I need an complete anatomy of respiratory system
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the detailed content needed. Let me compose the complete anatomy of the respiratory system.
Complete Anatomy of the Respiratory System
Sources: Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume; Morgan & Mikhail's Clinical Anesthesiology, 7e
Overview
The respiratory system has two interdependent essential functions:
- Ventilation-perfusion matching - delivering O2 to the body and removing CO2
- Host defense - protecting against airborne pathogens, chemicals, and particulates
Anatomically it is divided into the upper airway, the lower airway (tracheobronchial tree), the lungs and pleura, and the ventilatory pump (rib cage, muscles, neural control).
1. Upper Airway
Nose
The nose serves as the primary entry point for inspired air. It performs three critical functions: humidification, warming, and filtration of air. Turbinate bones increase the surface area of the nasal mucosa to maximize these functions. Hairs (vibrissae) at the nares trap large particles.
Pharynx
The pharynx is divided into three regions:
- Nasopharynx - posterior to the nasal cavity; contains the pharyngeal tonsil (adenoids) and the opening of the Eustachian tube
- Oropharynx - from the soft palate to the epiglottis; contains the palatine tonsils
- Laryngopharynx (hypopharynx) - from the epiglottis to the cricoid cartilage
Several pharyngeal muscles maintain airway patency. The genioglossus keeps the tongue from falling against the posterior pharyngeal wall (tonic inspiratory activity). The levator palati, tensor palati, palatopharyngeus, and palatoglossus prevent the soft palate from collapsing against the posterior pharynx, especially in the supine position.
Larynx
The larynx connects the pharynx to the trachea and houses the vocal cords. It is composed of cartilages:
- Thyroid cartilage - the largest; forms the "Adam's apple"
- Cricoid cartilage - the only complete ring in the airway; the narrowest part of the adult trachea (avg. 17 mm in men, 13 mm in women)
- Arytenoid cartilages - control vocal cord movement
- Epiglottis - leaf-shaped; prevents aspiration during swallowing
The glottis (vocal cords + rima glottidis) is the narrowest part of the larynx in adults.
2. Tracheobronchial Tree
Trachea
The trachea begins at the lower border of the cricoid cartilage and extends to the carina, with an average length of 10-13 cm. It is composed of C-shaped cartilaginous rings that form the anterior and lateral walls; the posterior wall is membranous. The trachea bifurcates at the carina at the level of the sternal angle (angle of Louis), corresponding to the T4/T5 vertebral level.
Mainstem Bronchi
- Right mainstem bronchus: shorter, wider, and lies in a more linear arrangement with the trachea - this is why aspirated foreign bodies and misplaced endotracheal tubes preferentially enter the right side. The right upper lobe bronchus takes off ~2.0 cm (men) / ~1.5 cm (women) from the carina.
- Left mainstem bronchus: longer (~5.0 cm in men, ~4.5 cm in women) and lies at a more angular orientation from the trachea. It divides into the left upper lobe bronchus and left lower lobe bronchus.
Dichotomous Division - 23 Generations
The tracheobronchial tree undergoes approximately 23 successive dichotomous divisions (each branch divides into two smaller branches), beginning with the trachea (generation 0) and ending in alveolar sacs (generation 23):
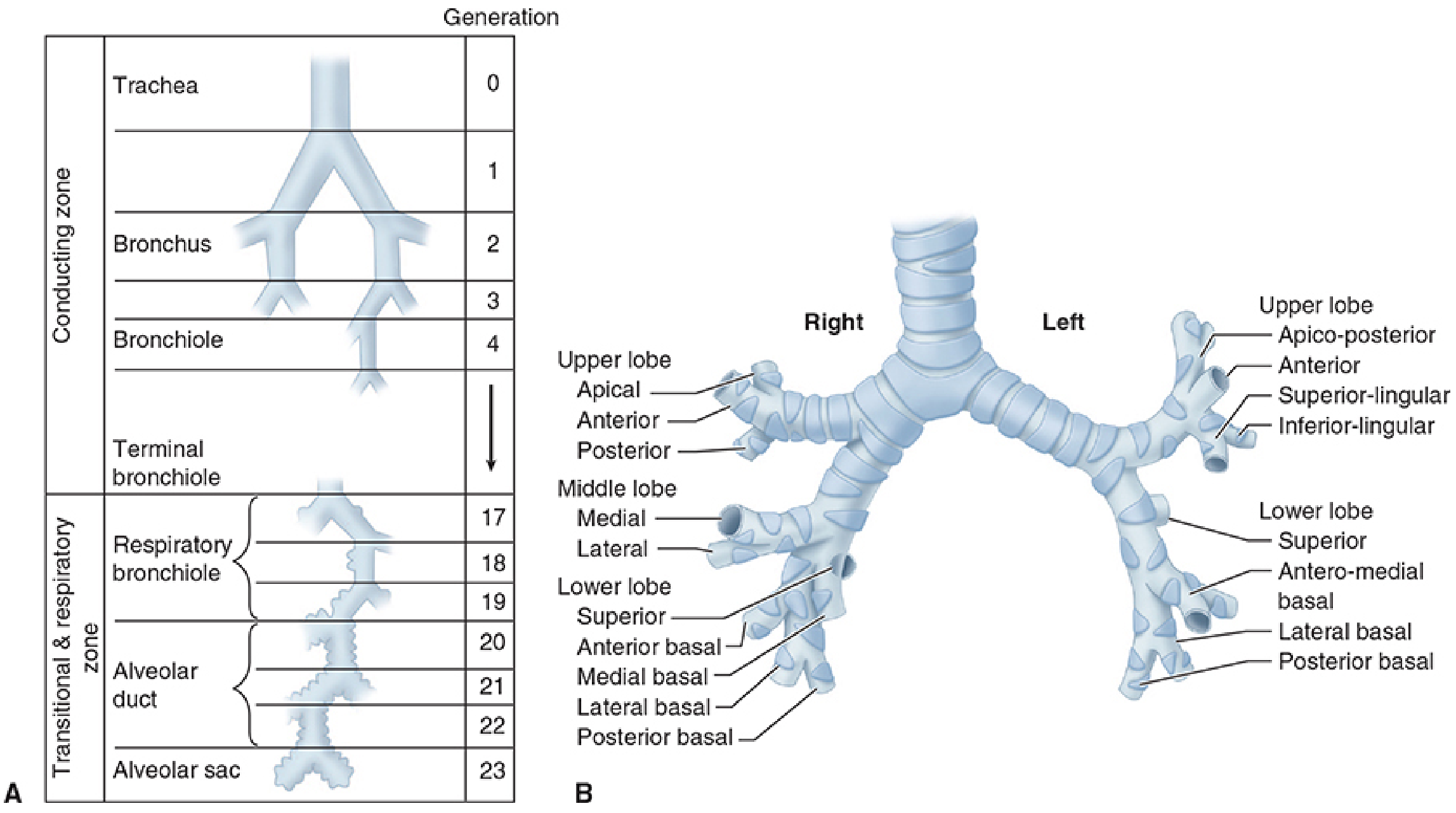
| Generation | Structure | Zone |
|---|---|---|
| 0 | Trachea | Conducting |
| 1-2 | Mainstem bronchi | Conducting |
| 3-4 | Lobar & segmental bronchi | Conducting |
| 5-16 | Bronchioles → terminal bronchioles | Conducting |
| 17-19 | Respiratory bronchioles | Transitional & respiratory |
| 20-22 | Alveolar ducts | Respiratory |
| 23 | Alveolar sacs | Respiratory |
The conducting zone (generations 0-16) carries air but does not participate in gas exchange - this constitutes anatomical dead space (~150 mL). Gas exchange begins only where flat alveolar epithelium first appears, starting at respiratory bronchioles (generations 17-19).
Bronchi vs. Bronchioles
- Bronchi have cartilaginous support in their walls and submucosal glands
- Bronchioles lack cartilage; patency depends on radial traction from surrounding elastic tissue - airway diameter becomes dependent on lung volume
- As the airway progresses distally, mucosa transitions from ciliated columnar epithelium → cuboidal → flat alveolar epithelium
3. Lungs
Gross Structure
The lungs occupy the thoracic cavity, each enclosed in its own pleura. The right lung is larger and has three lobes (upper, middle, lower); the left lung has two lobes (upper, lower) to accommodate the cardiac notch and the lingula.
Lobes and segments:
- Right lung - 10 bronchopulmonary segments:
- Upper lobe: apical, anterior, posterior
- Middle lobe: medial, lateral
- Lower lobe: superior, anterior basal, medial basal, lateral basal, posterior basal
- Left lung - 8-10 bronchopulmonary segments:
- Upper lobe: apico-posterior, anterior, superior lingular, inferior lingular
- Lower lobe: superior, antero-medial basal, lateral basal, posterior basal
Each bronchopulmonary segment is supplied by its own segmental bronchus and branch of the pulmonary artery, and drained by pulmonary veins that run in the intersegmental planes - this is the surgical unit of the lung.
Pleura
- Visceral pleura - directly covers the lung surface; has no pain fibers
- Parietal pleura - lines the inner chest wall, diaphragm, and mediastinum; richly innervated (pain-sensitive)
- Pleural space - a potential space between the two layers containing a thin film of fluid (~10-20 mL); the resting intrapleural pressure is approximately -5 cm H2O (subatmospheric), which keeps the lungs expanded against the chest wall
4. Alveoli and the Blood-Air Barrier
An estimated 300-500 million alveoli in the average adult provide a massive gas-exchange surface area of 50-100 m².
Alveolar size is gravity-dependent: in the upright position, apical alveoli are largest and basal alveoli are smallest. This equalizes with inspiration.
Alveolar Wall Structure
The alveolar wall (alveolocapillary membrane) is asymmetrical:
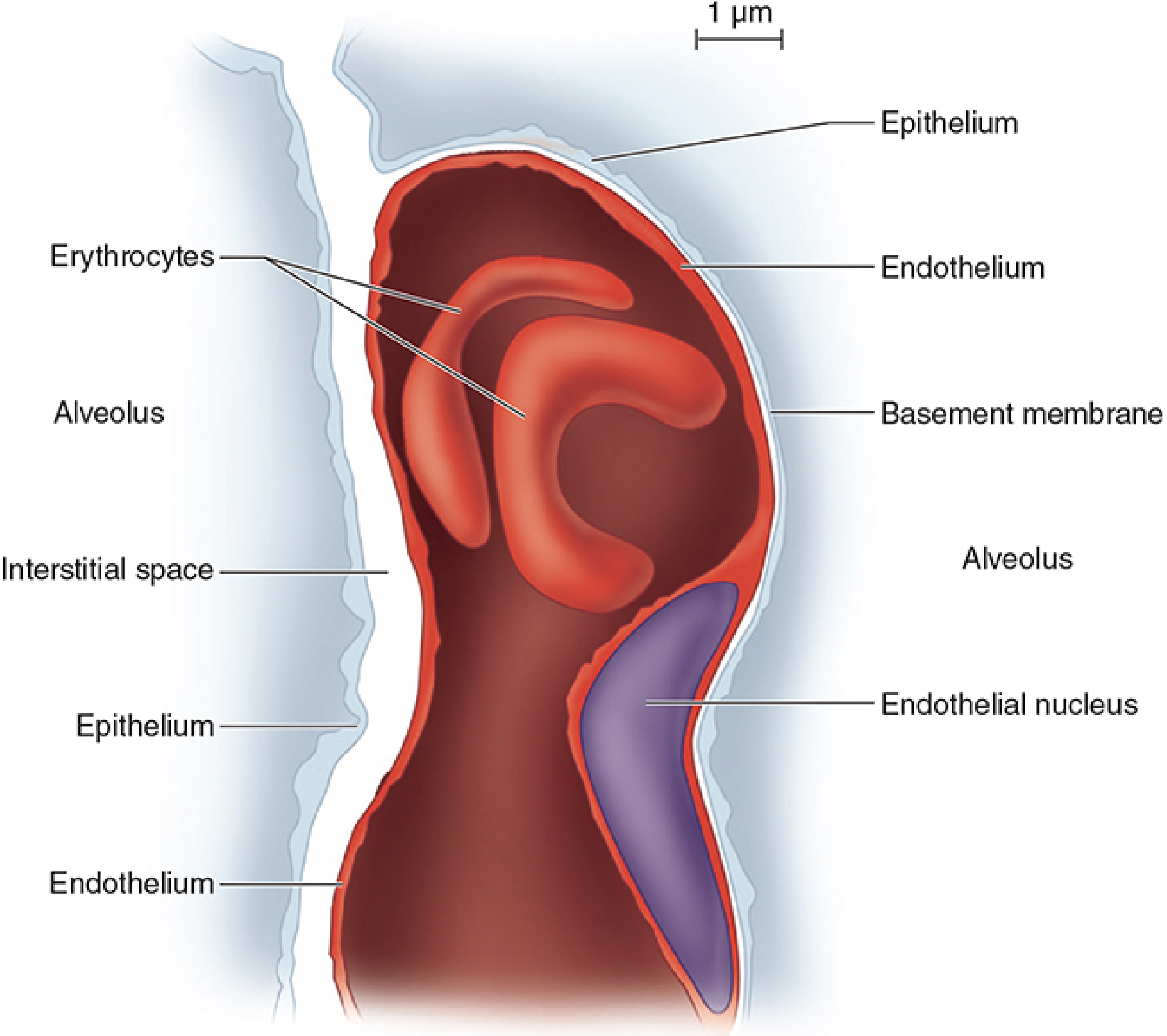
- Thin side (<0.4 μm thick): alveolar epithelium + fused basement membranes + capillary endothelium - this is where O2 and CO2 diffuse
- Thick side (1-2 μm): contains a true pulmonary interstitial space (elastin, collagen, nerve fibers) - where fluid and solute exchange occurs; provides structural support
Alveolar Cell Types
| Cell | Features |
|---|---|
| Type I pneumocytes | Flat, thin; form tight junctions (1-nm gaps) preventing passage of albumin; cover ~95% of alveolar surface area |
| Type II pneumocytes | Cuboidal, round; contain lamellar bodies (surfactant storage); more numerous but occupy <10% of surface; can divide and regenerate Type I cells |
| Alveolar macrophages | Resident scavengers in the air space; activated to secrete cytokines; cleared via mucociliary escalator or into interstitium |
| Mast cells, lymphocytes | Immune surveillance |
Surfactant
Produced and secreted by Type II pneumocytes. Reduces alveolar surface tension, preventing alveolar collapse (atelectasis) at low lung volumes. Composed primarily of dipalmitoylphosphatidylcholine (DPPC).
5. Pulmonary Circulation and Lymphatics
Dual Blood Supply
The lungs receive blood from two circulations:
1. Pulmonary circulation (gas exchange):
- The pulmonary artery from the right ventricle carries deoxygenated blood, divides into right and left branches supplying each lung
- Blood passes through the pulmonary capillaries (O2 taken up, CO2 eliminated)
- Four pulmonary veins (2 from each lung) return oxygenated blood to the left atrium
- Pulmonary arteries and veins have thinner walls with less smooth muscle than systemic vessels
- Normal mean pulmonary arterial pressure: ~15 mmHg (much lower than systemic ~100 mmHg)
2. Bronchial circulation (nutrition):
- Arises from the thoracic aorta and intercostal arteries
- Supplies <4% of cardiac output
- Sustains metabolic needs of the tracheobronchial tree down to the terminal bronchioles
- Anastomoses with pulmonary arterial circulation along the airways
Alveolar vs. Extra-alveolar Vessels
- Extra-alveolar vessels lie in loose peribronchovascular connective tissue; expand as lung volume increases
- Alveolar vessels (capillaries) lie within the alveolar walls and are subject to alveolar pressure
Pulmonary Lymphatics
Pulmonary lymphatics run in two main networks:
- Superficial (pleural) network - along visceral pleura
- Deep (peribronchial) network - along airways and blood vessels
Lymph drains to hilar and mediastinal lymph nodes. The lymphatic system plays a key role in removing excess fluid from the interstitium, preventing pulmonary edema.
6. Rib Cage and Muscles of Respiration
Rib Cage
- Contains both lungs, each surrounded by its own pleura
- The apex allows entry of the trachea, esophagus, and great vessels
- The base is formed by the diaphragm
- Each rib (except the last two) articulates posteriorly with a vertebra and is angulated downward as it attaches anteriorly to the sternum; upward and outward rib movement expands the chest
Primary Muscles of Inspiration
| Muscle | Action |
|---|---|
| Diaphragm | Principal pulmonary muscle; contracts and descends 1.5-7 cm; accounts for 75% of chest volume change |
| External intercostals | Elevate and expand the rib cage |
Accessory Muscles of Inspiration (recruited during increased demand)
- Sternocleidomastoid - elevates the rib cage
- Scalene muscles - prevent inward displacement of upper ribs
- Pectoralis muscles - assist chest expansion when arms are on a fixed support
Muscles of Expiration
- Expiration is passive during normal breathing (elastic recoil of the lung and chest wall)
- Becomes active in the upright position and with increased effort:
- Abdominal muscles (rectus abdominis, external and internal oblique, transversus) - compress the abdomen and assist downward movement of the ribs
- Internal intercostals - aid downward rib movement
7. Neural Control of Respiration (Ventilatory Pump)
Central Nervous System Controllers
- Cerebral cortex (parietal cortex): controls voluntary breathing; projects to motor neurons via corticospinal tracts
- Brainstem: controls automatic breathing
- Pontine center (pneumotaxic center): fine-tunes rhythm
- Dorsal respiratory group (DRG) in medulla: drives inspiration
- Ventral respiratory group (VRG) in medulla: active in both inspiration and expiration
Spinal Cord Pathways
- Corticospinal tract - carries voluntary breathing signals
- Reticulospinal tract - carries automatic breathing signals
- These are separate pathways; damage to one can preserve the other (explains "Ondine's curse" - loss of automatic breathing while voluntary is preserved)
Motor Innervation of Respiratory Muscles
| Muscle | Innervation |
|---|---|
| Diaphragm | Phrenic nerve (C3, C4, C5) |
| Intercostal muscles | Intercostal nerves (T1-T11) |
| Accessory muscles | Cranial nerves XI (SCM), C2-C4 (scalene) |
| Abdominal muscles | T7-L1 |
Feedback Mechanisms
- Central chemoreceptors (medullary ventral surface): respond primarily to changes in cerebrospinal fluid pH/PCO2
- Peripheral chemoreceptors (carotid and aortic bodies): respond to hypoxemia (PaO2 <60 mmHg), hypercapnia, and acidosis
- Pulmonary stretch receptors: in airway smooth muscle; Hering-Breuer reflex (inhibit inspiration when lung is over-inflated)
- J-receptors (juxtacapillary receptors): in alveolar walls; respond to pulmonary edema and embolism, causing rapid shallow breathing and dyspnea
8. Cellular Anatomy of the Airway Wall
Conducting Airway Epithelium (Pseudostratified columnar)
| Cell Type | Function |
|---|---|
| Ciliated columnar cells | Beat in coordinated fashion to move mucus toward the mouth (mucociliary escalator) |
| Goblet cells | Secrete mucin; intermixed with ciliated cells |
| Basal cells | Progenitor cells; replenish ciliated and goblet cells |
| Clara (Club) cells | Secretory; produce surfactant proteins and oxidative enzymes; progenitor role in bronchioles |
| Pulmonary neuroendocrine cells | O2 sensors; release hormones affecting smooth muscle (VIP, substance P); contain dense-cored vesicles with serotonin, dopamine, bombesin; <1% of airway cells |
| Ionocytes | Rare; primary source of CFTR (cystic fibrosis transmembrane conductance regulator) activity |
| Brush (tuft) cells | Blunt microvilli; putative chemosensory role |
Bronchial Wall Layers (from lumen outward)
- Mucosa - epithelium + basement membrane
- Lamina propria - contains lymphoid tissue, mast cells, and immune cells
- Smooth muscle - arranged in spiral bands; regulates airway diameter
- Submucosa - contains seromucous glands (between smooth muscle bands and cartilaginous plates)
- Cartilaginous plates (in bronchi only)
- Adventitia
9. Connective Tissue Framework (Elastic Continuum)
The lung's structural integrity depends on a network of connective tissue fibers:
- Collagen fibers: provide tensile strength, resist overdistension
- Elastin fibers: provide elastic recoil, allow the lung to return to its resting volume after inspiration
- Glycosaminoglycans (proteoglycans): form a gel-like matrix in the interstitium; also regulate epithelial cell phenotype, cytokine signaling, and cell behavior
Three fiber systems form the "elastic continuum":
- Axial fibers: from the hilum outward along airways and blood vessels
- Peripheral fibers: from the visceral pleura inward
- Parenchymal fibers: interconnect the alveolar walls
Summary: Functional Zones
| Zone | Components | Function |
|---|---|---|
| Conducting zone | Nose → trachea → bronchi → terminal bronchioles (Gen 0-16) | Air conduction, warming, humidification, filtration (anatomical dead space ~150 mL) |
| Transitional zone | Respiratory bronchioles (Gen 17-19) | Both conduction and gas exchange |
| Respiratory zone | Alveolar ducts, alveolar sacs, alveoli (Gen 20-23) | Gas exchange (O2/CO2) across ~50-100 m² surface |
References:
- Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume - Chapters 1 (Anatomy) and 130 (Neuromuscular)
- Morgan & Mikhail's Clinical Anesthesiology, 7e - Chapter 23 (Functional Respiratory Anatomy)
classification of pneumonia
Reading File
Finding Sources
Finding Sources
Searching PubMed
pneumonia classification community hospital acquired
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive textbook data from multiple authoritative sources. Let me compile the complete classification.
Classification of Pneumonia
Pneumonia is an infection/inflammation of the lung parenchyma. It can be classified by several different schemes: epidemiological setting, causative agent (etiology), anatomical/radiological pattern, host immune status, severity, and specific clinical syndromes. All major systems are complementary and are used together in clinical practice.
I. Classification by Epidemiological Setting (Most Clinically Used)
This is the most important classification because it predicts the likely pathogens and guides empiric antibiotic therapy.
1. Community-Acquired Pneumonia (CAP)
Pneumonia presenting before hospital admission or within 48 hours of admission in a person who has not been recently hospitalized.
- Most common serious infectious cause of hospitalization and death in the United States
- Hospitalization rates increase exponentially with age (1-2/1000 in young adults vs. ~40/1000 in adults >85 years)
- Seasonal peaks November-March, coinciding with influenza and respiratory viral activity
Common pathogens by clinical setting:
| Clinical Category | Key Pathogens |
|---|---|
| Outpatient, no comorbidities | S. pneumoniae, M. pneumoniae, C. pneumoniae, H. influenzae, respiratory viruses |
| Outpatient, with cardiopulmonary disease | All of the above + DRSP, enteric Gram-negatives, anaerobes (aspiration) |
| Inpatient (non-ICU), with comorbidities | S. pneumoniae (incl. DRSP), H. influenzae, M. pneumoniae, C. pneumoniae, enteric Gram-negatives, viruses, Legionella |
| Severe CAP (ICU), no Pseudomonas risk | S. pneumoniae, Legionella, H. influenzae, enteric Gram-negatives, S. aureus, M. pneumoniae, respiratory viruses |
| Severe CAP (ICU), with Pseudomonas risk | All above + P. aeruginosa |
DRSP = Drug-resistant S. pneumoniae
2. Hospital-Acquired Pneumonia (HAP)
Pneumonia developing ≥48 hours after hospital admission, not incubating at the time of admission.
- Incidence: 5-10 cases per 1000 hospital admissions
- Second most common cause of hospital-acquired infection
- Caused predominantly by multidrug-resistant (MDR) organisms
Common pathogens:
- S. aureus (10-20%; 50% of which are MRSA)
- Pseudomonas aeruginosa (10-20%; 28-35% resistant to cefepime)
- Enteric Gram-negative bacilli (20-40%; 19-29% resistant to piperacillin-tazobactam)
- Acinetobacter baumannii (5-10%; 56-61% resistant to carbapenems)
3. Ventilator-Associated Pneumonia (VAP)
A subtype of HAP occurring ≥72 hours (3 days) after the start of mechanical ventilation.
- Occurs in 16% of patients ventilated for more than 1 day
- Overall mortality ~13%
- The CDC/NHSN defines a surveillance algorithm with escalating categories:
| Category | Timing | Criteria |
|---|---|---|
| VAC (Ventilator-associated condition) | After ≥2 days of stability | FiO2 increase ≥0.20 OR PEEP increase ≥3 cm H2O, sustained ≥2 days |
| IVAC (Infection-related VAC) | ≥3 days MV, within 2 days of worsening oxygenation | Temperature >38°C or <36°C, or WBC ≥12 or ≤4, AND new antibiotic ≥4 days |
| Possible VAP | - | Purulent secretions (≥25 neutrophils, ≤10 squamous epithelial cells) |
| Probable VAP | - | Positive quantitative cultures meeting threshold |
4. Healthcare-Associated Pneumonia (HCAP) - Historical
Previously recognized as a separate category for patients with recent healthcare exposure (hemodialysis, chemotherapy, nursing home residence, hospitalization ≥2 days in past 90 days). The 2016 IDSA/ATS guidelines removed HCAP as a separate category because it over-predicted MDR risk and led to over-treatment. These patients are now stratified within CAP or HAP based on validated risk factors (prior MDR isolation, structural lung disease, recent IV antibiotics).
Risk factors for MDR organisms in CAP now include:
- Hospitalization ≥2 days in the past 90 days
- Broad-spectrum antibiotics within past 3 months
- Immune suppression / corticosteroids
- Prior respiratory isolation of MRSA or P. aeruginosa
- Residence in a nursing home / long-term care facility
II. Classification by Causative Agent (Etiological)
A. Bacterial Pneumonia
| Organism Type | Examples |
|---|---|
| Gram-positive | Streptococcus pneumoniae (most common), Staphylococcus aureus (incl. CA-MRSA), Streptococcus pyogenes |
| Gram-negative | Haemophilus influenzae, Klebsiella pneumoniae, Pseudomonas aeruginosa, Acinetobacter, enteric bacilli (E. coli, Enterobacter) |
| Atypical bacteria | Mycoplasma pneumoniae, Chlamydophila pneumoniae, Legionella pneumophila |
| Anaerobes | Bacteroides, Fusobacterium, Peptostreptococcus (mainly in aspiration) |
| Mycobacteria | M. tuberculosis, non-tuberculous mycobacteria (NTM) |
B. Viral Pneumonia
- Influenza A and B (most common in adults)
- SARS-CoV-2 (COVID-19 pneumonia)
- Respiratory syncytial virus (RSV) - especially in elderly and immunocompromised
- Parainfluenza, adenovirus, human metapneumovirus
- Cytomegalovirus (CMV) - in immunocompromised
C. Fungal Pneumonia
- Endemic fungi: Histoplasma capsulatum, Coccidioides immitis, Blastomyces dermatitidis
- Opportunistic fungi: Pneumocystis jirovecii (PCP - in HIV/AIDS, CD4 <200), Aspergillus, Candida, Cryptococcus neoformans
- Pneumocystis jirovecii: ubiquitous organism; colonizes >50% of adults; causes diffuse, bilateral, subacute but severe pneumonia in immunocompromised patients
D. Parasitic Pneumonia
- Toxoplasma gondii, Strongyloides stercoralis, Paragonimus spp.
- Generally seen in immunocompromised or tropical settings
III. Classification by Anatomical / Radiological Pattern
1. Lobar Pneumonia
- Consolidation involving an entire lobe or major segment
- Classic example: Streptococcus pneumoniae
- Pathological stages: congestion → red hepatization → grey hepatization → resolution
- Radiograph: homogeneous lobar or segmental consolidation, often with air bronchograms
2. Bronchopneumonia (Lobular Pneumonia)
- Patchy, multifocal consolidation centered on bronchioles, spreading to alveoli
- Bilateral, often basal predominance
- Common with S. aureus, Gram-negative bacilli, H. influenzae
- Often seen in debilitated patients, the elderly, post-surgical patients, and aspiration
3. Interstitial Pneumonia (Atypical Pneumonia Pattern)
- Inflammation primarily in the interstitium (walls of alveoli and bronchioles)
- Bilateral, diffuse, reticulonodular or ground-glass pattern on chest X-ray
- Classic "atypical" organisms: Mycoplasma pneumoniae, Chlamydophila, Legionella, viruses
- May also be seen with Pneumocystis jirovecii (bilateral perihilar ground-glass)
IV. Classification by Typical vs. Atypical Presentation
| Feature | Typical Pneumonia | Atypical Pneumonia |
|---|---|---|
| Onset | Abrupt | Gradual |
| Symptoms | High fever, rigors, productive purulent cough, pleuritic pain | Low-grade fever, dry/non-productive cough, headache, myalgias |
| Organisms | S. pneumoniae, S. aureus, H. influenzae, Gram-negatives | Mycoplasma, Chlamydophila, Legionella, viruses |
| Radiology | Lobar consolidation | Interstitial/diffuse bilateral infiltrates |
| WBC | Markedly elevated (leukocytosis) | Normal or mildly elevated |
| Response to beta-lactams | Good | Poor (need macrolide/fluoroquinolone) |
Note: The typical/atypical distinction is a clinical guide, not absolute. Legionella is "atypical" by organism but can present quite severely with lobar consolidation. Co-infections are also common.
V. Classification by Host Immune Status
Immunocompetent Host
Standard CAP, HAP, or VAP organisms as described above.
Immunocompromised Host
A special category requiring broader differential:
- HIV/AIDS (CD4 <200): Pneumocystis jirovecii, Cryptococcus, CMV, M. tuberculosis, MAC
- Neutropenic patients (chemotherapy, hematologic malignancy): Aspergillus spp., Candida, Gram-negative bacilli, Mucor
- Solid organ transplant: CMV, Aspergillus, Pneumocystis jirovecii, Nocardia
- Corticosteroid therapy: Aspergillus, P. jirovecii, atypical mycobacteria
VI. Classification by Severity (Site-of-Care Decision)
CURB-65 Score (simpler, commonly used)
One point each for:
| Variable | Criterion |
|---|---|
| C - Confusion | New-onset confusion |
| U - Urea | Blood urea >7 mmol/L (>19 mg/dL) |
| R - Respiratory rate | ≥30 breaths/min |
| B - Blood pressure | Systolic ≤90 mmHg or diastolic ≤60 mmHg |
| 65 - Age | ≥65 years |
| Score | Recommended Action | 30-day Mortality |
|---|---|---|
| 0 | Outpatient | ~1.5% |
| 1-2 | Consider hospitalization | ~5-9% |
| ≥3 | Hospital/ICU | ~22% |
Pneumonia Severity Index (PSI / PORT Score)
- Stratifies by 20 variables (age, comorbidities, vital signs, labs, imaging)
- Five classes: Class I-II (outpatient), Class III (borderline - observation), Class IV-V (hospital/ICU)
- Mortality: Class I = 0.1%; Class II = 0.6%; Class III = 2.8%; Class IV = 8.2%; Class V = 29.2%
- More validated than CURB-65 but more complex to calculate
IDSA/ATS Severe CAP Criteria
Requires 1 major criterion OR ≥3 minor criteria for ICU admission:
Major criteria:
- Hypotension requiring vasopressors (septic shock)
- Respiratory failure requiring mechanical ventilation
Minor criteria:
- Respiratory rate ≥30 breaths/min
- PaO2/FiO2 ≤250
- Multilobar infiltrates
- Confusion/disorientation
- BUN ≥20 mg/dL (uremia)
- WBC <4000 cells/µL (leukopenia)
- Platelet count <100,000/µL
- Core temperature <36°C (hypothermia)
- Hypotension requiring IV fluid resuscitation
VII. Special Clinical Syndromes
Aspiration Pneumonia
- Caused by macroaspiration of oropharyngeal contents (often less virulent organisms requiring a large inoculum)
- Distinguished from aspiration pneumonitis (chemical inflammation from gastric acid without infection - usually rapid recovery)
- Risk factors: stroke, esophageal disorders, impaired consciousness, alcoholism, poor dentition, acid-suppressive medications
- Community setting: normal oral flora - anaerobes, Streptococcus species
- Hospital setting: nosocomial organisms added - Gram-negative bacilli, S. aureus
- Typically affects dependent segments: posterior segment of right upper lobe (supine) and right lower lobe (upright)
- Complications: necrotizing pneumonia, lung abscess (cavity >1 cm), empyema - especially with anaerobes, S. aureus, Klebsiella, Pseudomonas
Necrotizing Pneumonia / Lung Abscess
- Multiple cavities ≤1 cm = necrotizing pneumonia
- One or more cavities >1 cm communicating with a bronchus = lung abscess
- Organisms: anaerobes (indolent), S. aureus, Klebsiella pneumoniae, P. aeruginosa (acute)
- CA-MRSA can cause a severe, necrotizing post-influenza pneumonia via exotoxin (Panton-Valentine leukocidin)
Summary Diagram
PNEUMONIA
│
├── By SETTING
│ ├── Community-Acquired (CAP)
│ ├── Hospital-Acquired (HAP) - ≥48h after admission
│ └── Ventilator-Associated (VAP) - ≥72h after intubation
│
├── By ETIOLOGY
│ ├── Bacterial (typical & atypical)
│ ├── Viral
│ ├── Fungal
│ └── Parasitic
│
├── By ANATOMY / RADIOLOGY
│ ├── Lobar (consolidation)
│ ├── Bronchopneumonia (patchy/lobular)
│ └── Interstitial (diffuse bilateral)
│
├── By HOST
│ ├── Immunocompetent
│ └── Immunocompromised (HIV, neutropenic, transplant)
│
├── By SEVERITY
│ ├── Non-severe (outpatient/ward)
│ └── Severe (ICU) — CURB-65 ≥3 or IDSA/ATS criteria
│
└── Special Syndromes
├── Aspiration pneumonia / pneumonitis
├── Necrotizing pneumonia / lung abscess
└── Opportunistic pneumonia (PCP, Aspergillus, CMV)
Sources:
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set - Ch. 122, 125
- Goldman-Cecil Medicine, International Edition - Ch. 84
- Current Surgical Therapy, 14e - Hospital-Acquired and Ventilator-Associated Pneumonia
- Harrison's Principles of Internal Medicine, 22e - Community-Acquired Pneumonia
- Frameworks for Internal Medicine - Aspiration Pneumonia
This is a shared conversation. Sign in to Orris to start your own chat.