Myxovirus 2nd yr mbbs microbiology refer apurba sastri cover definition ortho myxoviridie infection influenza antigenic variation clinical manifestation virulence factor,pathogenesis symptoms suppurative complications, non suppurative complications, lab diagnosis treatment answer in details
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed for a comprehensive answer. Let me compile the complete detailed response.
Myxovirus - Influenza (Orthomyxoviridae)
2nd Year MBBS Microbiology | Based on Sherris & Ryan's Medical Microbiology (8th Ed.) and Jawetz, Melnick & Adelberg's Medical Microbiology (28th Ed.)
Note: Apurba Sastri's textbook is not available in the digital library. The content below is drawn from equivalent standard microbiology references (Jawetz and Sherris & Ryan) which cover the same syllabus topics.
1. DEFINITION
Myxoviruses are a group of enveloped, RNA viruses that have an affinity for mucoproteins (myxo = mucus). They are divided into two families:
- Orthomyxoviridae - the influenza viruses (ortho = true/straight)
- Paramyxoviridae - parainfluenza, mumps, measles, RSV
2. ORTHOMYXOVIRIDAE - FAMILY CHARACTERISTICS
Classification and Structure
- Family: Orthomyxoviridae
- Types: Influenza A, B, and C (classified by antigenic differences in their ribonucleoprotein [NP] and matrix [M] protein antigens)
- Shape: Enveloped, pleomorphic (spherical to filamentous), helical nucleocapsid
- Genome: Single-stranded, negative-sense, segmented RNA
- Influenza A and B: 8 segments
- Influenza C: 7 segments
- Size: 80-120 nm
- Replication: Occurs in the nucleus (unlike paramyxoviruses, which replicate in the cytoplasm)
Key Structural Proteins
| Protein | Location | Function |
|---|---|---|
| Hemagglutinin (HA) | Envelope spike (trimer) | Attaches to sialic acid receptors on host cells; fusion with cell membrane; target of neutralizing antibodies |
| Neuraminidase (NA) | Envelope spike (tetramer) | Cleaves sialic acid; facilitates virus release from infected cells; lowers mucus viscosity |
| M2 protein | Envelope (Influenza A only) | Ion channel; target of adamantane drugs |
| NB protein | Influenza B only | Ion channel equivalent of M2 |
| HEF protein | Influenza C only | Combined hemagglutinin-esterase-fusion |
| Nucleoprotein (NP) | Internal | Determines type specificity (A, B, C) |
| Matrix (M1) protein | Internal | Structural; surrounds nucleocapsid |
| RNA polymerase | Internal | Lacks proofreading - source of mutations |
Differences Among Influenza Viruses (Table)
| Feature | Influenza A | Influenza B | Influenza C |
|---|---|---|---|
| Gene segments | 8 | 8 | 7 |
| Unique protein | M2 | NB | HEF |
| Host range | Humans, swine, avians, equines, marine mammals, bats | Humans and seals | Humans and pigs |
| Antigenic drift | Yes | Less frequent | No |
| Antigenic shift | Yes | No | No |
| Epidemic potential | Major epidemics + pandemics | Localized outbreaks | Minor disease |
| Virulence | Most severe | Moderate | Mildest |
- Sherris & Ryan's Medical Microbiology, 8th Ed., p. 314
3. INFLUENZA INFECTION - EPIDEMIOLOGY
- Transmission: Direct droplet spread (most common), contaminated hands/surfaces
- Incubation period: 1-4 days (average 2 days)
- Infectivity period: Begins about 1 day before symptoms, lasts 5-7 days
- Seasonal pattern: Winter epidemics in temperate climates
- Epidemic waves: Influenza A every 2-3 years; Influenza B every 3-6 years
- Pandemic: Every 10-40 years when a new influenza A subtype appears
- Known pandemics: 1918 H1N1 (Spanish flu), 1957 H2N2 (Asian flu), 1968 H3N2 (Hong Kong flu), 2009 H1N1 (Swine flu)
4. ANTIGENIC VARIATION
This is the most important feature of influenza A, explaining why immunity from one year does not protect in subsequent years.
A. Antigenic Drift (Minor change)
- Definition: Gradual, progressive change in H or N antigens due to accumulation of point mutations in viral RNA
- Mechanism: RNA polymerase lacks proofreading ability, so errors accumulate. Mutant strains that escape the host's immune response are selected by immunological pressure
- Frequency: Occurs every year to every few years; can occur multiple times in a single epidemic
- Affects: All three influenza types (A, B, and C), but most prominently A
- Result: Previously immune individuals can be reinfected by the new variant
- Implication: Annual reformulation of influenza vaccines is required
B. Antigenic Shift (Major change)
- Definition: Abrupt, drastic change in H or N antigen due to genetic reassortment (exchange of whole RNA segments) between two different influenza A strains co-infecting the same cell (usually an intermediate host like a pig)
- Mechanism: When a human influenza A virus and an animal influenza A virus co-infect the same cell (often a pig), the 8 genome segments can mix, producing a novel reassortant virus with entirely new H or N antigens
- Frequency: Unpredictable; occurs every 10-40 years
- Affects: Only Influenza A (because types B and C are restricted to humans; animal reservoirs of A allow reassortment)
- Result: A new subtype against which the population has no pre-existing immunity -> pandemic
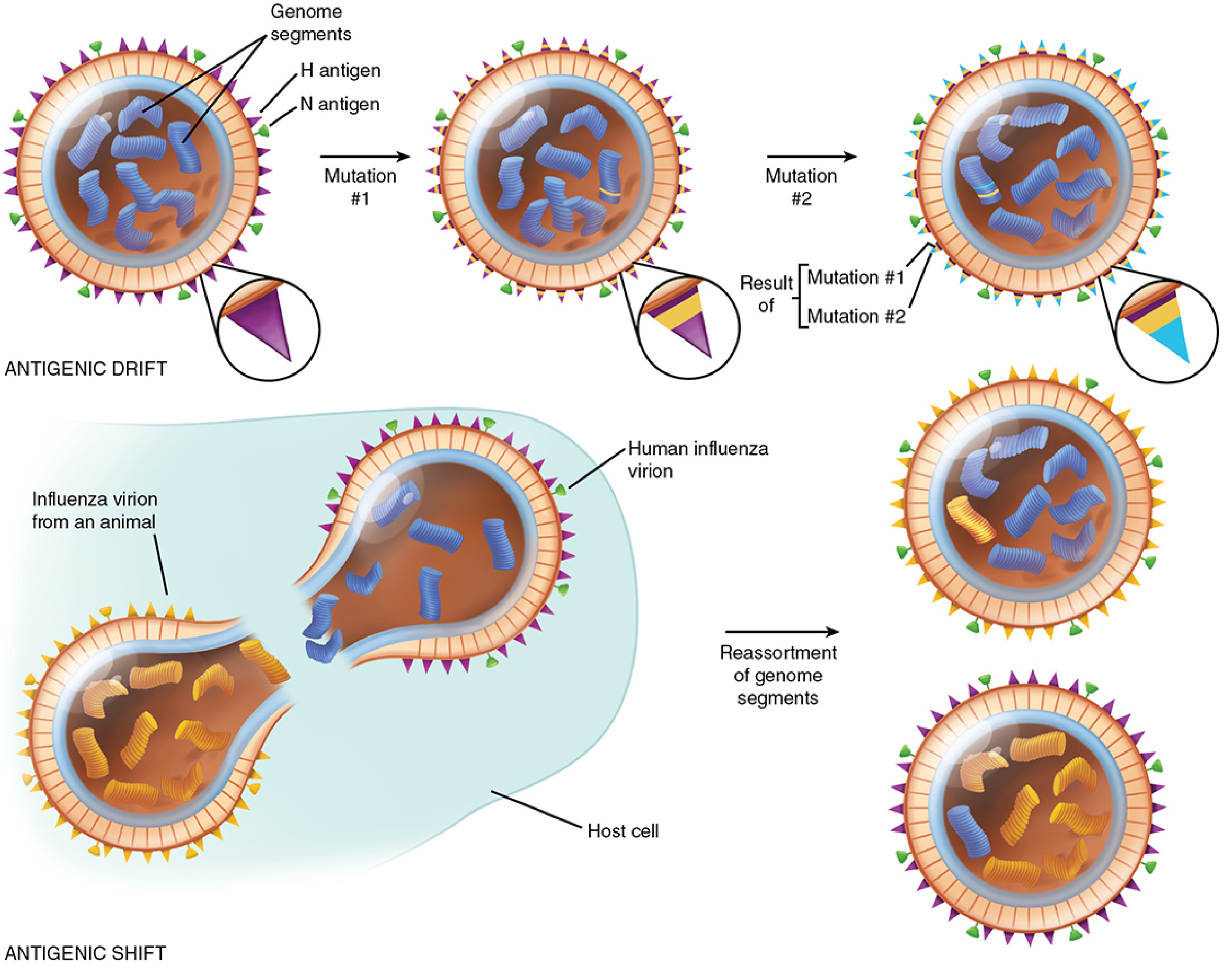
Above: Antigenic drift (top) occurs through sequential point mutations. Antigenic shift (bottom) occurs through reassortment of genome segments when a human and animal influenza virion co-infect the same host cell, producing entirely new progeny viruses.
- Jawetz Medical Microbiology, 28th Ed., p. 595
5. VIRULENCE FACTORS
-
Hemagglutinin (HA):
- Mediates attachment to sialic acid receptors on respiratory epithelial cells (SA α2,6 receptors in upper respiratory tract for human strains)
- HA must be cleaved into HA1 + HA2 by host cell proteases to be infectious
- More virulent strains use ubiquitous enzymes (e.g., plasmin) enabling systemic spread
- HA2 amino-terminal provides fusion activity at low pH for viral entry
-
Neuraminidase (NA):
- Lowers viscosity of mucus, exposing cell surface receptors
- Promotes spread of virus to lower respiratory tract
- Facilitates release of newly formed virions from infected cells
-
RNA Polymerase (lack of proofreading):
- Drives antigenic drift, enabling immune escape
-
Segmented genome:
- Enables antigenic shift/genetic reassortment, generating pandemic strains
-
NS1 protein (Non-structural):
- Interferon antagonist - blocks host innate immune response
-
PB1-F2 protein:
- Induces apoptosis in immune cells (macrophages, monocytes)
- Jawetz Medical Microbiology, 28th Ed., p. 589
6. PATHOGENESIS
- Entry: Virus enters via inhalation of infectious droplets. Deposited in respiratory mucosa
- First-line defense: May be cleared by cough reflex, neutralized by secretory IgA, or inactivated by mucus inhibitors
- Attachment: HA binds to sialic acid receptors on ciliated respiratory epithelial cells
- Entry: Virus is endocytosed; low pH in endosome triggers HA2 conformational change -> membrane fusion -> genome released into cytoplasm
- Replication: Genome transported to nucleus; viral RNA polymerase transcribes mRNAs; replicated in nucleus (unique among RNA viruses)
- Spread: NA cleaves sialic acid from cell surfaces, reducing mucus viscosity and allowing spread to lower respiratory tract. Newly formed virions bud from infected cells
- Cell damage: Virus kills infected respiratory epithelial cells -> desquamation of mucosa, ciliary dysfunction -> loss of the mucociliary escalator (mechanical clearance mechanism)
- Systemic effects: Cytokine storm (IL-1, TNF, IL-6, interferons) causes fever, myalgia, headache
- Secondary bacterial invasion: Loss of ciliary clearance and disrupted mucosal barrier -> bacterial superinfection (most common cause of death in seasonal influenza)
- Viremia: Uncommon in usual influenza; virus generally stays confined to respiratory tract
- Jawetz Medical Microbiology, 28th Ed., p. 592
7. CLINICAL MANIFESTATIONS
Typical (Uncomplicated) Influenza
- Incubation: 1-4 days (average 2 days)
- Onset: Abrupt, over a few hours
- Symptoms:
- High fever (38-40°C)
- Severe myalgia (muscle aches) - often the most distressing symptom
- Headache
- Chills (occasionally shaking rigors)
- Within 6-12 hours: dry, nonproductive cough, pharyngitis, rhinitis
- Respiratory distress in severe cases
- Duration: Acute phase 3-5 days
- Recovery: Feeling significantly better by 1 week, but fatigue, weakness, and cough persist for 2-6 weeks
Severe/Complicated Influenza
-
Progressive involvement of tracheobronchial tree and lungs
-
Primary viral pneumonia: Direct viral invasion of lung parenchyma
-
CNS dysfunction
-
Myositis (especially in children)
-
Myocarditis
-
Sherris & Ryan's Medical Microbiology, 8th Ed., p. 332
8. SUPPURATIVE (PURULENT) COMPLICATIONS
These result from bacterial superinfection, the most common and important complication of influenza:
-
Bacterial pneumonia - most common serious complication
- Causative organisms (in order of frequency):
- Streptococcus pneumoniae (most common)
- Haemophilus influenzae
- Staphylococcus aureus (most virulent; particularly associated with post-influenza necrotizing pneumonia)
- Pattern: Patient initially improves, then suddenly deteriorates with worsening fever, purulent sputum, lobar/bronchopneumonia on X-ray
- Can occur at any time during acute or convalescent phase
- Causative organisms (in order of frequency):
-
Sinusitis (bacterial)
-
Otitis media - particularly in children
-
Bacteremia - secondary bacteremia from lung with seeding of distant sites
Mechanism: Influenza damages ciliated epithelium -> loss of mucociliary clearance -> bacteria colonize and invade. Viral proteins (PB1-F2) also impair macrophage function.
- Sherris & Ryan's Medical Microbiology, 8th Ed., p. 333
9. NON-SUPPURATIVE (NON-PURULENT) COMPLICATIONS
These are direct consequences of the viral infection itself or immune-mediated processes:
-
Reye Syndrome
- Occurs especially in infants and children, 2-12 days after infection
- Characterized by:
- Severe fatty infiltration of the liver (hepatic dysfunction)
- Cerebral edema (encephalopathy)
- Risk dramatically increased by aspirin (salicylate) use during viral illness
- Also associated with varicella and other systemic viral illnesses
- Aspirin is CONTRAINDICATED in children with influenza
-
Primary Viral Pneumonia
- Direct viral pneumonia without bacterial superinfection
- More common with H5N1 and pandemic strains (e.g., 2009 H1N1)
- Mechanism: cytokine storm, alveolar flooding, Na+ channel blockage
- High mortality, particularly in young healthy adults
-
Encephalitis / CNS complications
- Encephalopathy, febrile seizures in children
- Rare but recognized
-
Myocarditis
- Direct viral involvement of myocardium
-
Myositis / Rhabdomyolysis
- Muscle inflammation, elevated CK
- Myoglobinuria and renal failure in severe cases
-
Post-influenza asthenia
- Prolonged fatigue and weakness for weeks after acute illness
-
Decompensation of underlying disease
- Elderly and those with chronic cardiac or pulmonary disease are at high risk of decompensation from any respiratory infection
- Sherris & Ryan's Medical Microbiology, 8th Ed., p. 333-334
10. LABORATORY DIAGNOSIS
Specimen Collection
- Nasopharyngeal swabs (highest yield), nasal swabs, or throat swabs
- Collected during the acute phase (first 48-72 hours of illness)
- Bronchoalveolar lavage in severe cases
Diagnostic Methods (in order of clinical use)
| Method | Details | Remarks |
|---|---|---|
| 1. Rapid Antigen Detection (RIAT) | Detects viral antigens (mainly NP) by immunoassay (EIA, ELISA) in nasopharyngeal swabs | Most widely used; results in 15-30 min; sensitivity ~50-70%, specificity ~90-95% |
| 2. RT-PCR (Molecular) | Reverse transcription PCR detects viral RNA (most sensitive and specific) | Gold standard for definitive diagnosis; can subtype (H/N); differentiates A from B; used for surveillance |
| 3. Immunofluorescence (DFA/IFA) | Direct or Indirect Fluorescent Antibody staining of nasopharyngeal cells | Rapid, requires expertise; sensitivity ~70-90% |
| 4. Virus Culture | Cell lines (MDCK - Madin-Darby Canine Kidney cells); virus grows in 2-7 days | "Gold standard" historically; slow; used mainly for surveillance and antigenic characterization |
| 5. Serology | Paired sera (acute + convalescent, 2-4 weeks apart); 4-fold rise in HAI or CF antibody titers | Not useful for acute diagnosis; used epidemiologically |
| 6. Hemagglutination Inhibition (HAI) test | Specific antibodies inhibit virus-induced hemagglutination of RBCs | Used for serotyping, vaccine strain selection, seroepidemiological studies |
Key points:
-
Virus grows in the amniotic cavity of chick embryos (egg inoculation), forming hemagglutinins
-
MDCK cell lines are the standard for viral culture
-
Cytopathic effect (CPE) in cell culture is confirmed by hemadsorption
-
RT-PCR is now the most commonly used diagnostic test
-
Sherris & Ryan's Medical Microbiology, 8th Ed., p. 334; Jawetz Medical Microbiology, 28th Ed., p. 593
11. TREATMENT
General/Supportive
- Bed rest, hydration, antipyretics (paracetamol/acetaminophen)
- Aspirin is CONTRAINDICATED in children (risk of Reye syndrome)
Antiviral Drugs
A. Neuraminidase Inhibitors (NAIs) - First-line therapy
| Drug | Route | Notes |
|---|---|---|
| Oseltamivir (Tamiflu) | Oral | Active against both Influenza A and B; most widely used |
| Zanamivir (Relenza) | Inhaled | Active against both A and B |
| Peramivir | IV | For hospitalized patients |
- Most effective when started within 48 hours of symptom onset
- Mechanism: Inhibit neuraminidase -> prevent release of new virions from infected cells -> reduce spread
- Resistance to NAIs is less common than M2 inhibitors
B. M2 Ion Channel Inhibitors (Adamantanes) - No longer recommended
| Drug | Notes |
|---|---|
| Amantadine | Active against Influenza A only |
| Rimantadine | Active against Influenza A only |
- Mechanism: Block M2 ion channel -> prevent uncoating
- No longer recommended due to widespread resistance (>99% of circulating H3N2 strains are resistant)
- Inactive against Influenza B (no M2 protein in influenza B)
C. Novel Antivirals
| Drug | Mechanism | Notes |
|---|---|---|
| Baloxavir marboxil | Cap-dependent endonuclease inhibitor | Single oral dose; active against both A and B |
| Favipiravir | RNA polymerase inhibitor | Used in some countries |
Indications for Antiviral Treatment
- High-risk groups: elderly (>65 years), immunocompromised, chronic cardiac/pulmonary/renal disease, pregnant women, children <2 years
- Hospitalized patients
- Within 48 hours of onset for outpatients
Prophylaxis
-
Annual influenza vaccination - most effective prevention
- Inactivated influenza vaccine (IIV) - injectable; for most groups
- Live-attenuated influenza vaccine (LAIV) - intranasal; for healthy non-pregnant 2-49 year olds
- Vaccine formulated annually based on WHO surveillance of circulating strains (antigenic drift necessitates yearly updates)
-
Chemoprophylaxis: Oseltamivir can be used for post-exposure prophylaxis in high-risk contacts
-
Jawetz Medical Microbiology, 28th Ed., p. 594-595; Sherris & Ryan's Medical Microbiology, 8th Ed., p. 336
QUICK SUMMARY TABLE - Key Points for Exam
| Feature | Detail |
|---|---|
| Family | Orthomyxoviridae |
| Genome | ss (-) sense, segmented RNA, 8 segments (7 in C) |
| Envelope | Yes; HA and NA spikes |
| Replication site | Nucleus |
| Type-specific antigen | Nucleoprotein (NP) and Matrix (M1) |
| Antigenic drift | Point mutations in HA/NA; all types; yearly |
| Antigenic shift | Genetic reassortment; only Influenza A; pandemic |
| Most common complication | Bacterial pneumonia (Strep. pneumoniae, S. aureus, H. influenzae) |
| Non-suppurative complication | Reye syndrome (children, aspirin use) |
| Lab diagnosis | RT-PCR (best); Rapid antigen test (most used) |
| Culture medium | MDCK cell line or chick embryo (amniotic cavity) |
| First-line treatment | Oseltamivir (within 48 hours) |
| Contraindicated drug | Aspirin in children |
| Prevention | Annual inactivated vaccine |
Sources:
- Sherris & Ryan's Medical Microbiology, 8th Edition, pp. 313-336
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Edition, pp. 585-595
This is a shared conversation. Sign in to Orris to start your own chat.