Above knee amputation
Reading File
Finding Sources
Searching PubMed
"transfemoral amputation" AND rehabilitation
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Now I have all the content needed for a thorough answer. Here it is:
Above-Knee Amputation (Transfemoral Amputation)
Definition and Overview
An above-knee or transfemoral amputation (AKA/TFA) is the surgical removal of the lower limb through the femoral shaft, proximal to the knee joint. It carries the highest energy cost of all lower limb amputations and significantly impacts walking ability.
Indications
Indications span four main categories:
| Category | Details |
|---|---|
| Vascular / Diabetes | Peripheral artery disease with gangrene, diabetic foot infections with ischemia, failed below-knee amputation (BKA) requiring revision, absent femoral pulse |
| Infection | Necrotizing soft tissue infections (NSTIs) with extensive soft tissue damage, septic shock requiring rapid source control, osteomyelitis not amenable to distal salvage |
| Trauma | Severe open fractures with irreparable vascular injury, mangled extremity where BKA is not feasible |
| Oncology | Soft tissue or bone sarcoma where limb salvage is not possible |
A key decision point: a below-knee amputation should always be preferred if feasible, as it preserves the knee joint and dramatically improves rehabilitation potential. An AKA is reserved for patients who are bed-bound, have severe ischemia precluding BKA healing (absent femoral pulse), or have tissue loss too proximal for a below-knee flap. - Sabiston Textbook of Surgery, p. 2342; Bailey & Love, p. 8000
Surgical Anatomy - Key Principles
Optimal bone length: The femur should be transected at least 12 cm above the knee joint to accommodate a prosthetic knee mechanism. Greater femoral length improves the lever arm, suspension, and limb advancement. The femur is typically divided in the distal one-third if tissue allows. - Miller's Review of Orthopaedics, p. 875
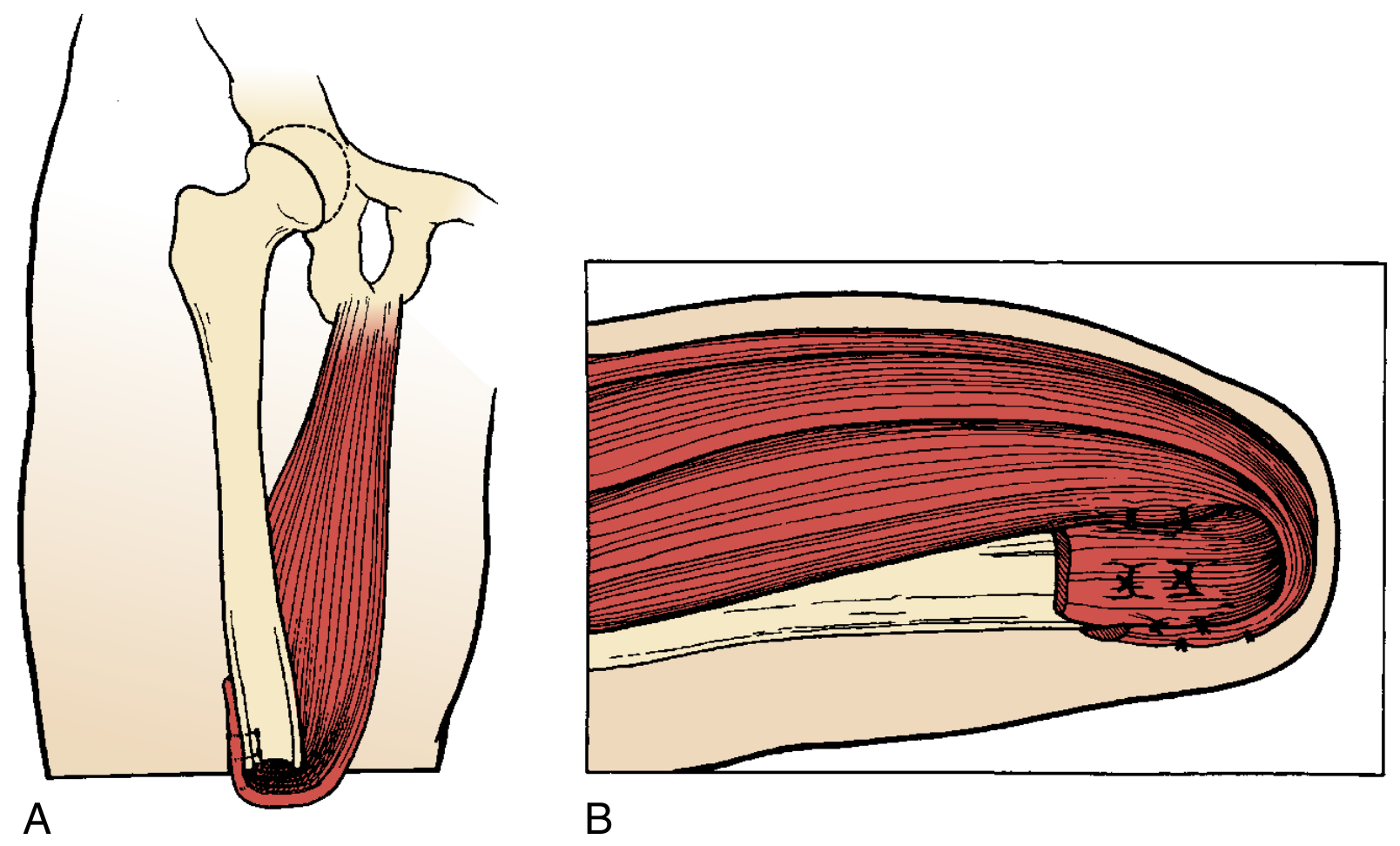
Adductor myodesis is the single most important technical step. The major deforming forces after AKA are abduction and flexion of the stump. Adductor magnus must be reattached (myodesis) to the lateral femur to maintain femoral adduction during stance phase, which is essential for prosthetic function. Transecting the adductor magnus results in a 70% loss of adductor pull.
Surgical Technique
The standard technique follows these steps (Sabiston, p. 2342):
- Incision: Fishmouth technique with anterior and posterior flaps; corners curve proximally. The posterior flap is made 1-2 cm longer to keep the closure away from a dependent position.
- Vascular control: Suture ligation of the femoral artery and vein.
- Bone transection: A periosteal elevator clears the femur ~2-3 cm proximal to the skin incision; the femur is transected proximal to the corners of the incision with an electric saw.
- Nerve handling: The sciatic nerve is placed on tension, tied with absorbable suture, and sharply transected - allowing it to retract. This prevents neuroma formation abutting the stump.
- Muscle closure: Muscles are reapproximated with absorbable sutures over the bone end (myoplasty/myodesis).
- Fascial closure: Anterior and posterior fascia approximated with interrupted absorbable sutures.
- Skin closure: Vertical mattress interrupted permanent sutures or skin staples.
Stump length rule: The stump must be at least 20 cm above the knee for adequate prosthetic leverage and suction suspension. - Bailey & Love, p. 8015
Energy Cost of Walking - Critical Exam Point
AKA carries the highest energy cost among lower limb amputations:
| Amputation Level | Energy Above Baseline (%) | Walking Speed (m/min) |
|---|---|---|
| Long transtibial | 10% | 70 |
| Average transtibial | 25% | 60 |
| Bilateral transtibial | 41% | 50 |
| Transfemoral | 65% | 40 |
| Wheelchair | 0-8% | 70 |
Key rule: Bilateral transtibial amputation (40-50% energy increase) costs less energy than unilateral transfemoral amputation (65-75%). This is why preserving the knee is so important. Patients with peripheral vascular disease and a transfemoral amputation may have an obligate doubling of energy expenditure while walking. - Miller's Review of Orthopaedics, p. 869
Postoperative Management
- Wound dressing: Rigid dressings are difficult to apply at this level; elastic compression dressings suspended about the opposite iliac crest are used instead.
- Positioning: Prevent hip flexion contracture - avoid prolonged sitting with the stump in flexion; prone lying exercises are encouraged.
- Early mobilisation: Begin between parallel bars; an inflatable artificial limb allows weight bearing before a formal prosthesis is ready.
- Pain: Regular opiate analgesia; phantom limb pain managed separately.
- Care of the contralateral limb: A pressure ulcer on the remaining foot will delay rehabilitation.
Complications
Early:
- Haemorrhage - return to OR for haemostasis
- Haematoma - requires evacuation
- Wound infection (often associated with haematoma)
- Gas gangrene (rare)
- Deep vein thrombosis / pulmonary embolism
Late:
- Phantom limb pain - most common chronic complication
- Neuroma - from improper nerve handling
- Skin breakdown - from poor prosthetic socket fit
- Hip flexion contracture - compromises prosthetic gait
- Stump revision - for inadequate length or poor soft tissue coverage
- Psychological morbidity - altered body image, depression
Prosthetics and Rehabilitation
- Socket design: The transfemoral socket must provide intimate total-contact fit because load transfer is indirect (unlike knee/ankle disarticulation where end-bearing is possible). A 2026 systematic review (PMID 39820416) found subischial sockets may offer advantages over traditional ischial containment designs.
- Prosthetic components: A prosthetic knee joint is required - microprocessor knees (C-Leg) offer improved stability and reduced fall risk in active patients.
- Gait training: Patients must compensate for absent knee proprioception; weight-bearing asymmetry during sit-to-stand is a significant rehabilitative challenge.
- Vascular disease patients: Patients with transfemoral amputations from PVD are unlikely to become efficient walkers - this is the core reason to preserve the knee if possible. - Miller's Review of Orthopaedics, p. 875
Comparison with Knee Disarticulation
Through-knee amputation has regained popularity as an alternative when AKA would otherwise be required:
- Preserves full femoral length - better lever arm
- Self-suspending bulbous stump - less rotation
- Better for non-ambulatory patients (improved core stability and sitting balance)
- Controlled by stronger proximal muscles
- Bailey & Love, p. 8019
Recent Evidence
- [PMID 39820416] (2026 Systematic Review, Prosthet Orthot Int): Subischial sockets vs. traditional designs in transfemoral amputees - RCTs show potential functional advantages.
- [PMID 39240037] (2024 Systematic Review + Meta-analysis): Weight-bearing asymmetry during sit-to-stand after major lower-limb amputation is consistent and clinically significant, relevant for rehabilitation planning.
This is a shared conversation. Sign in to Orris to start your own chat.