with primary suture repair; rare with mesh |
| Chronic pain | From mesh tacks/sutures; may need intervention |
| Bowel adhesions (laparoscopic) | Anti-adhesion mesh reduces risk |
Key Comparison: Mayo's vs. Mesh Repair
| Feature | Mayo's Repair | Mesh Repair |
|---|---|---|
| Technique | Overlapping fascial flaps | Tension-free mesh placement |
| Recurrence | Higher (10-20%+) | Very low (<1-3%) |
| Best for | Small defects < 2 cm | All defects, especially > 2 cm |
| Current evidence | Less favoured | Procedure of choice |
| Contaminated field | Acceptable | Avoid synthetic mesh |
Para umbilical Hernia and it's procedure , careful condition to follow during surgery
paraumbilical hernia surgical precautions intraoperative care careful conditions
"paraumbilical hernia" OR "umbilical hernia" AND surgery complications precautions
"umbilical hernia" AND mesh AND repair
Paraumbilical Hernia - Procedure & Careful Intraoperative Conditions
What is a Paraumbilical Hernia?
Clinical Appearance
Surgical Procedures
1. Open Primary Suture Repair (Mayo's "Waistcoat-over-Trousers")
- Curvilinear (infraumbilical or supraumbilical) skin incision placed close to the hernia
- Dissect through dermis; identify and expose the hernia sac and umbilical stalk circumferentially
- Dissect the sac off the umbilical stalk - this step requires great care to avoid inadvertent skin injury
- Open the sac; reduce contents into the peritoneal cavity. If omentum/preperitoneal fat is irreducible, tie and excise at fascial level
- Peritoneum closed with absorbable suture
- Fascia cleared circumferentially to ensure adequate fascial bites
- Defect extended transversely; fascial edges closed in overlapping "vest-over-pants" fashion (superior flap over inferior) using non-absorbable/slowly absorbable monofilament sutures (figure-of-eight or simple interrupted, transverse direction)
- Umbilical stalk reapproximated to linea alba to restore cosmetic umbilical contour
- Redundant skin excised if needed; subcutaneous layers and skin closed
2. Open Mesh Repair (Tension-Free Hernioplasty) - Procedure of Choice
a) Open Preperitoneal Mesh Repair
- Curvilinear incision inferior or superior to the umbilicus
- Dissect to identify the hernia sac; preserve the sac to facilitate entry into the preperitoneal plane
- Dissect in the preperitoneal plane circumferentially under the fascia, creating a pocket for mesh with 3-5 cm overlap in all directions
- Close any peritoneal holes with absorbable sutures
- Place a flat polypropylene (Prolene) mesh in preperitoneal space; lay it flat (intra-abdominal pressure keeps it sandwiched - fixation sutures often not required)
- Close the fascial defect over the mesh with permanent or slowly absorbable sutures; close skin
b) Open Intraperitoneal Mesh Repair (Hernia Patch)
- Used when peritoneum is thin and tears during preperitoneal dissection
- A barrier-coated (anti-adhesion) hernia patch is placed intraperitoneally
- Sac transected at fascial level; contents reduced; mesh introduced into abdominal cavity and fixed with sutures/tails/memory ring
- Fascia reapproximated over mesh; skin closed
3. Laparoscopic Repair
- Camera port + two lateral working ports (placed well away from the defect)
- Reduce hernia contents by traction + external manual pressure
- Take down falciform ligament (above) and median umbilical fold (below) to create a smooth surface for mesh placement
- Introduce disc of intraperitoneal non-adherent mesh; position centred on defect with generous overlap
- Fix to peritoneum and posterior rectus sheaths using staples, tacks, or sutures
4. Emergency Repair (Incarceration/Obstruction/Strangulation)
- General anaesthesia - always
- Open approach preferred
- Assess viability of bowel/omentum
- Non-viable omentum: omentectomy
- Non-viable bowel: resection and primary anastomosis
- In a contaminated field: avoid synthetic mesh - use primary suture repair only, or biologic mesh; definitive mesh repair deferred to a later elective procedure
- Multiloculated hernias: examine all loculi - strangulated bowel may be in one compartment while others feel soft
Intraoperative Mesh Repair - Surgical Photo
⚠️ Careful Conditions to Follow During Surgery
1. Skin & Umbilicus Preservation
"Care must be taken during sac dissection to ensure the skin is not inadvertently injured."
- Fischer's Mastery of Surgery, p.5905
- Dissect the sac meticulously off the umbilical stalk without buttonholing the overlying skin
- Preserve the blood supply to the umbilical skin flap - aggressive or wide dissection can devascularise the umbilicus, leading to necrosis
- Reapproximate the umbilical stalk back to the linea alba at closure to prevent a flat, cosmetically unacceptable scar
2. Do Not Inadvertently Enlarge the Hernia Defect
"Care should be taken to not enlarge the hernia defect unless necessary."
- Fischer's Mastery of Surgery, p.5905
- When contents are difficult to reduce due to large volume, do not forcibly enlarge the opening
- If preperitoneal fat/omentum cannot be reduced, tie and excise it cleanly at fascial level rather than tearing
- Uncontrolled defect enlargement complicates mesh sizing and fascial closure
3. Circumferential Fascial Clearance Before Closure
- The fascia around the defect must be cleared circumferentially before any suture or mesh placement
- This ensures adequate fascial bites during closure and proper mesh overlap
- Failure to clear fascia leads to inadequate repair and recurrence
4. Peritoneal Integrity
- Before placing mesh in the preperitoneal space, close all peritoneal holes with absorbable suture
- Unrecognised peritoneal defects allow mesh to migrate into the abdominal cavity and contact bowel - a serious complication
- If peritoneum is thin and tears easily during dissection, switch to intraperitoneal mesh with anti-adhesion coating rather than persisting with preperitoneal technique
5. Mesh Selection - Anti-Adhesion Coating is Mandatory Intraperitoneally
"If the mesh is placed in contact with the viscera, it is imperative that a mesh with an antiadhesive barrier be utilized."
- Fischer's Mastery of Surgery, p.5911
| Mesh Position | Mesh Type Required |
|---|---|
| Onlay (over fascia) | Flat non-coated polypropylene |
| Preperitoneal | Flat polypropylene or hernia patch |
| Intraperitoneal (contact with bowel) | Anti-adhesion barrier-coated mesh ONLY |
- Dense bowel adhesions
- Bowel erosion
- Entero-cutaneous fistula (serious, life-threatening)
6. Adequate Mesh Overlap
- Mesh must extend at least 3-5 cm beyond the fascial defect in all directions
- Insufficient overlap is the most common technical reason for recurrence
- Do not undersize the mesh to save time or cost
7. Avoid Mesh in Contaminated/Infected Field
"In the presence of established strangulation, mesh should be avoided as the risk of infection is too high."
- Bailey and Love's Short Practice of Surgery, p.1095
- Emergency cases with strangulated bowel or omentum: use suture repair only
- Synthetic mesh in contaminated fields leads to wound infection, mesh infection, chronic sinus, and explantation
- Schedule a definitive elective mesh repair at a later date once the field is clean
8. Bowel Viability Check in Emergency Cases
- Before closing, carefully assess all bowel and omentum for viability
- Signs of non-viability: black/dark colour, no peristalsis, no bleeding on cut edge, loss of mesenteric pulse
- Wrap questionable bowel in warm moist packs, wait 5 minutes - if no improvement, resect
- In multiloculated hernias: examine every loculus independently - do not assume all compartments are viable because one looks normal
9. Mesh Fixation - Avoid Chronic Pain
- Tacks and sutures used to fix intraperitoneal mesh can pierce nerves and cause chronic post-operative pain
- Use the minimum required fixation
- Intra-abdominal pressure alone is sufficient to hold preperitoneal mesh flat - over-fixation is unnecessary
10. Laparoscopic-Specific Precautions
- In the presence of dense peritoneal adhesions, the laparoscopic surgeon must take great care because bowel injury is possible and may not be recognised intraoperatively
- If occult bowel injury occurs and is missed, it presents as peritonitis post-operatively - a life-threatening complication
- Consider conversion to open if adhesiolysis is unsafe laparoscopically
11. Special Patient Conditions
| Condition | Intraoperative Precaution |
|---|---|
| Liver cirrhosis with ascites | Use fine continuous sutures on fascia; minimises risk of post-op ascites leak through repair. Child's B/C: very high mortality - ensure hepatology input and optimal preoperative preparation |
| Obesity | Prefer laparoscopic approach - fewer wound complications; wide subcutaneous flaps in open onlay repair significantly increase SSI (surgical site infection) risk |
| Thin peritoneum | Do not persist with preperitoneal dissection if peritoneum tears easily; switch to intraperitoneal barrier-coated mesh technique |
| Pregnancy | Surgery strongly discouraged during pregnancy; defer to elective post-partum repair |
| Diabetes / COPD / Collagen disorders | Higher recurrence with suture repair; use mesh even for small defects |
12. Post-Operative Intraperitoneal Mesh Pain Warning
- Intraperitoneal mesh tacks/fixation devices can cause severe pain lasting 24-48 hours post-operatively that mimics peritonitis
- Surgical team must be aware to avoid unnecessary re-exploration; careful clinical monitoring is required to distinguish this from true peritonitis
Summary: Key "Do's and Don'ts"
| DO | DON'T |
|---|---|
| Clear fascia circumferentially before closure | Enlarge the defect unnecessarily |
| Use anti-adhesion mesh if placing intraperitoneally | Use bare mesh in contact with viscera |
| Ensure 3-5 cm mesh overlap | Undersize the mesh |
| Assess bowel viability in all emergency cases | Place mesh in contaminated/strangulated field |
| Use suture repair only in emergency contaminated cases | Ignore thin/torn peritoneum during preperitoneal dissection |
| Reapproximate umbilical stalk for cosmesis | Aggressively dissect and devascularise umbilical skin |
| Examine all loculi in multiloculated hernias | Assume one safe loculus means all are safe |
- Bailey and Love's Short Practice of Surgery, 28th Ed., pp. 1094-1096
- Fischer's Mastery of Surgery, 8th Ed., pp. 5905-5912
Incisional hernia and procedure
incisional hernia definition causes classification surgical repair procedure
"incisional hernia" AND repair
Incisional Hernia
Definition
Clinical Appearance

Incidence
- 10-50% of laparotomy incisions
- 1-5% of laparoscopic port-site incisions
- Approximately 25-30% of patients develop an incisional hernia when a wound infection occurs after abdominal surgery
Aetiology & Risk Factors
A. Patient Factors
| Factor | Mechanism |
|---|---|
| Obesity | Increased intra-abdominal pressure; poor tissue perfusion |
| Malnutrition | Poor collagen synthesis; impaired wound healing |
| Diabetes | Impaired healing; susceptibility to infection |
| Immunosuppression / Steroids | Reduced collagen formation |
| Chronic cough (COPD) | Repeated surges in intra-abdominal pressure |
| Cancer | Catabolic state; malnutrition |
| Genetic collagen disorders | Structurally weak fascia |
| Smoking | Tissue hypoxia; impaired healing |
B. Wound Factors
- Poor quality wound edges (ischaemic, infected, irradiated)
- Excessive wound tension
- Wound infection - single most important avoidable cause; 25-30% of infected wounds develop incisional hernia
C. Surgical Factors
- Inappropriate suture material
- Poor closure technique (large bites, incorporating fat/muscle instead of fascia only)
- Drains brought out through the wound instead of separate stab incisions
- Suture length-to-wound length ratio < 4:1
Pathogenesis
- The process starts with musculofascial layer disruption in the early postoperative period
- This may rapidly progress to full-thickness wound dehiscence (heralded by serosanguineous discharge around day 6 post-op)
- More commonly the skin heals but deep fascia separates unnoticed
- A visible hernia swelling may take weeks, months, or even years to appear
- The hernia tends to enlarge progressively with time
When fat and muscle are incorporated in a fascial stitch, traction on the suture line cuts through or necrotises these softer tissues. The suture line loses tension, the fascia edges separate, and a hernia forms. Only fascia should be taken in each suture bite.
- Fischer's Mastery of Surgery, p. 5842
EHS Classification of Incisional Hernia
| Location | Subtype | Code |
|---|---|---|
| Midline | Subxiphoid | M1 |
| Epigastric | M2 | |
| Umbilical | M3 | |
| Infraumbilical | M4 | |
| Suprapubic | M5 | |
| Lateral | Subcostal | L1 |
| Flank | L2 | |
| Iliac | L3 | |
| Lumbar | L4 |
- W1 = < 4 cm
- W2 = 4-10 cm
- W3 = > 10 cm
Ventral Hernia Working Group (VHWG) Grade
| Grade | Profile | Criteria |
|---|---|---|
| 1 | Low risk | Healthy patient, no wound infection history |
| 2 | Comorbid | Smoker, obese, diabetic, immunosuppressed, COPD |
| 3 | Potentially contaminated | Previous wound infection, stoma present, GI tract violation |
| 4 | Infected | Infected mesh, septic dehiscence |
Clinical Features
- Localised swelling at surgical scar, or diffuse bulging of the whole incision length
- Multiple discrete defects along one scar are common; unsuspected extra defects are frequently found at surgery
- Progressive enlargement; overlying skin becomes thin and atrophic
- Skin ulceration from local trauma/microvascular damage
- Intestinal obstruction - common (due to coexisting internal adhesions)
- Strangulation - less frequent than obstruction because most incisional hernias are shallow and wide-necked; most likely when the defect is small relative to sac size
- "Loss of domain" - in massive hernias, abdominal contents have permanently migrated outside the abdominal cavity
Investigations
- Usually clinical diagnosis
- CT abdomen (with Valsalva if possible) - defines exact number and size of defects, contents, abdominal wall anatomy, and presence of adhesions; essential for complex/large hernias and pre-operative planning
Pre-operative Optimisation ("Prehabilitation")
- Weight loss - 7% bodyweight loss achieves significant metabolic improvement; 5 kg weight loss creates ~1 litre extra abdominal space in men
- Smoking cessation - reduces wound infection, tissue hypoxia
- Glycaemic control - target HbA1c < 8%
- Nutritional correction
- Core strength exercises
- Multidisciplinary team assessment in complex cases
Principles of Surgical Repair
- The repair must cover the whole length of the previous incision (to capture all defects, including unsuspected ones)
- Musculofascial layers must be approximated with minimal tension
- Prosthetic mesh must be used to reduce recurrence risk
- Bailey and Love's Short Practice of Surgery, p. 1100
Surgical Procedures
1. Open Primary Suture Repair (Tissue Repair)
- Fascial edges cleared of all fat and muscle (fascia only in each bite)
- 5 mm tissue bites at 5 mm intervals from wound edge
- Running monofilament 2-0 slowly absorbable suture (e.g. PDS) on 30-40 mm needle
- Suture length-to-wound length ratio must be ≥ 4:1
- For wide midline defects: interrupted figure-of-eight sutures placed loosely first along entire wound, then cinched together uniformly to distribute tension
2. Open Mesh Repair - The Gold Standard
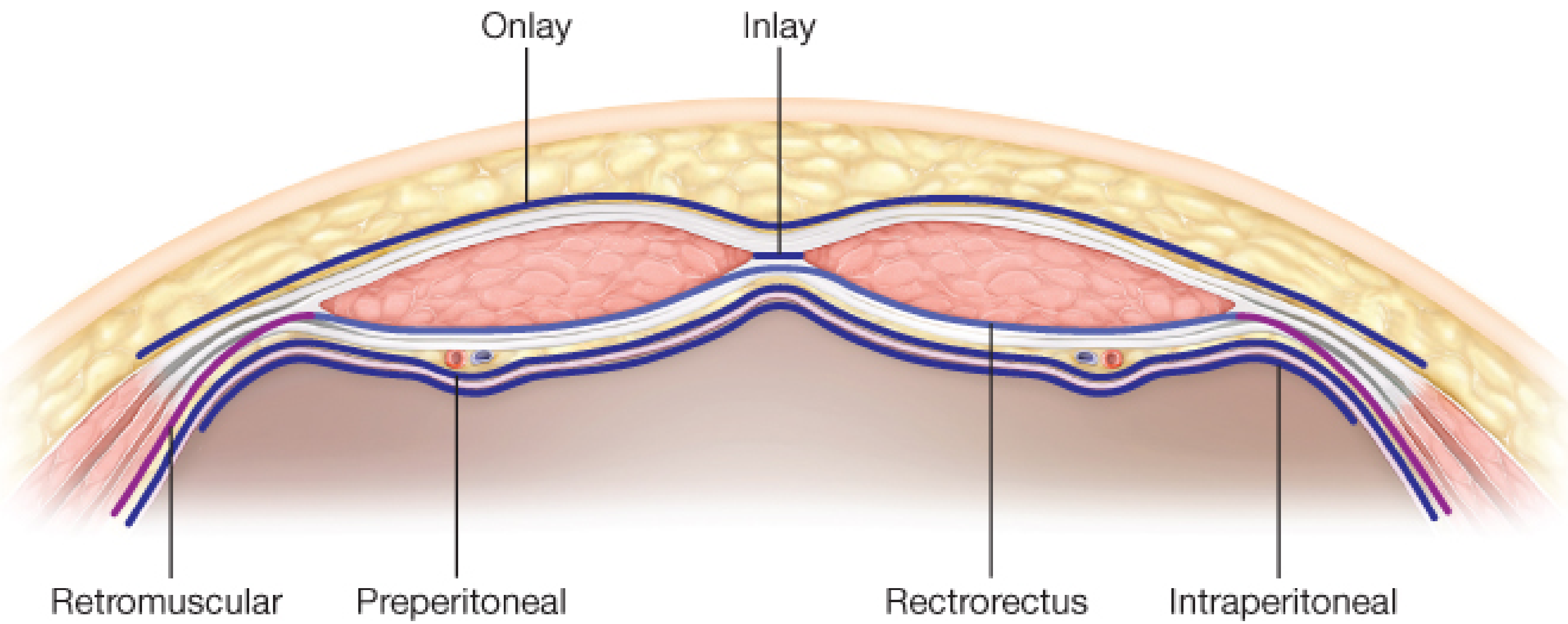
a) Onlay Mesh Repair
- Mesh placed on top of anterior rectus sheath after primary fascial closure
- Simplest technique; good outcomes in experienced hands
- Requires elevation of large skin flaps - increases seroma risk and skin ischaemia/necrosis
- Risk of mesh exposure if wound infection occurs
- Fix mesh with non-absorbable sutures + fibrin glue; place drains on top of mesh to reduce seroma
b) Retrorectus / Retromuscular (Sublay) Repair - Preferred Position
- Mesh placed between rectus abdominis muscle and posterior rectus sheath
- Best outcomes - lowest recurrence and lowest SSI rates
- Protected from wound infection; well-vascularised plane
- Requires dissection of retrorectus space (Rives-Stoppa technique)
- Can be extended laterally by Transversus Abdominis Release (TAR) for larger defects, creating a wide retromuscular plane
c) Preperitoneal Repair
- Mesh placed between transversalis fascia and peritoneum
- Good alternative when retrorectus plane difficult
- Requires careful dissection to avoid peritoneal tear
d) Intraperitoneal Onlay Mesh (IPOM) - Open
- Mesh placed inside abdomen, directly on peritoneum
- Must use anti-adhesion barrier-coated mesh - bare polypropylene must never contact viscera
- Fixed using transfascial "U" sutures (Reverdin needle or Carter-Thomason passer) placed close together around mesh circumference
- Technically difficult to keep flat
- Avoids large skin flaps; useful when retrorectus plane difficult
e) Inlay (Bridge) Repair
"Inlay mesh should be avoided due to its extremely high recurrence rates."
- Fischer's Mastery of Surgery, p. 5910
- Mesh placed as interposition between muscle edges - not sutured to overlying fascia, just bridges the gap
- Only used in emergency or non-optimised patients as a temporary measure
- Use cheapest non-permanent mesh; plan for future definitive repair
3. Laparoscopic Repair (IPOM-Lap)
- Laparoscopy; careful adhesiolysis under direct vision
- Hernia contents reduced; fibrous defect margins exposed
- Falciform ligament and median umbilical fold taken down as needed
- Some surgeons close the fascial defect(s) with transcutaneous sutures before mesh; others bridge without closure (only safe for small defects)
- Anti-adhesion barrier mesh (IPOM mesh) introduced and positioned; centred on defect with generous overlap (≥ 3-5 cm)
- Fixed with staples, tacks, or transfascial sutures to peritoneum and posterior rectus sheath
- "Pseudo-recurrence" - mesh bulging outward after laparoscopic bridging repair without fascial closure; common with large defects - not a true recurrence but a recognised phenomenon
4. Robotic Repair
- Growing evidence supports robotic-assisted repair (PMID 37725188)
- Allows retromuscular mesh placement (rTAR) with minimally invasive access
- Better ergonomics for complex abdominal wall reconstruction
- Similar outcomes to laparoscopic IPOM with the option of fascial closure
5. Emergency Repair (Incarceration/Strangulation)
- General anaesthesia; open approach
- Divide adhesions; reduce contents; assess bowel viability
- Resect non-viable bowel; primary anastomosis
- In contaminated field: avoid synthetic permanent mesh
- Use primary suture repair or biologic mesh
- Definitive mesh repair deferred to elective setting
Summary: Mesh Position Comparison
| Mesh Position | Plane | Recurrence | SSI Risk | Comment |
|---|---|---|---|---|
| Retromuscular (Sublay) | Behind rectus | Lowest | Lowest | Preferred for most cases |
| Onlay | Anterior to fascia | Similar to retromuscular | Higher | Large skin flaps needed |
| Preperitoneal | Behind transversalis | Low | Low | Good alternative |
| Intraperitoneal (IPOM) | Inside peritoneum | Low | Low | Anti-adhesion mesh mandatory |
| Inlay (Bridge) | Between muscle edges | Highest | - | Avoid in elective repair |
Prevention of Incisional Hernia
The best treatment is prevention at the time of original laparotomy closure.
- Small-bite technique for fascial closure (5 mm bites, 5 mm apart; fascia ONLY - no fat or muscle)
- Suture:wound length ratio ≥ 4:1
- Slowly resorbable 2/0 monofilament suture (PDS)
- Drains through separate stab incisions - never through the wound
- Peritoneum does not need to be closed separately (no added strength)
- Consider negative pressure wound therapy or partial skin closure in high-risk contaminated wounds
- Prophylactic mesh in high-risk patients (obese, bariatric surgery patients) - substantially reduces risk
- Prophylactic mesh at stoma formation sites (reduces parastomal hernia rate significantly)
Complications of Incisional Hernia Repair
| Complication | Notes |
|---|---|
| Seroma | Most common; higher with onlay (large flaps); drain placement reduces it |
| Wound infection / SSI | Can lead to mesh infection; most serious complication |
| Mesh infection | May require mesh removal; biologic mesh preferred in contaminated cases |
| Bowel adhesion / obstruction | Risk with intraperitoneal mesh (must use anti-adhesion coating) |
| Bowel erosion / fistula | Rare but serious; bare mesh against bowel |
| Chronic pain | From mesh tacks/fixation sutures |
| Pseudo-recurrence | Mesh bulge after bridging repair without fascial closure (laparoscopic) |
| Recurrence | Higher with: suture-only repair, inlay mesh, inadequate overlap, persistent risk factors |
| Skin necrosis | After large onlay repair with extensive skin flap elevation |
- Bailey and Love's Short Practice of Surgery, 28th Ed., pp. 1098-1102
- Fischer's Mastery of Surgery, 8th Ed., pp. 5842-5913
- Mulholland and Greenfield's Surgery, 7th Ed. (VHWG/EHS Classification)
Anterior ABDOMINAL wall tumor, fnac fibro epithelial neoplasm
anterior abdominal wall tumor FNAC fibroepithelial neoplasm diagnosis management
"abdominal wall" AND "fibroepithelial" AND neoplasm
https://pmc.ncbi.nlm.nih.gov/articles/PMC11131566
"abdominal wall" AND "desmoid" AND fibromatosis
fibroepithelial neoplasm FNAC cytology features benign phyllodes squamous skin tag clinical significance
Anterior Abdominal Wall Tumor - FNAC: Fibroepithelial Neoplasm
Overview: Anterior Abdominal Wall Tumors
- Benign neoplasm: 52.9% (most common - lipoma)
- Non-neoplastic lesions: 30% (abscess, suture granuloma, endometriosis, hematoma)
- Malignant neoplasm: 17.1% (most common - metastatic adenocarcinoma)
Classification of Anterior Abdominal Wall Tumors
A. Non-neoplastic / Benign Inflammatory
| Lesion | Key Features |
|---|---|
| Suture granuloma | History of prior surgery; granulomatous reaction to suture material |
| Abscess / Infected wound | Fluctuant, tender, inflammatory signs |
| Hematoma | Post-trauma or post-surgery; ecchymosis |
| Epidermoid / sebaceous cyst | Superficial, punctum visible, cheesy contents |
| Keloid | At scar site, firm, raised |
| Endometriosis (scar) | In surgical scar (C-section site); cyclical pain/swelling with menstruation |
B. Primary Benign Neoplasms
| Tumor | Notes |
|---|---|
| Lipoma | Most common benign tumour - soft, lobulated, slips away on palpation |
| Fibroma / Desmoid fibromatosis | Firm, deep-seated; locally aggressive |
| Neurofibroma / Schwannoma | Neural sheath origin; may be multiple in NF1 |
| Fibroepithelial polyp (skin tag) | Soft, pedunculated, on skin surface |
| Nodular fasciitis | Reactive fibrous proliferation; rapidly growing; can mimic malignancy |
| Haemangioma / Vascular malformation | Soft, compressible; may increase with Valsalva |
C. Primary Malignant Neoplasms
| Tumor | Notes |
|---|---|
| Desmoid tumor (aggressive fibromatosis) | Locally aggressive; does not metastasize; most common primary abdominal wall "sarcoma-like" |
| Dermatofibrosarcoma protuberans (DFSP) | Low-grade dermal sarcoma; nodular; t(17;22) translocation |
| Liposarcoma | Deep-seated; large; heterogeneous on imaging |
| Leiomyosarcoma / Other sarcomas | Rare; aggressive |
| Melanoma | Superficial origin |
D. Metastatic Tumors (Most Common Malignant Cause)
- Sister Mary Joseph nodule - umbilical metastasis from intra-abdominal primary (gastric, colorectal, ovarian)
- Subcutaneous metastases from breast, colon, stomach, ovarian primaries
- Adenocarcinoma is the most common histotype on FNAC
FNAC of Anterior Abdominal Wall Tumors
Why FNAC?
- Simple, fast, minimally invasive
- Performed at bedside or under USS guidance
- Provides immediate triage: benign vs malignant vs inflammatory
- Can guide decision between conservative management, surgery, chemotherapy, or further biopsy
- Particularly important at the umbilicus - may reveal occult systemic malignancy
Technique
- Patient supine; mass identified clinically ± USS guidance
- 22-23G needle, 10 mL syringe
- 2-3 passes with aspiration; smears prepared immediately
- Air-dried (Diff-Quik/MGG) and alcohol-fixed (Papanicolaou/H&E) stains
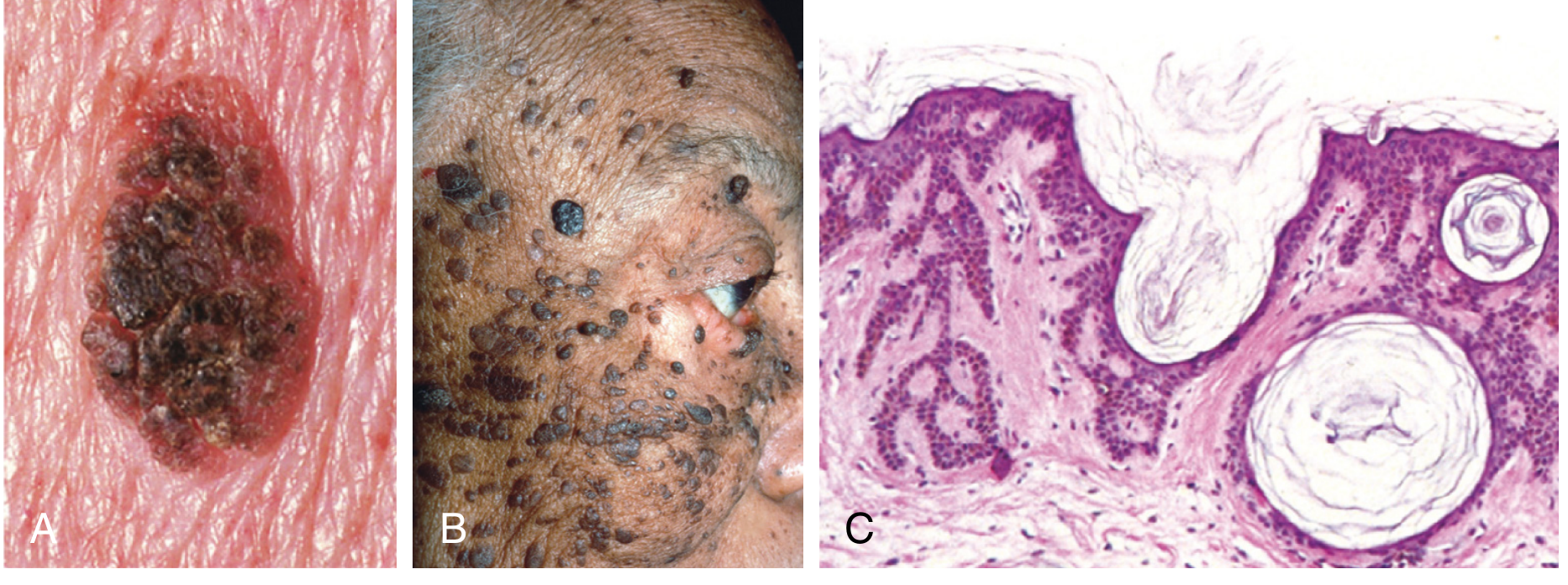
Fibroepithelial Neoplasm on FNAC
1. Fibroepithelial Polyp (Acrochordon / Skin Tag)
"Fibroepithelial polyps are soft, flesh-colored, bag-like tumors that are often attached to the surrounding skin by a slender stalk. They consist of fibrovascular cores covered by benign squamous epithelium."
- Robbins & Cotran Pathologic Basis of Disease
- Most common cutaneous lesion; highly prevalent in middle-aged and older individuals
- Found on neck, trunk, face, intertriginous areas - can occur on abdominal skin
- Soft, pendulous, skin-coloured or hyperpigmented
- Attached by a narrow stalk (pedunculated)
- Become more numerous during pregnancy (hormonal stimulation)
- Associated with: diabetes, obesity, intestinal polyposis
- Fibrovascular core covered by benign squamous (stratified) epithelium
- No atypia; no mitoses; benign cytomorphology
- Can undergo ischaemic necrosis due to torsion (causes pain)
- Sporadic (majority)
- Rare: Birt-Hogg-Dubé syndrome (when combined with perifollicular mesenchyme tumors) - associated with renal neoplasms; genetic counselling needed
2. Phyllodes Tumor (Classic Biphasic Fibroepithelial Neoplasm)
| Feature | Finding |
|---|---|
| Architecture | Large wavy/folded epithelial clusters in leaf-like arrangement |
| Stromal component | Fibromyxoid stromal clumps - characteristic; reduced epithelial:stromal ratio vs fibroadenoma |
| Epithelial cells | Usually benign cytomorphology; occasionally hyperplastic (enlarged vesicular nuclei, small nucleoli) |
| Stromal cells | Fibroblastic pavements; spindle-shaped |
| Atypia | Increased in higher grades; dispersed atypical stromal cells |
| Malignant features | Multinucleated tumour cells; marked stromal anaplasia; ≥10 mitoses/10 HPF |
| Grade | Stromal Hypercellularity | Atypia | Overgrowth | Border | Mitoses |
|---|---|---|---|---|---|
| Benign | Mild | Minimal/None | None | Circumscribed (pushing) | ≤ 4/10 HPF |
| Borderline | Moderate | Moderate | Focal | Focal infiltration | 5-9/10 HPF |
| Malignant | Marked | Marked | Present | Infiltrative (permeative) | ≥ 10/10 HPF |
- Benign/Borderline: Wide local excision with clear margins (≥ 1 cm)
- Malignant: Wide excision ± mastectomy; axillary dissection NOT routine (lymph node metastasis rare)
- Local recurrence risk present in all grades; follow-up essential
- No role for routine adjuvant chemotherapy/radiation in benign phyllodes
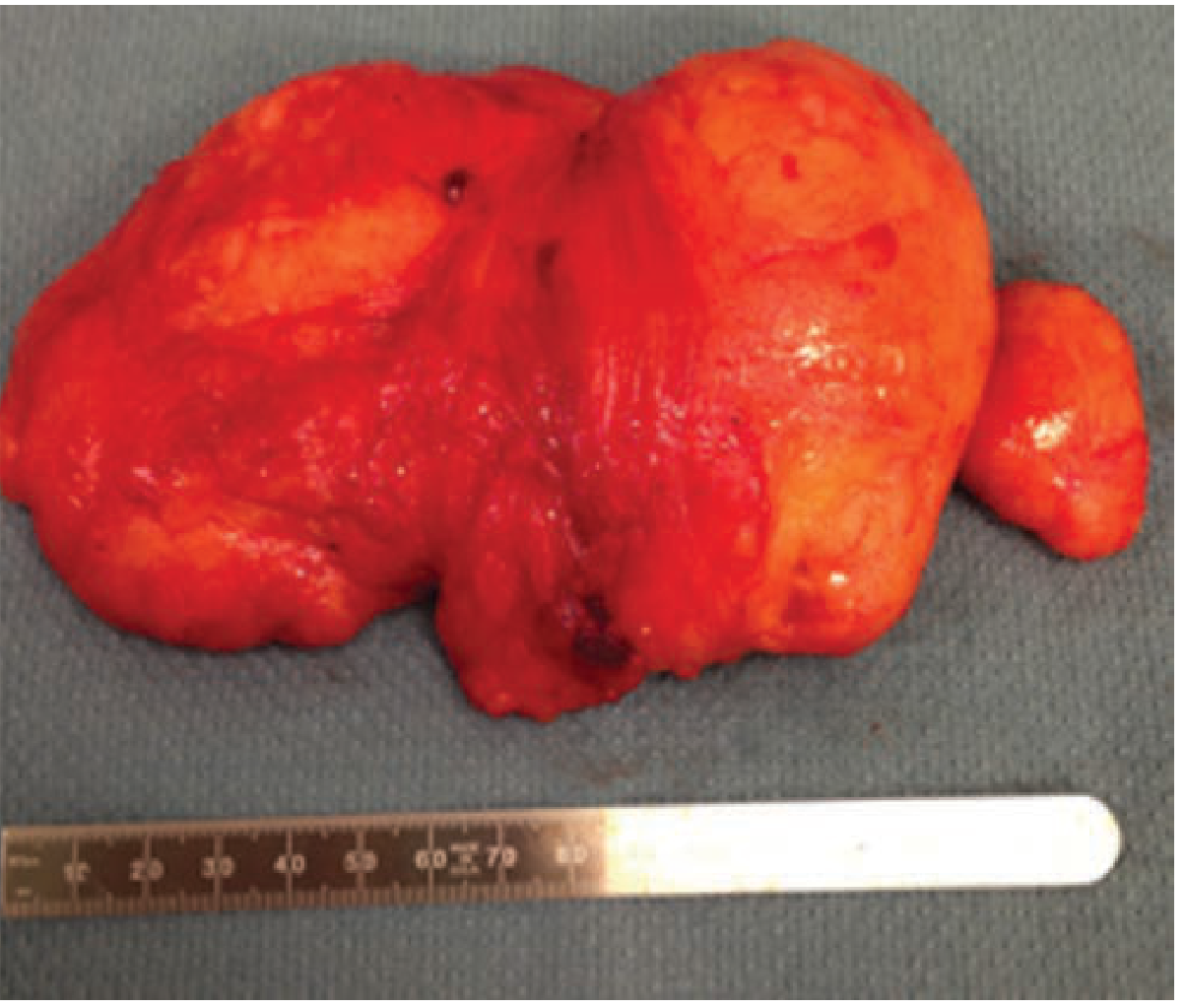
3. Desmoid Tumor (Aggressive Fibromatosis) - The Classic Anterior Abdominal Wall Fibroepithelial/Fibrous Neoplasm
"Desmoid tumors are classically described as an abdominal wall tumor, seen in young women during the postpartum period."
- Mulholland and Greenfield's Surgery, 7th Ed.
- Sporadic cases: Mutations in CTNNB1 (β-catenin gene) - most common
- FAP-associated cases: Germline APC gene mutations; seen in Gardner's syndrome
- Risk factors: pregnancy, prior surgical incision, trauma, hormonal exposure
- 10-15% of FAP patients develop desmoids; after prophylactic colectomy, desmoids become the leading cause of death in FAP
- Deep-seated in muscles/fascial planes
- Firm, smooth mass with surrounding pseudocapsule
- Microscopically: tumour extends BEYOND the pseudocapsule - fibrous septae extend radially (key feature explaining high local recurrence rates)
- Increased oestrogen receptor-β expression in 80%
- Large (> 5 cm), localised, firm mass with indolent growth
- Minimally painful
- Intra-abdominal: mass effect, intestinal obstruction, mucosal ischaemia
- Notoriously infiltrative - microscopically positive margins in a significant number of resections
- Bland-looking fibroblastic spindle cells in collagenous stroma
- Low cellularity; no atypia; no mitoses (can be mistaken for benign fibrous tissue)
- Core needle biopsy preferred for diagnosis (FNAC often non-diagnostic due to scant cellularity)
- β-catenin nuclear positivity on immunohistochemistry - key diagnostic marker
- MRI preferred - best defines extent of disease and invasion into adjacent structures
- CT with IV contrast - defines local extent and chest metastases (important if high-grade component suspected)
Management of Abdominal Wall Desmoid Tumor
Step 1: Active Surveillance (First-line - NCCN recommendation)
- Asymptomatic, non-life-threatening tumors: watchful waiting first
- Periodic MRI scans to monitor
- 29% of desmoids undergo spontaneous regression
- Only 16% require surgery over 3-year follow-up (observational cohort)
Step 2: Medical Therapy (if growing under observation)
| Drug | Mechanism |
|---|---|
| NSAIDs (Sulindac) | β-catenin pathway modulation |
| Tamoxifen / Anti-oestrogens | Oestrogen receptor-β blockade |
| Imatinib | Tyrosine kinase inhibition (moderate evidence) |
| Sorafenib | TKI - active; approved for desmoid in some guidelines |
| Nirogacestat | γ-secretase inhibitor (newer; approved 2023) |
| Methotrexate + Vinblastine | Cytotoxic; for progressive unresectable disease |
| Doxorubicin (pegylated) | For refractory aggressive cases |
| Radiation (50-54 Gy) | Unresectable tumours or post-op recurrence |
Step 3: Surgery (Selective - not first-line)
- Indicated for: symptomatic disease, risk of invasion of vital structures, enlarging tumors failing other treatment, or women with desmoid considering pregnancy
- Margin-negative resection + immediate mesh reconstruction historically gold standard
- However, local recurrence occurs in up to 1/3 of patients regardless of margin status
- Up to 2/3 of patients with positive margins do NOT recur
- Therefore: function-sparing surgery acceptable even with positive margins on critical structures
FNAC Interpretation Algorithm for Abdominal Wall Mass
FNAC Result: "Fibroepithelial Neoplasm"
|
├── Skin surface/superficial, pedunculated:
│ → Fibroepithelial POLYP (skin tag)
│ → Excision; benign
|
├── Breast tissue / ectopic breast / young woman:
│ → Consider PHYLLODES TUMOR
│ → Core biopsy for grading
│ → Wide excision with clear margins
|
├── Deep mass, muscular/fascial plane, young woman,
│ post-partum, or FAP history:
│ → Consider DESMOID FIBROMATOSIS
│ → MRI + core needle biopsy + β-catenin IHC
│ → Active surveillance first
|
└── Atypical stromal cells, increased mitoses,
infiltrative imaging:
→ Consider MALIGNANT PHYLLODES / SARCOMA
→ Multidisciplinary sarcoma centre referral
Summary Table: Key Fibroepithelial Neoplasms of Abdominal Wall
| Feature | Fibroepithelial Polyp | Phyllodes Tumor | Desmoid Fibromatosis |
|---|---|---|---|
| Origin | Skin/epidermis | Breast fibroepithelial | Muscular/aponeurotic |
| Age/Sex | Middle-aged; both | Women 35-55 | Women; young adults |
| Metastasis | No | Rare (malignant grade only) | Never |
| Local recurrence | No | Yes (all grades) | Yes (up to 30%) |
| FNAC yield | Good | Moderate (core biopsy better) | Low (core biopsy preferred) |
| Key FNAC feature | Benign squamous + fibrovascular core | Fibromyxoid stromal clumps + epithelial clusters | Bland spindle cells, collagenous stroma |
| IHC marker | - | CD34+ stromal cells | β-catenin nuclear+ |
| First-line Rx | Excision | Wide excision (clear margins) | Active surveillance |
| Prognosis | Excellent | Good (benign); variable (malignant) | Good; recurrence possible |
- Robbins & Cotran Pathologic Basis of Disease (fibroepithelial polyp)
- Schwartz's Principles of Surgery, 11th Ed. (desmoid tumors, abdominal wall)
- Mulholland & Greenfield's Surgery, 7th Ed. (desmoid fibromatosis classification)
- FNAC spectrum data: PMC11131566