What is anal fistula. How it happens. How it’s surgery happens. What happens in it
Anal Fistula - A Complete Guide
What Is an Anal Fistula?
- The internal opening is inside the anal canal, almost always at the dentate line (a landmark about 2 cm inside the anus where anal glands empty into the canal).
- The external opening is on the skin around the anus, usually within 3 cm of the anal opening.
- Goldman-Cecil Medicine, p. 17-19
- Pfenninger and Fowler's Procedures for Primary Care, p. 693
How Does It Happen? (Cause and Mechanism)
Step-by-Step Pathway
Risk Factors That Increase the Chance
- Crohn's disease (IBD) - up to 54% of Crohn's patients develop anal fistulas
- Diabetes
- Immunocompromised states (e.g., on steroids, HIV)
- Post-radiation to the pelvis
- Recurrent abscesses in the same location (50%+ chance of fistula)
- Tuberculosis
- Malignancy
Epidemiology
-
Affects about 8.6 per 100,000 people
-
Two to three times more common in men than women
-
Goldman-Cecil Medicine, p. 22-24
-
Harrison's Principles of Internal Medicine 22E, p. 1297
Types of Anal Fistulas (Classification)
| Type | Frequency | Description |
|---|---|---|
| Intersphincteric | ~70% | Tract lies between the internal and external sphincter muscles. Simplest type. |
| Transsphincteric | ~23% | Tract crosses through both sphincters. Can be "low" (safer) or "high" (risky). |
| Suprasphincteric | ~5% | Loops over the entire sphincter complex |
| Extrasphincteric | ~2% | Internal opening is away from the dentate line; often from pelvic disease (appendicitis, diverticulitis, Crohn's) |
| Horseshoe fistula | Rare | External openings on both sides of the anus, with a single internal opening in the posterior midline |
- Harrison's Principles of Internal Medicine 22E, p. 1299
- Goldman-Cecil Medicine, p. 26
What the Patient Feels (Symptoms)
-
Chronic drainage from a small opening near the anus - often the first complaint. The discharge can be pus, blood-stained fluid, or mucus.
-
Recurrent "boil" near the anus - forms, swells painfully, then bursts and temporarily relieves pain, over and over
-
Palpable firm nodule within 3 cm of the anal opening
-
Perianal skin irritation and wetness
-
When the external opening closes over temporarily, pus builds up and a new abscess forms
-
Patients often describe months of thinking the area "healed," then experiencing the same swelling and rupture again
-
Goldman-Cecil Medicine, p. 33
How It Is Diagnosed
- Prior perianal abscess that never fully healed
- Location, duration, drainage pattern
- Bowel symptoms (to check for Crohn's disease)
- Prior anorectal surgery
- The external opening may look like a small red bump (papule) or pustule on the perianal skin - not always a visible "hole"
- A fibrous cord (the tract) can often be felt under the skin, like a small firm pipe running toward the anus
- Digital rectal exam to feel for induration (firmness) at the dentate line, which marks the internal opening
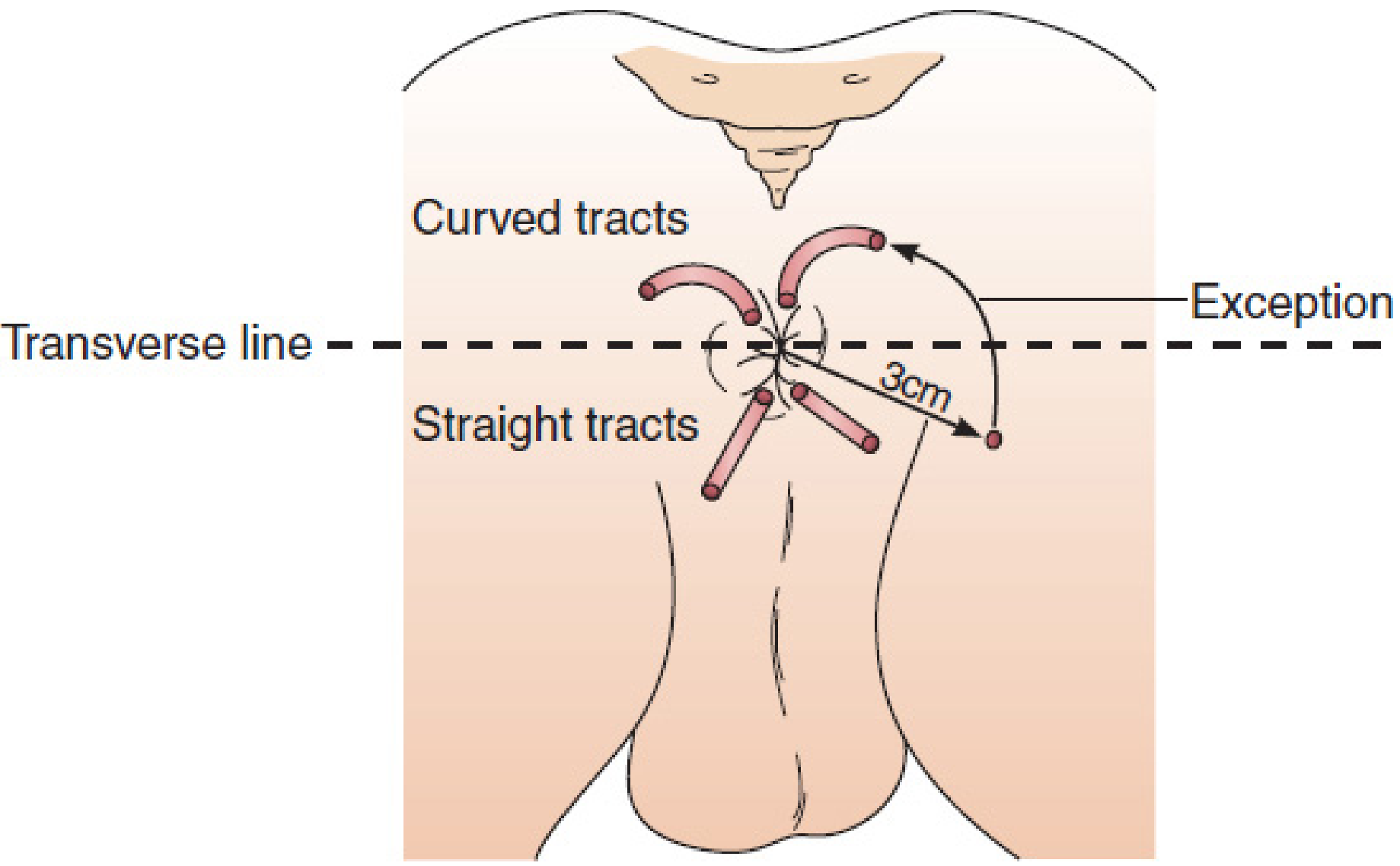
- An external opening posterior to an imaginary horizontal line across the anus connects internally to the posterior midline
- An external opening anterior to this line connects to the nearest anal crypt
- Exception: if the external opening is more than 3 cm from the anus, the tract may be complex and not follow this rule
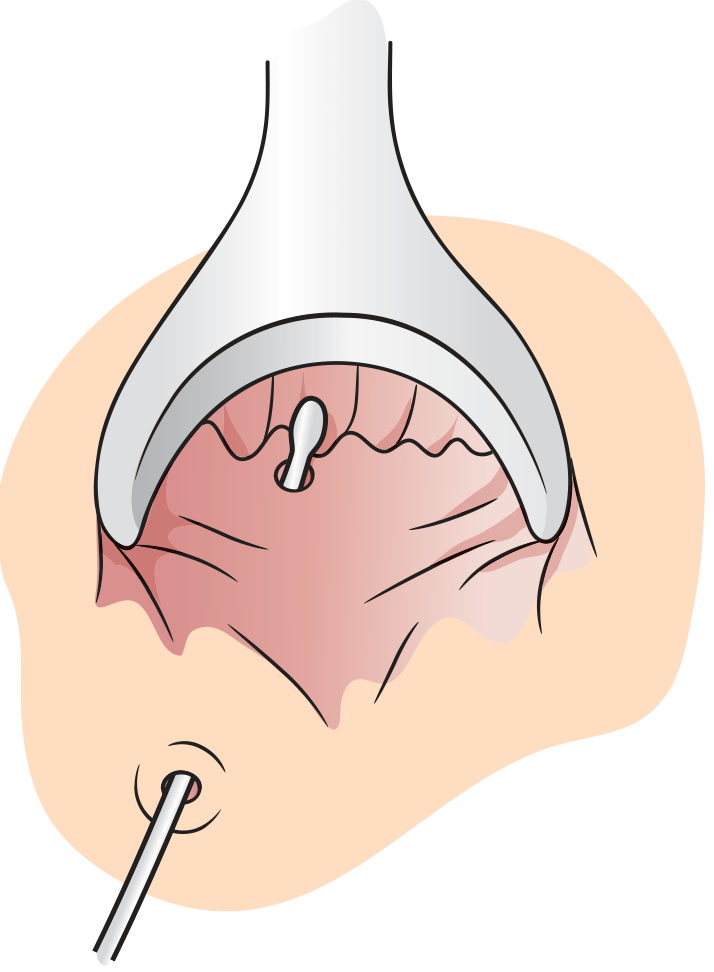
- A blunt probe is gently inserted into the external opening to feel the direction and depth of the tract
- Hydrogen peroxide injection into the external opening - bubbles appear at the internal opening, helping confirm its location
- Endoanal ultrasound - identifies fistula tracts
- MRI of the pelvis - gold standard for complex/multiple fistulas; 80% accuracy for tract identification; mandatory before operating on Crohn's-related fistulas
- Pfenninger and Fowler's Procedures for Primary Care, p. 694-695
- Harrison's Principles of Internal Medicine 22E, p. 1301
Surgery for Anal Fistula
Operation 1: Fistulotomy ("Laying Open")
- Patient is put under anesthesia (general, spinal, or MAC - monitored anesthesia care) in prone (face-down) or lithotomy position
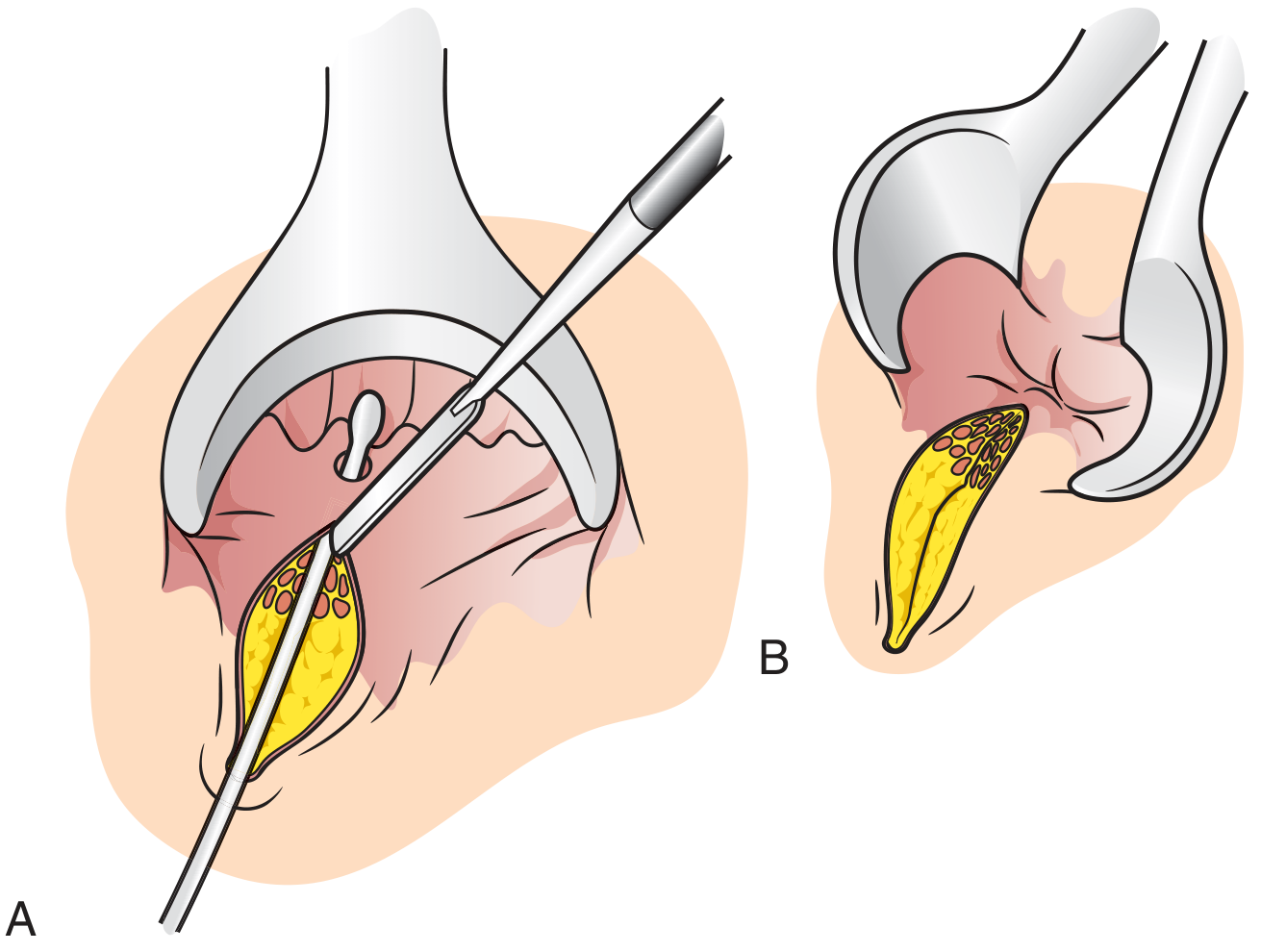
- The surgeon passes a probe through the fistula tract from external to internal opening
- Electrocautery or a scalpel is used to cut along the probe, opening the entire tract from skin to internal opening
- The wound is left open and packed with gauze - it heals by granulation over several weeks
- Mulholland and Greenfield's Surgery, p. 3562
- Harrison's Principles of Internal Medicine 22E, p. 1313
Operation 2: Seton Placement
- Keeps the external opening from closing over (preventing new abscess formation)
- Gradually promotes fibrosis (scarring) around the tract
- Allows the exact anatomy and sphincter involvement to be mapped safely before definitive surgery
- Draining seton - left loosely in place for 4-6 weeks to reduce inflammation, then definitive surgery follows
- Cutting seton - tightened progressively at 2-4 week intervals, slowly eroding through sphincter muscle over time. Success rate up to 94%, but incontinence risk ranges 22-23%.
- Mulholland and Greenfield's Surgery, p. 3562
- Goldman-Cecil Medicine, p. 40
Operation 3: Advancement Flap (Sphincter-Sparing)
- Seton is placed first to reduce inflammation (usually 4-6 weeks)
- Under anesthesia, a flap of rectal mucosa and internal sphincter is elevated (raised)
- The fistula tract is scraped (curetted) clean
- The internal opening is sutured shut
- The flap is pulled down and stitched over the closed internal opening
- The external opening is left open to drain
- Mulholland and Greenfield's Surgery, p. 3562-3563
Operation 4: LIFT Procedure (Ligation of the Intersphincteric Fistula Tract)
- Seton is placed first to allow fibrosis to form around the tract
- After fibrosis develops, an incision is made over the intersphincteric groove (between the two sphincter muscles)
- The fistula tract is identified within this plane
- Both sides of the exposed tract are ligated (tied off) with suture
- The tract between the ligatures is divided (cut)
- The wound is closed
- Mulholland and Greenfield's Surgery, p. 3562-3563
Summary: Which Surgery for Which Fistula?
| Fistula Type | Recommended Surgery |
|---|---|
| Simple intersphincteric / Low transsphincteric | Fistulotomy (lay open) |
| High transsphincteric / Complex | Seton first → then advancement flap or LIFT |
| Complex with multiple tracts | Seton, unroofing of branches, staged approach |
| Crohn's-related fistula | Seton + anti-TNF medication (e.g., infliximab); surgery only after inflammation is controlled |
What Happens After Surgery (Recovery)
- The wound is left open and packed with gauze, healing from the inside out over several weeks
- Patients take sitz baths (sitting in warm water) multiple times daily to keep the area clean
- Stool softeners and a high-fiber diet help reduce straining
- Regular follow-up visits for wound checks and packing changes
- Full healing typically takes 6-12 weeks depending on the complexity of the fistula
- Patients are monitored for recurrence or signs of incontinence
Key Takeaways
- An anal fistula is an infected tunnel from inside the anal canal to the outer skin, almost always caused by a perianal abscess that does not fully heal
- The core problem is a persistently infected anal gland at the dentate line
- It never heals on its own - surgery is always required
- The surgical challenge is eliminating the infection source without damaging the sphincter muscles that control bowel continence
- Simple/low fistulas are cured with fistulotomy; high/complex fistulas require staged, sphincter-sparing approaches
Why it happens
Why Does an Anal Fistula Happen?
The Root Cause - Anal Glands
The Step-by-Step Process
Why Doesn't It Just Heal?
Who Is More Likely to Get It?
| Risk Factor | Why It Increases Risk |
|---|---|
| Crohn's disease (IBD) | Chronic bowel inflammation extends to the perianal area, causing complex, multiple fistulas in up to 54% of patients |
| Diabetes | High blood sugar impairs immune response and wound healing |
| Steroids / immunosuppression | Weakens the body's ability to fight infection |
| Prior perianal radiation | Damages tissue and blood supply, impairing healing |
| Recurrent abscess | If you've had 2+ abscesses in the same spot, there is a >50% chance a fistula is already present |
| Tuberculosis | TB bacteria can infect perianal glands directly |
| Trauma or surgery | Disrupts normal tissue planes |
Less Common Causes (Non-Gland Origin)
- Crohn's disease transmural inflammation
- Pelvic abscess from ruptured appendix or diverticulitis (these create extrasphincteric fistulas)
- Tuberculosis of the perianal region
- Malignancy (rectal cancer eroding through tissue)
- Radiation proctitis
In One Sentence
In non medico term and in simple tell what it is
What is Anal Fistula - In Plain, Simple Words
Think of it like this:
Where exactly?
How the tunnel forms - the simple story
What does the person feel?
- A small wet or leaky spot near their bottom that never dries up
- Sometimes a painful swelling that comes back again and again
- A bit of blood or pus on their underwear or tissue paper
- Soreness and itching around their bottom
- The swelling appears, hurts, bursts, goes away... then comes back in the same spot months later
Will it go away on its own?
One-line summary
Your bottom has a tiny infected tunnel connecting the inside to the outside skin - it keeps leaking and never heals without surgery.
How is anal fistula surgery performed in simple terms?
Anal Fistula Surgery - In Simple Words
The Goal of Every Surgery
- Destroy or remove the secret tunnel
- Not damage the muscles that keep you in control of your bowel (so you don't accidentally leak poo)
Before Surgery
- You go to hospital, usually as a day patient (go home same day)
- You are given anaesthesia - either fully asleep, or a spinal injection so the lower half of your body goes numb
- You lie either face down, or on your back with legs up
- The surgeon examines the tunnel carefully first - sometimes they inject a little hydrogen peroxide (the fizzy liquid) into the outside hole to see where the inside hole is, because bubbles appear at the internal opening
Surgery Type 1 - "Laying it Open" (Fistulotomy)
- The surgeon puts a thin probe (like a very thin wire) into the tunnel from the outside hole, all the way through to the inside
- Using a surgical tool (like an electric pen that cuts and seals at the same time), they cut along the probe - slicing the tunnel open from end to end
- Now instead of a closed tunnel, there is an open groove - like a trench
- That open trench is left open. It is NOT stitched shut
- The body fills it in from the bottom up, like filling a ditch with soil - this takes a few weeks
Surgery Type 2 - "The Rubber Band Trick" (Seton)
- Keeps the tunnel from closing over (so no painful abscess builds up again)
- Over weeks, the body slowly builds scar tissue around it
- The surgeon tightens the loop a little at every visit - like tightening a cheese wire, very slowly over months
- The muscle is cut so slowly (a tiny bit at a time) that the body hardens and compensates as it goes, protecting bowel control
- When the loop has worked its way through, the tunnel is gone
Surgery Type 3 - "Patching from the Inside" (Advancement Flap)
- The surgeon goes inside the back passage and cuts a small flap of tissue (like lifting a patch of carpet)
- The inside hole of the tunnel is stitched shut from underneath
- That flap of tissue is pulled down and stitched over the closed hole, like putting a patch over a hole in a wall
- The outside hole is left open to drain
- No muscle is cut at all
Surgery Type 4 - "Tie and Cut" (LIFT Procedure)
- A small cut is made in the groove between the two sphincter muscles
- The tunnel is found running through this space
- The surgeon ties a stitch on each side of the tunnel
- The piece of tunnel between the stitches is removed
- Now both ends are sealed - the tunnel is dead
Simple Comparison Table
| Surgery | What the Surgeon Does | Best For | Risk |
|---|---|---|---|
| Lay it open | Cuts the whole tunnel open, leaves it to heal | Shallow tunnels | Tiny muscle damage possible |
| Rubber band (seton) | Threads a loop through, tightens slowly over months | Deep tunnels near muscle | Slow process, small incontinence risk |
| Patch from inside | Stitches the inner hole, covers with a tissue flap | Deep/complex tunnels | No muscle risk, can fail and need redo |
| Tie and cut (LIFT) | Ties and cuts the tunnel from the middle | Medium tunnels | No muscle risk, newer technique |
After Surgery - What Happens?
- The wound is left open (not stitched up like a normal cut) - this is normal and intentional
- You take warm baths (sitting in a shallow bath of warm water 2-3 times a day) to keep it clean - this is called a sitz bath
- You eat high-fibre food and drink plenty of water so you pass stool easily without straining
- A nurse or doctor packs the wound with soft gauze at first to keep it clean
- The wound heals slowly from the inside out over 6 to 12 weeks
- You go back for regular check-ups to make sure it is healing properly
Will it Come Back?
- Simple fistulas treated with lay-open surgery: very rarely come back
- Complex fistulas: can sometimes recur - about 1 in 10 cases
- Fistulas from Crohn's disease need extra treatment (medication + surgery) and are harder to fully cure
One-Line Summary
The surgeon either opens the tunnel up to let it heal naturally, or seals it shut from the inside - whichever method is safest for the muscles that keep you in control of your bowel.
If someone has snap fistula and has went through a surgery recently and has issues with sitting. What would be good to be seted on like gel sit. Buying from India. For regular day to day use like siting and stuff just after surgery. Recommend by doc
best donut cushion gel seat cushion after anal fistula surgery buy India 2024
donut ring cushion post surgery sitting relief buy Amazon India price
https://www.reddit.com/r/AnalFistula/comments/1hgq8bu/favour…
Best Cushions to Sit On After Anal Fistula Surgery - India Buying Guide
First - Important Point About Donut Cushions
- A donut/ring cushion keeps direct pressure OFF the wound - which sounds ideal
- BUT for some patients, the ring shape stretches the skin around the anus and can actually make it MORE uncomfortable, especially in the first 2-3 weeks right after surgery when the wound is raw
- A flat memory foam or gel cushion (without the hole) sometimes feels better because it distributes weight evenly and does not pull the wound area
Types to Look For
Option 1 - Inflatable Air Donut Cushion ✅ Best for Post-Surgery
Option 2 - Memory Foam Donut Cushion ✅ Good for Day-to-Day Use
- Primica Donut Pillow Hemorrhoid Cushion - available on Amazon.in, rated well for post-surgery use
- BOS Medicare Surgical Donut Pillow - specifically listed for post-surgery sitting support (49% off currently on Amazon.in)
Option 3 - Gel + Memory Foam Flat Cushion ✅ Best for Long Sitting (Office/Car)
Where to Buy in India
| Platform | What to Search |
|---|---|
| Amazon.in | "donut pillow post surgery fistula" or "inflatable air cushion piles fistula" |
| Flipkart | "orthopedic donut cushion tailbone" |
| 1mg / Medprime | "surgical donut cushion" |
| Local medical/surgical shop | Ask for "air ring cushion" or "piles donut cushion" - most surgical supply shops stock them |
Tips for Using the Cushion
- On a hard chair (office, dining) - always use the cushion, never sit directly on a hard surface
- In the car - keep the cushion on the seat at all times; every bump on the road is painful without it
- On the toilet - a small inflatable ring on the toilet seat can make a huge difference
- On a sofa - a sofa is naturally soft, so sometimes no cushion is needed; use your comfort as a guide
- Do not sit for too long regardless of cushion - get up and walk around every 30-45 minutes to reduce pressure and help blood flow to the healing area
What to Avoid
- Hard plastic or wooden chairs without any cushion - very painful
- Very soft, deep-sinking sofas - these can actually push up on the wound area as you sink in
- Sitting cross-legged on the floor - puts uneven pressure on the wound
- Driving long distances in the first 2-3 weeks without stopping
Quick Recommendation Summary
| Situation | Best Choice |
|---|---|
| Right after surgery (week 1-2) | Inflatable air donut - adjustable, gentle |
| Daily office/desk use | Memory foam donut cushion |
| Car travel | Gel + memory foam flat cushion or inflatable donut |
| All-round best buy | Memory foam donut ₹500-1,000 from Amazon.in |
One Honest Tip from Patients
We have to buy one. What would be best overall. Give me specific name and detail and I will get it