History taking of RTA case comes with the 5th metatarsal fracture
Reading File
Finding Sources
Finding Sources
Searching the Web
5th metatarsal fracture history taking RTA clinical assessment zones
Reading File
Reading File
Reading File
Loading Image
Reading File
Here is a complete, structured history-taking framework for an RTA patient presenting with a 5th metatarsal fracture:
History Taking: RTA Case with 5th Metatarsal Fracture
1. Presenting Complaint
- Pain on the lateral aspect of the foot/ankle following a road traffic accident
- Inability or difficulty bearing weight
- Swelling and bruising over the outer foot
2. History of Presenting Illness (HPI)
Mechanism of Injury
This is the most critical part - it predicts fracture zone and type:
| Mechanism | Likely Fracture |
|---|---|
| Forced inversion of foot (ankle rolls inward) | Zone 1 - Avulsion fracture (Pseudo-Jones) |
| Strong abduction force to forefoot (bending moment at base) | Zone 2 - True Jones fracture |
| Direct blow / crush (foot run over, pedal impact) | Diaphyseal/shaft fracture (Zone 3 or distal) |
| Stress over time (repeated loading) | Zone 3 stress fracture |
In an RTA, ask specifically:
- Was the foot on the brake/clutch pedal at time of impact?
- Was there a direct crush (motorcycle fall, wheel over foot)?
- Did the foot roll inward on impact?
- Was there a twisting component?
Pain
- Location: Lateral border of foot, base of the 5th metatarsal, or along the shaft?
- Onset: Immediate after injury
- Character: Sharp, throbbing
- Severity: VAS/NRS score (0-10)
- Radiation: Up the leg or into the toes?
- Aggravating factors: Weight bearing, movement
- Relieving factors: Rest, elevation, analgesia
- Associated "snap" or "pop" heard at the time?
Weight-Bearing Status
- Can the patient walk at all? (Ottawa Foot Rules: inability to weight-bear = X-ray indicated)
- Did they walk after the injury?
3. Associated Injuries (Especially Important in RTA)
RTA is a high-energy mechanism - always screen for:
- Ankle injuries (ligament tears, malleolar fractures - inversion is the same mechanism)
- Other metatarsal fractures (Lisfranc pattern if multiple metatarsals involved)
- Calcaneus and talus fractures
- Knee and leg injuries (dashboard injury pattern)
- Pelvic/spinal injuries in high-speed RTA
- Open wounds or abrasions over the fracture site (open fracture risk)
- Neurovascular symptoms: Numbness or tingling in the toes?
4. Past Medical History
- Previous injury to the same foot (prior fractures, non-union risk if prior zone 2/3)
- Diabetes mellitus (impaired bone healing, neuropathy)
- Osteoporosis or metabolic bone disease (lower-energy fractures possible)
- Peripheral vascular disease (affects healing)
- Inflammatory arthritis (rheumatoid, gout)
- Neuropathy (may mask pain, increases non-union risk)
- Corticosteroid use (bone fragility)
5. Drug History
- NSAIDs (can impair fracture healing - Cox-2 inhibitors with particular concern)
- Steroids (bone quality)
- Bisphosphonates (atypical fracture pattern risk)
- Anticoagulants (haematoma, surgical planning)
- Diabetic medications
- Allergies (especially to latex, anaesthetic agents if surgery likely)
6. Social History
- Occupation: Manual labour vs. sedentary (affects weight-bearing advice and time off work; average 22 days off work post-injury)
- Dominant side / Affected foot: Right vs. left
- Driving status: Especially relevant if right foot - affects fitness to drive
- Sports/physical activity level: Athlete vs. non-athlete (directly impacts management - athletes with Zone 2 fractures are often offered surgical fixation)
- Smoking: Significantly impairs fracture healing and increases non-union risk
- Alcohol use: Nutritional status, compliance with treatment
- Living situation: Stairs at home? Anyone to help with mobility?
- BMI / Body weight: Increased load on fracture site with weight bearing
7. Functional History
- Pre-injury mobility: Was the patient walking normally before the accident?
- Pre-injury foot problems: Any previous foot pain, deformity, or flat feet (pes planus) or high arch (cavovarus - associated with Zone 3 stress fractures)?
8. System Review (Relevant)
- Fever (rule out open fracture/infection)
- Bladder/bowel changes (if high-energy RTA with spinal concern)
- Chest pain/SOB (rib fractures, pneumothorax in polytrauma)
Key Classification to Know (Lawrence & Botte Zones)
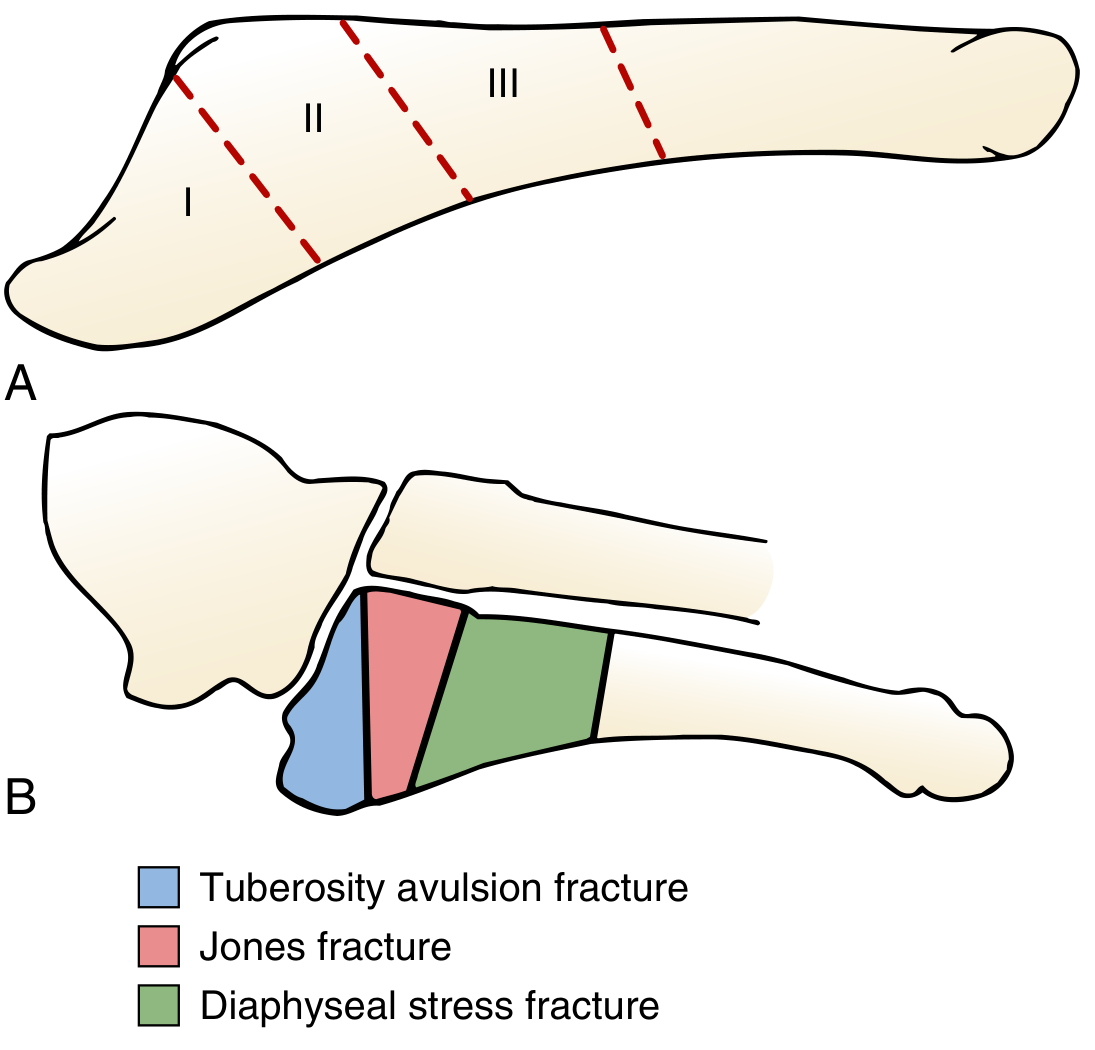
(From Miller's Review of Orthopaedics, 9th Ed, Fig. 6.108)
| Zone | Location | Fracture Type | In RTA? |
|---|---|---|---|
| Zone 1 | Proximal tuberosity | Avulsion (Pseudo-Jones) | Common - inversion |
| Zone 2 | Metaphyseal-diaphyseal junction, includes 4th-5th intermetatarsal joint | True Jones fracture | Less common in RTA |
| Zone 3 | Proximal diaphysis | Stress/diaphyseal | Rare - direct blow in RTA |
Examiner Tip: Ottawa Foot Rules (for X-ray decision)
X-ray of the foot is indicated if there is pain in the midfoot zone AND any of:
- Bone tenderness at the base of the 5th metatarsal, OR
- Bone tenderness at the navicular, OR
- Inability to bear weight immediately or in the ED (4 steps)
Sources:
- Miller's Review of Orthopaedics, 9th Ed, Ch. 12 (5th Metatarsal Base Fractures)
- Campbell's Operative Orthopaedics, 15th Ed, Ch. 93 (Metatarsals)
- Tintinalli's Emergency Medicine, Comprehensive Study (Foot and Toe Injuries)
- StatPearls - 5th Metatarsal Fracture (Smidt et al., 2023)
This is a shared conversation. Sign in to Orris to start your own chat.