inner ear fluids in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Searching PubMed
endolymph perilymph inner ear fluid homeostasis
Finding Sources
Searching PubMed
endolymph perilymph homeostasis cochlea
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Searching PubMed
aquaporin inner ear endolymph Meniere disease
Loading Image
INNER EAR FLUIDS
A Comprehensive 20-Mark Answer (RGUHS Standard)
OVERVIEW AND INTRODUCTION
The inner ear contains two distinct fluid compartments separated by specialized epithelial barriers: perilymph (filling the bony labyrinth) and endolymph (filling the membranous labyrinth). A third fluid, the intrastrial fluid, is now recognized as a functionally distinct compartment within the stria vascularis. These fluids are essential for mechanoelectrical transduction (MET) in the cochlea and for vestibular mechanosensation.
"The bony channels are filled with perilymph, which surrounds the membranous canals. Perilymph is essentially a typical extracellular fluid, similar, but not identical, to cerebrospinal fluid (CSF) or serum." — Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2, Ch. 47 (Gale & Forge)
1. ANATOMICAL COMPARTMENTS
BONY LABYRINTH
├── Scala Vestibuli ──────────────── PERILYMPH (High Na+, Low K+)
│ │ (communicates via helicotrema)
├── Scala Tympani ──────────────── PERILYMPH (High Na+, Low K+)
│
MEMBRANOUS LABYRINTH
├── Scala Media (Cochlear Duct) ─── ENDOLYMPH (High K+, Low Na+, +80 mV EP)
├── Saccule ────────────────────── ENDOLYMPH
├── Utricle ────────────────────── ENDOLYMPH
├── Semicircular Canal Ducts ─────── ENDOLYMPH
└── Endolymphatic Duct & Sac ─────── Resorption of Endolymph
The scala vestibuli and scala tympani communicate at the apex of the cochlea through the helicotrema and both contain perilymph. They are separated from the scala media (endolymph) by:
- Reissner's membrane (roof) - superiorly
- Basilar membrane (floor) - inferiorly
2. IONIC COMPOSITION
Table: Comparison of Inner Ear Fluids
(From Shambaugh Surgery of the Ear, Table 4-2, adapted from Lang et al.)
| Ion / Parameter | Cochlear Perilymph | Cochlear Endolymph | Plasma / CSF |
|---|---|---|---|
| Na⁺ (mM) | 148 | 1.3 | 140 |
| K⁺ (mM) | 4.2 | 157 | 4.5 |
| Cl⁻ (mM) | 119 | 132 | 103 |
| HCO₃⁻ (mM) | 21 | 31 | 24 |
| Ca²⁺ (mM) | 1.3 | 0.023 (very low) | 2.4 |
| pH | 7.3 | 7.5 | 7.4 |
| Electrical potential | 0 mV (reference) | +80 mV (EP) | - |
| Protein | ~200 mg/dL | ~40 mg/dL | trace |
Key points:
- Endolymph is the only extracellular fluid with high K⁺ and low Na⁺ (resembles intracellular fluid)
- The very low Ca²⁺ in endolymph is critical for tip-link integrity in stereocilia
- The +80 mV endocochlear potential (EP) is unique to cochlear endolymph; vestibular endolymph has ~0 mV
3. PERILYMPH
A. Definition and Origin
Perilymph is the extracellular fluid filling the scala vestibuli and scala tympani. It closely resembles CSF and extracellular fluid in composition.
B. Sources of Perilymph (Flowchart)
SOURCES OF PERILYMPH
│
┌────────────────┼─────────────────┐
▼ ▼ ▼
Blood plasma CSF via Local secretion by
(ultrafiltration cochlear fibrocytes of
via vessels) aqueduct spiral ligament
│ │ │
└────────────────┴─────────────────┘
│
PERILYMPH (High Na+, Low K+)
│
Fills scala vestibuli
and scala tympani
- Primary source: Ultrafiltration from blood vessels in the spiral ligament and cochlear capsule
- Secondary source: Possible contribution from CSF via the cochlear aqueduct (however, the exact compositions differ, indicating local modification)
- The cochlear aqueduct connects the scala tympani perilymph with the subarachnoid space; this is why meningitis can affect the inner ear
"The perilymphatic compartment connects with the arachnoid space of the brain via the cochlear aqueduct... indicating that perilymph is produced or at least significantly modified locally in the inner ear." — Scott-Brown's, Vol. 2, Ch. 47
C. Drainage of Perilymph
- Via cochlear aqueduct to CSF
- Possible absorption by fibrocytes of the spiral ligament
4. ENDOLYMPH
A. Definition and Unique Properties
Endolymph fills the membranous labyrinth and is the most unique extracellular fluid in the body - it has an ionic composition resembling intracellular fluid (high K⁺, low Na⁺) and a high positive electrical potential (+80 mV in cochlea).
B. Production of Endolymph
ENDOLYMPH PRODUCTION
│
┌──────────┴──────────┐
▼ ▼
COCHLEAR ENDOLYMPH VESTIBULAR ENDOLYMPH
(Scala media) (Utricle/Saccule/SCC)
│ │
▼ ▼
STRIA VASCULARIS DARK CELLS of vestibular
(primary secretory epithelium (utricle/SCC
organ for K+) ampullae)
Stria Vascularis - The Engine of Endolymph Production
The stria vascularis is a 3-layered, highly vascularized structure on the lateral wall of the scala media:
STRIA VASCULARIS LAYERS:
┌─────────────────────────────────────────────┐
│ MARGINAL CELLS ← face Scala Media │
│ (secrete K+ into endolymph via KCNQ1/KCNE1)│
├─────────────────────────────────────────────┤
│ INTRASTRIAL COMPARTMENT │
│ (fluid: +100 mV, low K+) │
│ + Intermediate cells (KCNJ10 channel) │
│ + Blood vessels │
├─────────────────────────────────────────────┤
│ BASAL CELLS ← face Perilymph/Spiral lig. │
│ (tight junctions + gap junctions) │
└─────────────────────────────────────────────┘
"The stria vascularis plays a pivotal role in cochlear homeostasis by generating the endocochlear potential and maintaining the unique ion composition of the endolymph." — Shambaugh Surgery of the Ear, p. 102
C. Absorption/Drainage of Endolymph
ENDOLYMPH DRAINAGE / RESORPTION
│
┌─────┴──────┐
▼ ▼
ENDOLYMPHATIC REISSNER'S MEMBRANE
SAC (minor role - bidirectional
(primary site transport of ions & water)
of resorption)
│
▼
Endolymphatic duct → Endolymphatic sac
(projects into posterior cranial fossa,
under the dura)
│
▼
Resorption of ions, fluid, and immune
surveillance of endolymph
The endolymphatic sac contains two zones:
- Rugose (proximal) portion: heavily folded, with large phagocytic cells - active resorption
- Smooth (distal) portion: less folded, immunologically active
5. THE ENDOCOCHLEAR POTENTIAL (EP) AND K⁺ RECYCLING
The Endocochlear Potential
The EP is +80 mV inside the scala media relative to perilymph. This is generated and maintained by the stria vascularis.
The driving force for K⁺ entry into hair cells = EP (+80 mV) + resting hair cell potential (-45 mV) = ~130 mV - an enormous driving force.
"Hearing threshold increases approximately 1 dB per mV loss of endocochlear potential." — Shambaugh Surgery of the Ear, p. 103
The K⁺ Recycling Pathway (The "Potassium Cycling Model")
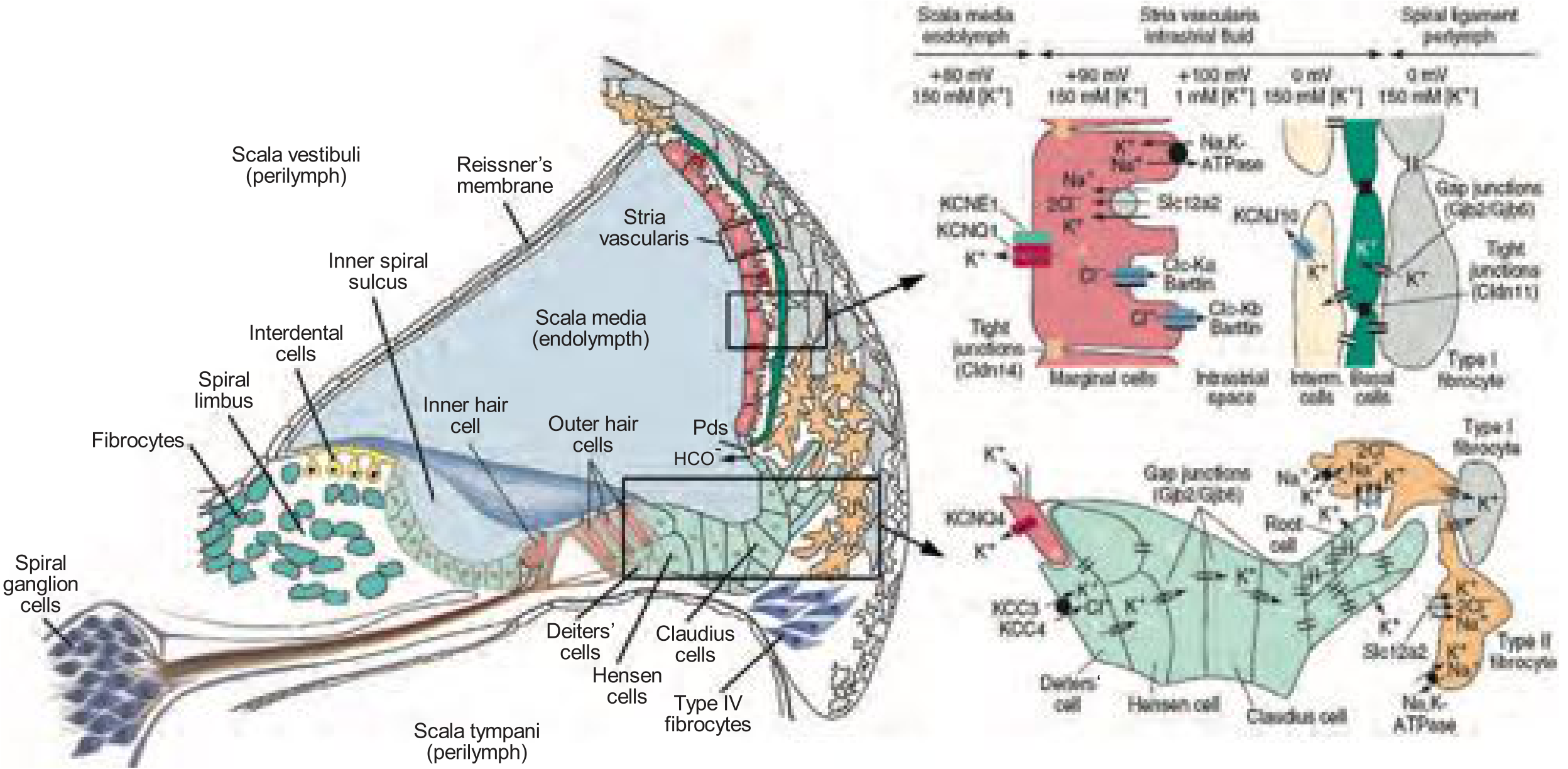
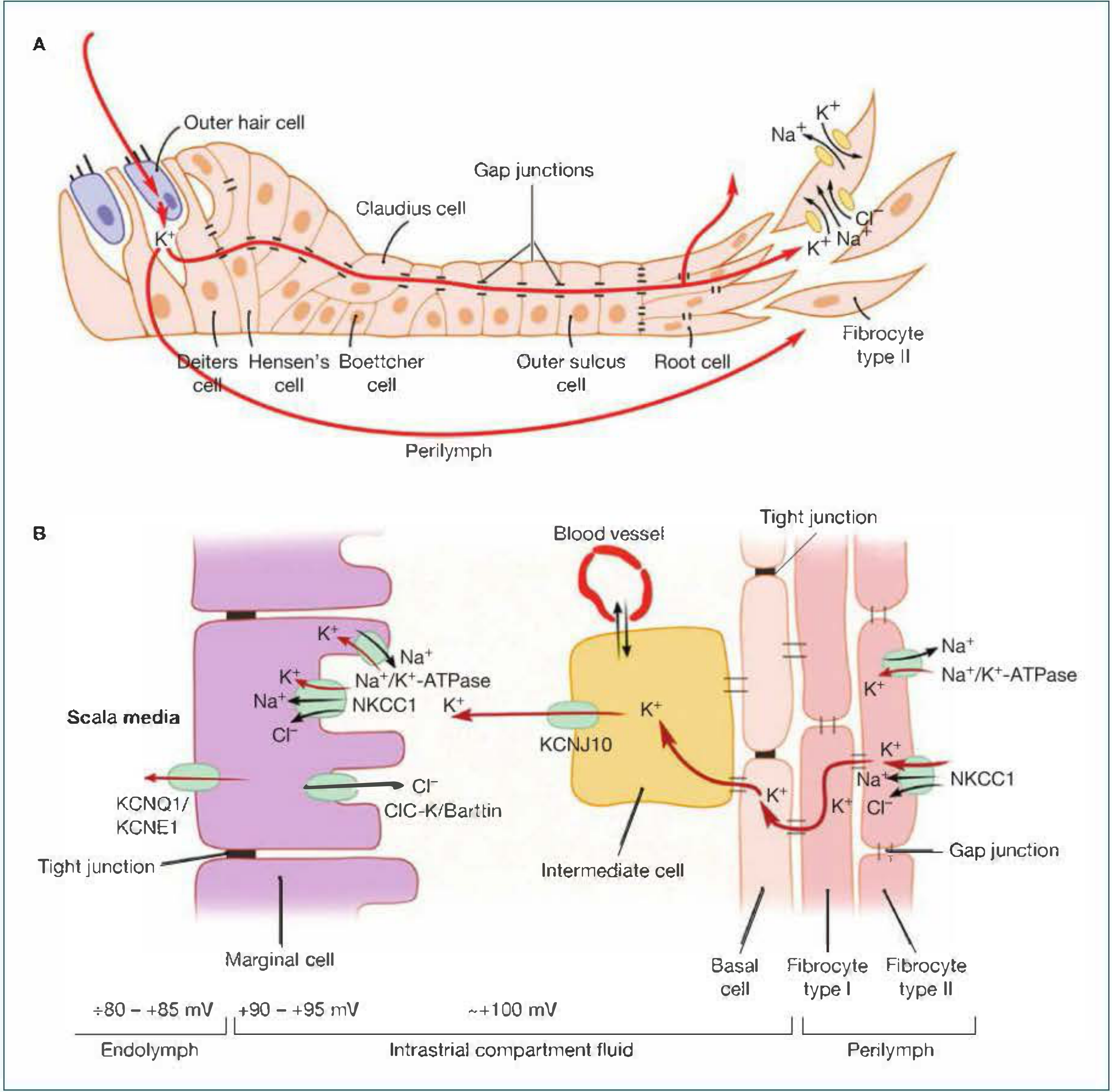
K+ RECYCLING FLOWCHART (Potassium Cycling Model)
ENDOLYMPH (Scala media, +80 mV, [K+] = 157 mM)
│
│ K+ enters hair cell via
│ MET channels at stereocilia tips
▼
HAIR CELL (depolarization)
│
│ K+ exits basolateral membrane
│ via KCNQ4 channels
▼
PERILYMPH (Scala tympani)
│
┌───┴───────────────────────┐
▼ ▼
PATHWAY A: PATHWAY B:
Perilymphatic space Epithelial gap junction network:
(minor) Deiters' cells → Hensen's cells →
Claudius cells → Root cells
│
KCC3/KCC4 cotransporters take up K+
│
▼
SPIRAL LIGAMENT fibrocytes
(Type II fibrocytes take up K+
via Na/K-ATPase and NKCC1)
│
Connective tissue gap junction
network (Cx26, Cx30, Cx31, Cx43)
│
▼
STRIA VASCULARIS (Basal → Intermediate cells)
│
INTERMEDIATE CELLS
(KCNJ10 releases K+ into intrastrial space)
│
▼
INTRASTRIAL SPACE (+100 mV, low K+)
│
MARGINAL CELLS take up K+ via:
• NKCC1 (Na+/K+/2Cl- cotransporter)
• Na+/K+-ATPase (ATP1A1, ATP1B1, ATP1B2)
│
▼
K+ secreted into SCALA MEDIA
via KCNQ1/KCNE1 channels
(apical surface of marginal cells)
│
▼
ENDOLYMPH [K+] maintained at 157 mM
Endocochlear potential = +80 mV
"K+ is efficiently removed from the intrastrial space by marginal cells, which actively take up K+ via NKCC1 (Na+/K+/2Cl−) cotransporters and by Na+/K+-ATPases. Finally, marginal cells secrete K+ into the scala media via the KCNQ1/KCNE1 K+ channel." — Shambaugh Surgery of the Ear, p. 103
6. ION TRANSPORTERS AND CHANNELS - SUMMARY TABLE
| Protein | Gene | Location | Function |
|---|---|---|---|
| KCNQ4 | KCNQ4 | Hair cell basolateral | K⁺ exit from hair cells |
| KCC3, KCC4 | SLC12A6/7 | Deiters' cells | K⁺-Cl⁻ cotransport into supporting cells |
| NKCC1 | SLC12A2 | Marginal cells, Type II fibrocytes | Na⁺-K⁺-2Cl⁻ cotransport |
| Na⁺/K⁺-ATPase | ATP1A1, ATP1B1 | Marginal cells, fibrocytes | Maintains Na⁺/K⁺ gradients |
| KCNJ10 | KCNJ10 | Intermediate cells | K⁺ release into intrastrial space → EP generation |
| KCNQ1/KCNE1 | KCNQ1/KCNE1 | Marginal cell apical | K⁺ secretion into endolymph |
| ClC-Ka/Kb + Barttin | BSND | Marginal cells | Cl⁻ recycling to intrastrial space |
| Connexin 26 | GJB2 | Supporting cells, fibrocytes | Gap junction - K⁺ recycling network |
| Connexin 30 | GJB6 | Supporting cells, fibrocytes | Gap junction - K⁺ recycling network |
| Aquaporin 2 | AQP2 | Endolymphatic sac epithelium | Water transport (vasopressin-regulated) |
| Aquaporin 4 | AQP4 | Perilymphatic tissues | Transmembranous water movement |
| Pendrin | SLC26A4 | Spiral ligament, endolymphatic sac | Cl⁻/HCO₃⁻ exchanger - pH/volume regulation |
"Homeostatic mechanisms that involve the maintenance of separate endolymphatic and perilymphatic compartments... are essential for normal auditory function. Numerous mutant genes that alter homeostasis and are responsible for hereditary hearing impairments have been identified." — Cummings Otolaryngology 7th Ed., Fig. 148.19-148.20
7. GENETIC DISORDERS OF INNER EAR FLUID HOMEOSTASIS
| Syndrome | Gene | Defect | Effect |
|---|---|---|---|
| Jervell & Lange-Nielsen | KCNQ1, KCNE1 | Marginal cell K⁺ secretion | SNHL + prolonged QT |
| DFNB1 (most common AR SNHL) | GJB2 (Cx26) | Gap junction K⁺ recycling | Prelingual SNHL |
| DFNB1B | GJB6 (Cx30) | Gap junction K⁺ recycling | SNHL |
| Bartter Syndrome type IV | BSND (Barttin) | Cl⁻ channel - intrastrial | SNHL + renal tubular acidosis |
| Pendred Syndrome | SLC26A4 | Pendrin - Cl⁻/HCO₃⁻ | SNHL + goitre + EVA |
| DFNA2 | KCNQ4 | Hair cell K⁺ exit | Adult-onset SNHL |
| Enlarged Vestibular Aqueduct (EVA) | SLC26A4 | Pendrin defect | Fluctuating SNHL |
8. ENDOLYMPH VOLUME REGULATION AND FLOW
Two Historical Theories:
- Longitudinal flow theory: Endolymph flows from the cochlear duct apically and drains into the endolymphatic sac. Favored historically.
- Radial flow theory: Local production and absorption balanced radially.
Current Understanding:
"Today, the prevailing thought is that there is no significant volume flow under physiological conditions. Experiments in animals have shown that markers iontophoresed into the endolymph without volume disturbance move solely by diffusion. The ions in the endolymph, therefore, turn over locally without concomitant volume flow." — Shambaugh Surgery of the Ear, p. 103
Role of Aquaporins in Volume Regulation:
WATER TRANSPORT IN INNER EAR
Vasopressin (ADH)
│
▼
AQP2 in endolymphatic sac
(membrane expression increases)
│
▼
Increased water resorption
from endolymph → normal volume
│
(If vasopressin pathologically elevated)
▼
Excessive water retention → ENDOLYMPHATIC HYDROPS
(morphological basis of Ménière's disease)
- AQP2: In endolymphatic sac, regulated by vasopressin (AVP) - key for volume regulation
- AQP4: In perilymphatic tissues; knockout mice show hearing impairment
- AQP10, AQP11, AQP12: Recently identified in rat stria vascularis (Ichikawa et al., Acta Otolaryngol 2024, PMID 38511591)
9. VESTIBULAR ENDOLYMPH vs. COCHLEAR ENDOLYMPH
| Feature | Cochlear Endolymph | Vestibular Endolymph |
|---|---|---|
| Electrical potential (EP) | +80 mV | ~0 mV (same as perilymph) |
| K⁺ concentration | 157 mM | ~150 mM (similar) |
| Na⁺ concentration | 1.3 mM | ~15 mM (slightly higher) |
| Ca²⁺ concentration | Very low (0.023 mM) | Higher (~0.25 mM) |
| Secretory organ | Stria vascularis | Dark cells (utricle/ampullae) |
| Role of Ca²⁺ | Tip-link regulation in cochlea | Otolith membrane (CaCO₃) calcification |
10. THE ENDOLYMPHATIC SAC - STRUCTURE AND FUNCTION
The endolymphatic sac (ELS) is the terminal dilation of the endolymphatic duct, lying under the dura of the posterior cranial fossa.
ENDOLYMPHATIC SAC FUNCTIONS
│
┌──────┼──────┬──────────┐
▼ ▼ ▼ ▼
FLUID ION IMMUNE PRESSURE
RESORB- REGUL- SURVEIL- SENSOR
TION ATION LANCE
│ │ │ │
AQP2 Na+ / IgA, IgG Responds to
Cl- H+ phagocytic changes in
transport exchange cells endolymph
present volume
- Destruction/dysfunction of ELS → endolymphatic hydrops → Ménière's disease
- ELS contains IgA secreting cells and macrophages (immune role)
- Surgical decompression/shunting of ELS is a treatment for intractable Ménière's disease
11. CLINICAL RELEVANCE - FLOWCHART
INNER EAR FLUID DISTURBANCES
│
┌─────┴──────┐
▼ ▼
ENDOLYMPH PERILYMPH
DISTURBANCE DISTURBANCE
│ │
▼ ▼
ENDOLYMPHATIC PERILYMPH
HYDROPS FISTULA
│ │
▼ ▼
Ménière's disease Trauma / barotrauma
(Fluctuating SNHL, • Oval/round window
vertigo, tinnitus, fistula
aural fullness) • Fluctuating SNHL
│ • Perilymph behind
▼ TM (sign)
Treatment:
• Diuretics (↓ endolymph)
• Salt restriction
• Betahistine
• ELS surgery
• Intratympanic dexamethasone/
gentamicin
12. REISSNER'S MEMBRANE
- A thin two-layered membrane separating scala vestibuli (perilymph) from scala media (endolymph)
- Inner layer: Simple squamous epithelium (faces endolymph) - contains Na⁺/K⁺-ATPase, ion channels
- Outer layer: Mesothelial cells (faces perilymph)
- Functions:
- Maintains the electrolyte barrier between endolymph and perilymph
- Active ion transport (Na⁺ and Cl⁻ from endolymph to perilymph)
- Contributes to endolymph volume regulation
13. RECENT ADVANCES (2021-2026)
1. Aquaporin Subtypes in Stria Vascularis
Ichikawa R et al. (2024) - [Acta Otolaryngol PMID 38511591] reported the expression of AQP10, AQP11, and AQP12 in the rat stria vascularis, expanding our knowledge of water channel diversity in endolymph regulation. These had not previously been characterized in the inner ear.
2. Endolymph Proteomics
Fukuda M et al. (2024) - [iScience PMID 39563888] published a comprehensive protein profile of mouse endolymph, identifying proteins involved in controlling cochlear homeostasis. The proteome differs significantly from perilymph and suggests active secretory roles beyond simple K⁺ transport.
3. Vasopressin-AQP2 Axis in Ménière's Disease
Mom R et al. (2022) - [Biomolecules PMID 35454100] investigated dexamethasone as a direct modulator of AQP2, providing a molecular rationale for intratympanic steroid therapy in Ménière's disease via endolymphatic sac AQP2 regulation.
4. Cell and Gene Therapy for Inner Ear Fluid Disorders
Fankhauser V & Kempfle JS (2026) - [HNO PMID 42307737] reviewed emerging cell and gene therapy approaches for Ménière's disease, targeting genes in the K⁺ recycling pathway and endolymphatic sac function.
5. Potassium Channel Pharmacology
Emerging research targets KCNQ1/KCNE1 and KCNJ10 channels as therapeutic targets to modulate the endocochlear potential in noise-induced and age-related hearing loss.
SUMMARY DIAGRAM
INNER EAR FLUID COMPARTMENTS - COMPLETE OVERVIEW
┌─────────────────────────────────────┐
│ MEMBRANOUS LABYRINTH │
│ │
BONY LABYRINTH │ ┌─────────────────────────────┐ │
(Perilymph) │ │ ENDOLYMPH │ │
High Na+, Low K+ │ │ High K+ (157 mM) │ │
~0 mV │ │ Low Na+ (1.3 mM) │ │
│ │ Low Ca²+ (0.023 mM) │ │
Source: │ │ +80 mV (EP) │ │
• Blood │ │ │ │
ultrafiltrate │ │ Source: │ │
• CSF via │ │ • Stria vascularis │ │
cochlear │ │ (cochlea) │ │
aqueduct │ │ • Dark cells (vestibule) │ │
• Spiral │ │ │ │
ligament │ │ Drainage: │ │
│ │ • Endolymphatic sac │ │
Drainage: │ │ (main) │ │
• Cochlear │ │ • Reissner's membrane │ │
aqueduct │ │ (minor) │ │
• Fibrocytes │ └─────────────────────────────┘ │
└─────────────────────────────────────┘
KEY BARRIER: Tight junctions of epithelial cells lining membranous labyrinth
KEY GENERATOR: Stria vascularis (KCNJ10 + KCNQ1/KCNE1 + Na/K-ATPase + NKCC1)
KEY RECYCLER: Gap junction networks (Connexins 26, 30, 31, 43)
KEY REGULATOR: Endolymphatic sac (AQP2 + vasopressin axis)
REFERENCES (RGUHS Preferred Sources)
| Source | Contribution to this topic |
|---|---|
| Scott-Brown's Otorhinolaryngology HNS, 8th Ed., Vol. 2, Ch. 47 (Gale & Forge) | Endolymph/perilymph composition, epithelial barriers, hair cell biology |
| Cummings Otolaryngology HNS, 7th Ed., Ch. 148 | Endolymph homeostasis, K⁺ recycling, connexins, gap junctions, genetic hearing loss |
| Shambaugh Surgery of the Ear | Ionic composition table (Table 4-2), stria vascularis, K⁺ circulation (Figs 4-6, 4-7), cochlear fluid homeostasis, aquaporins |
| Dhingra's Diseases of Ear, Nose and Throat | Inner ear anatomy, clinical correlations with Ménière's disease |
| Hazarika's Textbook of ENT & HNS | Endolymph/perilymph clinical aspects |
| Zakir Hussain's Clinical ENT | Endolymph, perilymph, clinical correlations |
| KJ Lee's Essential Otolaryngology, 11th Ed. | Perilymph fistula, inner ear fluids |
| Ichikawa R et al., Acta Otolaryngol 2024 [PMID 38511591] | AQP10/11/12 in stria vascularis |
| Fukuda M et al., iScience 2024 [PMID 39563888] | Endolymph proteomics |
| Mom R et al., Biomolecules 2022 [PMID 35454100] | Dexamethasone-AQP2 axis |
| Fankhauser & Kempfle, HNO 2026 [PMID 42307737] | Gene therapy for Ménière's disease |
QUICK REVISION POINTS (RGUHS 20-Mark Checklist)
- Two compartments: Perilymph (bony labyrinth) and Endolymph (membranous labyrinth)
- Perilymph: High Na⁺ (148 mM), Low K⁺ (4.2 mM) - like ECF/CSF
- Endolymph: High K⁺ (157 mM), Low Na⁺ (1.3 mM), very Low Ca²⁺ (0.023 mM) - like ICF
- Endocochlear potential: +80 mV (cochlea only, not vestibule)
- Generated by: Stria vascularis (marginal cells via KCNQ1/KCNE1)
- K⁺ recycling via: Gap junctions (Connexins 26, 30, 31, 43) through supporting cells → spiral ligament → stria vascularis
- KCNJ10 in intermediate cells - essential for EP generation
- Endolymph drainage via endolymphatic sac (main) + Reissner's membrane (minor)
- Perilymph source: blood ultrafiltrate + CSF via cochlear aqueduct
- Water regulation: Aquaporin 2 (vasopressin-regulated) in endolymphatic sac
- GJB2 mutations (Connexin 26) = most common cause of hereditary SNHL (DFNB1)
- Endolymphatic hydrops → Ménière's disease; excess AVP → AQP2 overactivation
- Perilymph fistula: leak of perilymph through oval/round window → fluctuating SNHL
- Furosemide inhibits NKCC1 → reduces EP → used to test cochlear function (electrocochleography)
- Pendrin (SLC26A4) - Cl⁻/HCO₃⁻ exchanger in ELS - mutations cause Pendred syndrome + EVA
This is a shared conversation. Sign in to Orris to start your own chat.