Rickets / Spasmophilia
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Searching Images
rickets radiograph widened metaphysis rachitic rosary bowing
Reading File
Reading File
Loading Image
Loading Image
Rickets / Spasmophilia for childhood diseases
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Searching Images
rickets bowing legs rachitic rosary wrist cupping fraying metaphysis child
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Finding Sources
I now have comprehensive content. Let me compile the full response.
Rickets & Spasmophilia — Childhood Diseases
PART 1 — RICKETS
Definition
Rickets is a metabolic bone disease of growing children resulting from inadequate mineralization of the growth plate (epiphyseal cartilage) and osteoid. It occurs exclusively before epiphyseal plate closure (as opposed to osteomalacia, which is its adult equivalent). The fundamental defect is diminished calcium–phosphate product in the extracellular fluid around developing growth plates, disrupting normal chondrocyte maturation, apoptosis, and scaffold mineralization.
Pathophysiology
Normal growth plate: Chondrocytes in the resting zone mature, organize into longitudinal columns, hypertrophy, undergo apoptosis, and mineralize — providing a scaffold for osteoclast remodeling.
In rickets: Low extracellular Ca²⁺ × PO₄³⁻ disrupts chondrocyte apoptosis → disorganized, expanded, hypomineralized growth plate → classic radiologic findings.
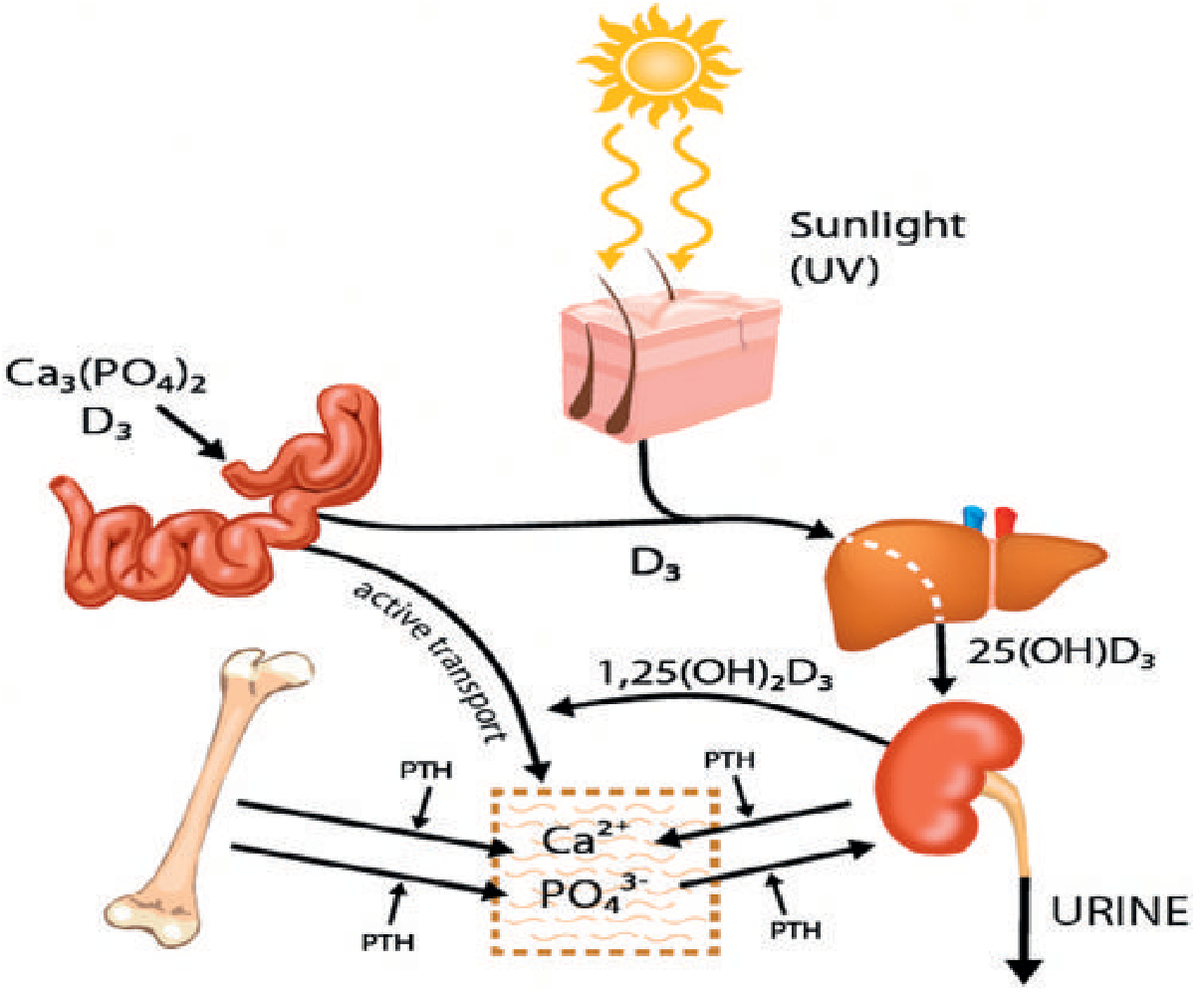
Key metabolic changes in rickets:
- Phosphate is greatly depressed (PTH increases renal phosphate excretion)
- Calcium is only slightly depressed (PTH compensates via osteoclastic resorption)
- When bone calcium stores are finally exhausted → rapid hypocalcemia → tetany
Etiology / Classification
| Type | Mechanism | Key Features |
|---|---|---|
| Nutritional (vitamin D–deficient) | Inadequate sun exposure or dietary deficiency | Most common; responds rapidly to vitamin D supplementation |
| Vitamin D–Dependent Type 1 | AR; deficient renal 1α-hydroxylase (impaired 2nd hydroxylation) | Presents <2 yrs; severe bony changes; hypocalcemic tetany/seizures |
| Vitamin D–Dependent Type 2 | AR; defective vitamin D receptor (VDR) on target organs | Presents <1 yr; associated with alopecia and poor dentition |
| Vitamin D–Resistant (X-linked hypophosphatemic) | X-linked dominant mutation in PHEX gene; impaired proximal renal tubular phosphate reabsorption | Normal/elevated 25-OHD; severe bowing, short stature, dental abnormalities |
| Renal Osteodystrophy | CKD → failure of renal 1α-hydroxylation; phosphate retention → secondary hyperparathyroidism | Elevated ALP & PO₄; features of both rickets and hyperparathyroidism on X-ray |
| Tumor-induced (oncogenic) | Tumors secrete FGF-23 (phosphaturic); excess phosphate wasting | Normal Ca²⁺; elevated ALP; cure with tumor resection |
| Fanconi syndrome / renal tubular acidosis | Proximal tubular dysfunction → phosphate, glucose, amino acid wasting | Systemic acidosis accelerates demineralization |
Congenital rickets (at birth due to maternal vitamin D deficiency) is rare — vitamin D is preferentially diverted from mother to fetus.
Clinical Features
Skeletal signs (from Fitzpatrick's Dermatology):
- Rachitic rosary — beaded enlargement of the costochondral junctions (anterior rib ends)
- Craniotabes — softening of skull bones (ping-pong ball feel on palpation)
- Frontal bossing — prominence of frontal bones
- Widening of wrists — metaphyseal expansion; clinically palpable
- Lateral bowing of lower extremities (genu varum / genu valgum) — bones too soft to bear weight
- Harrison's sulcus — costophrenic depression from diaphragmatic pull on softened ribs
- Scoliosis, kyphosis
- Short stature
- Dental defects, delayed eruption
Systemic signs:
- Hypotonia
- Fractures (only in children with radiographic rickets)
- Dilated cardiomyopathy (rare but potentially fatal — vitamin D-responsive)
- Hypocalcemic seizures or tetany (rare, in advanced disease)

Radiologic Findings
Growth plate / metaphysis:
- Widening, cupping, and fraying of metaphyses (distal radius/ulna, distal femur, proximal tibia are most prominent)
- Loss of the sharp zone of provisional calcification
- Widened, irregular growth plates
General:
- Generalized osteopenia, thinned cortices
- Looser zones (pseudofractures) — transverse lucent bands at sites of stress (pubic rami, medial femoral neck, posterior ulna, axillary scapula, ribs)
- Bowing of long bones
- Irregular vertebral end plates

Biochemistry Summary
| Parameter | Nutritional Rickets | VD-Resistant Rickets | Renal Osteodystrophy |
|---|---|---|---|
| Ca²⁺ | Low/normal | Normal | Low/normal |
| PO₄³⁻ | ↓↓ | ↓↓ | ↑ |
| ALP | ↑ | ↑ | ↑ |
| PTH | ↑ (secondary) | Normal | ↑↑ (secondary) |
| 25-OH-D | ↓ | Normal/↑ | Low |
| 1,25-(OH)₂D | ↓ | Low (Type 1) / Normal (Type 2) | ↓ |
Laboratory screening: serum Ca²⁺, PO₄³⁻, alkaline phosphatase, 25-OH vitamin D, PTH. Definitive diagnosis of osteomalacia requires undecalcified bone biopsy (widened osteoid seams).
Treatment
Nutritional rickets (vitamin D–deficient):
- Prophylaxis: 400 IU/day in breastfed infants and those on unfortified formula
- Treatment (established disease): 1,000 IU/day → normalizes Ca²⁺/PO₄ in ~10 days, radiographic healing ~3 weeks
- More rapid healing: 3,000–4,000 IU/day (especially if thoracic rickets compromises respiration)
- Harriet Lane doses: 2,000–5,000 IU/day × 6–12 weeks (normal GI absorption)
Vitamin D–resistant rickets (X-linked hypophosphatemic):
- Phosphate supplementation + high-dose vitamin D
- Child: initial 40,000–80,000 IU/day ergocalciferol, increase by 10,000–20,000 IU every 3–4 months as needed
- Burosumab (anti-FGF-23 monoclonal antibody) — newer targeted therapy for XLH
Renal rickets / CKD-MBD:
- Active form calcitriol (1,25-(OH)₂D₃) bypasses dysfunctional renal hydroxylation
- Phosphate restriction + phosphate binders
PART 2 — SPASMOPHILIA
Definition & Concept
Spasmophilia (also called latent tetany or normocalcemic tetany) refers to a state of increased neuromuscular excitability in which clinical signs of tetany can be provoked even without overt hypocalcemia. In classical European/francophone pediatrics, it is recognized as a distinct clinical entity — a condition considered a physical disease in France but less recognized as a nosological entity in Anglo-American medicine.
Spasmophilia is closely linked to rickets because rickets-associated hypocalcemia is a major underlying trigger in infancy and childhood.
Pathophysiology of Tetany
Tetany results from decreased ionized calcium in extracellular fluid → reduced threshold for nerve membrane depolarization → spontaneous or easily provoked action potentials → muscle hyperactivity.
Causes of hypocalcemia / tetany in children:
- Vitamin D deficiency rickets (most common)
- Hypoparathyroidism (post-surgical, DiGeorge syndrome)
- Neonatal hypocalcemia (PTH deficiency, maternal hyperparathyroidism causing neonatal parathyroid suppression)
- Hypomagnesemia (blocks PTH release and causes PTH resistance)
- Alkalosis (respiratory or metabolic) — decreases ionized Ca²⁺ without changing total calcium
- Pseudohypoparathyroidism
Tetany in rickets specifically: In early rickets, PTH maintains near-normal calcium by mobilizing bone stores. Tetany only occurs when bone calcium is exhausted and blood calcium falls below 7 mg/dL — at which point the child is at risk of fatal tetanic respiratory spasm.
Clinical Forms
| Form | Description |
|---|---|
| Manifest (overt) tetany | Spontaneous carpopedal spasm, laryngospasm, generalized muscle cramps, seizures |
| Latent tetany / spasmophilia | Increased excitability without spontaneous spasm; elicited only by provocation tests |
Clinical Signs of Latent Tetany (Spasmophilia)
Chvostek's sign:
- Tap the facial nerve just anterior to the ear (near the temporomandibular joint)
- Positive: ipsilateral contraction of facial muscles (eye, mouth, nose)
- Present in up to 10–25% of normals → less specific
- A useful screening sign in infants at risk
Trousseau's sign:
- Inflate a blood pressure cuff above systolic pressure for 3 minutes
- Positive: carpal spasm (flexion of wrist and MCP joints, extension of IP joints, thumb adduction — "obstetrician's hand")
- More specific for hypocalcemia than Chvostek
- Confirmation requires ionized calcium measurement
Other symptoms of neuromuscular irritability:
- Circumoral and distal paresthesias (tingling)
- Perioral numbness
- Muscle cramps
- Laryngospasm (inspiratory stridor — dangerous)
- Bronchospasm
- Seizures (in severe hypocalcemia)
ECG change: Prolonged QT interval (due to slow ventricular repolarization with low Ca²⁺)
Mental/behavioral changes: Irritability, anxiety, emotional lability, confusion (in severe/chronic cases)
Relationship Between Rickets and Spasmophilia
Vitamin D deficiency
↓
↓ Intestinal Ca²⁺ absorption
↓
↑ PTH (secondary hyperparathyroidism)
↓
Osteoclastic bone resorption maintains serum Ca²⁺ (temporarily)
↓
Bone calcium exhausted (late rickets)
↓
Serum Ca²⁺ < 7 mg/dL
↓
TETANY / SPASMOPHILIA
In the early stages of rickets, tetany is rare because PTH compensates. In advanced rickets, when bones are depleted, hypocalcemia can become severe and life-threatening.
Diagnosis
| Test | Finding |
|---|---|
| Serum ionized Ca²⁺ | Low (<1.1 mmol/L or total Ca²⁺ <8 mg/dL) |
| Total serum calcium | <8 mg/dL (consider albumin correction) |
| Serum phosphate | Low (nutritional rickets), high (hypoparathyroidism) |
| 25-OH Vitamin D | Low in nutritional rickets |
| PTH | Elevated (secondary) in rickets; low in hypoparathyroidism |
| ALP | Elevated in active rickets |
| Serum magnesium | Rule out hypomagnesemia as cause |
| ECG | Prolonged QT interval |
| Chvostek / Trousseau | Positive (latent tetany) |
Treatment of Spasmophilia / Hypocalcemic Tetany
Acute overt tetany (emergency):
- IV calcium gluconate — immediate relief of tetanic spasm
- Relieves laryngospasm and respiratory crisis
- Followed by oral supplementation
Latent tetany / underlying rickets:
- Treat the underlying cause (vitamin D supplementation ± calcium)
- Oral calcium supplementation
- Monitor Ca²⁺ × PO₄ product (keep <70 mg²/dL² to avoid ectopic calcification)
Monitoring (Harriet Lane): Serum Ca²⁺, PO₄, 25-OH-D (target ≥20 ng/mL in children), ALP. Titrate to clinical response.
Summary Table
| Feature | Rickets | Spasmophilia |
|---|---|---|
| Age | Infants, toddlers, school-age | Infants, young children |
| Primary cause | Vitamin D/Ca/PO₄ deficiency | Hypocalcemia (often from rickets) |
| Key skeletal sign | Rachitic rosary, bowing, cupping | No specific skeletal sign |
| Key neurological sign | Late tetany (bone-depleted) | Chvostek + Trousseau (latent) |
| X-ray | Widened/cupped/frayed metaphyses | Normal |
| Lab | ↓PO₄, ↑ALP, ↓25-OHD, ↑PTH | ↓Ca²⁺ ionized, prolonged QT |
| Emergency | Tetanic respiratory spasm | Laryngospasm, seizure |
| Treatment | Vitamin D ± calcium | IV Ca²⁺ gluconate (acute) + vitamin D |
Sources: Guyton & Hall Textbook of Medical Physiology; Grainger & Allison's Diagnostic Radiology; Fitzpatrick's Dermatology; Goodman & Gilman's Pharmacological Basis of Therapeutics; Harriet Lane Handbook (23rd ed.); Miller's Review of Orthopaedics; Robbins, Cotran & Kumar Pathologic Basis of Disease; National Kidney Foundation Primer on Kidney Diseases; Henry's Clinical Diagnosis by Laboratory Methods.
This is a shared conversation. Sign in to Orris to start your own chat.