Hernia related to surgery and anatomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a comprehensive overview of hernias from a surgical and anatomical perspective, drawn from multiple surgical textbooks.
Hernias: Surgical and Anatomical Overview
Definition
A hernia is the protrusion of any viscus from its normal cavity through an abnormal opening. Abdominal hernias involve intraabdominal contents (usually bowel or omentum) pushing through a defect in the abdominal wall musculature. This weakness may arise from a congenital tract that failed to close, aging with loss of tissue elasticity, increased intraabdominal pressure, failed wound healing, or trauma.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
Classification by Reducibility
| State | Definition |
|---|---|
| Reducible | Contents return through the fascial defect without surgery |
| Incarcerated | Contents are irreducible without surgery; not inherently an emergency if chronic |
| Strangulated | Incarcerated hernia with compromised blood supply - a surgical emergency |
Hernias with a small neck are most likely to become incarcerated or strangulated. Strangulation leads to tissue ischemia and necrosis if blood flow is not restored.
- Mulholland and Greenfield's Surgery, 7e
Types of Hernia by Location
1. Inguinal Hernias (75% of all hernias)
Inguinal hernias lie within the inguinal triangle, bounded by the inguinal ligament inferiorly, the inferior epigastric artery superolaterally, and the lateral edge of the rectus abdominis medially.
Anatomy of the inguinal canal:
Key structures include the iliopubic tract (an aponeurotic band from the anterior superior iliac spine inserting into Cooper's ligament), the lacunar ligament (ligament of Gimbernat), Cooper's (pectineal) ligament (fused to the periosteum of the pubic tubercle), and the conjoined tendon (fusion of inferior fibers of internal oblique and transversus abdominis at the pubic tubercle).
Indirect inguinal hernia:
- The hernial orifice is lateral to the inferior epigastric vessels, through the deep inguinal ring
- The sac passes along the inguinal canal (and may reach the scrotum)
- Can be congenital (patent processus vaginalis) or acquired
- Hernial sac layers: parietal peritoneum + transversalis fascia + cremaster muscle
- Most common groin hernia; predominant in children and young adults
Direct inguinal hernia:
- Hernial orifice is medial to the inferior epigastric vessels, within Hesselbach's triangle
- Borders of Hesselbach's triangle: inguinal ligament (inferior), lateral edge of rectus sheath (medial), inferior epigastric vessels (superolateral)
- The sac consists only of parietal peritoneum and transversalis fascia (no cremaster)
- Acquired, not congenital; more common with age
Pantaloon hernia: A combination of both direct and indirect hernias straddling the inferior epigastric vessels.
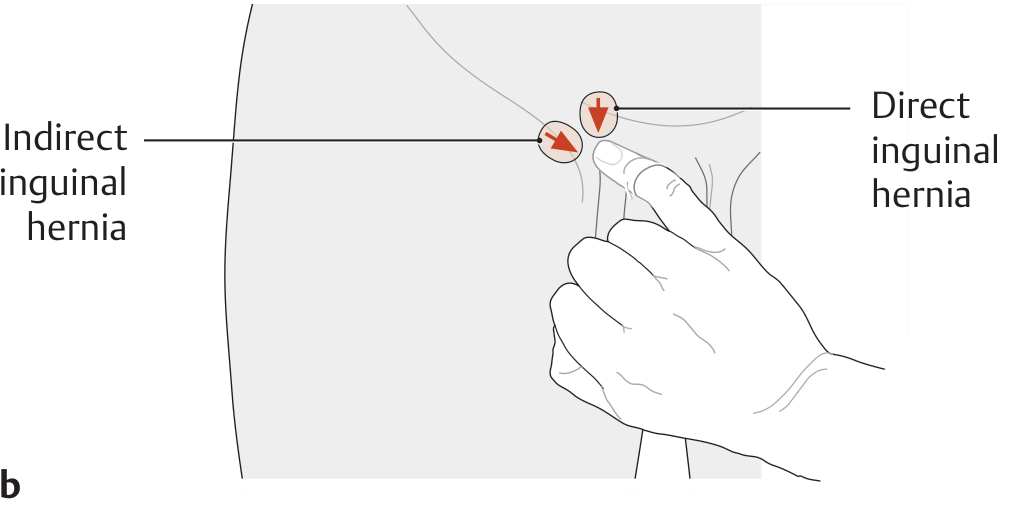
Three-finger rule: With the thenar eminence on the ASIS, the index finger points to a direct hernia, the middle finger to an indirect hernia, and the ring finger to a femoral hernia.
- THIEME Atlas of Anatomy; Schwartz's Principles of Surgery, 11e
2. Femoral Hernia
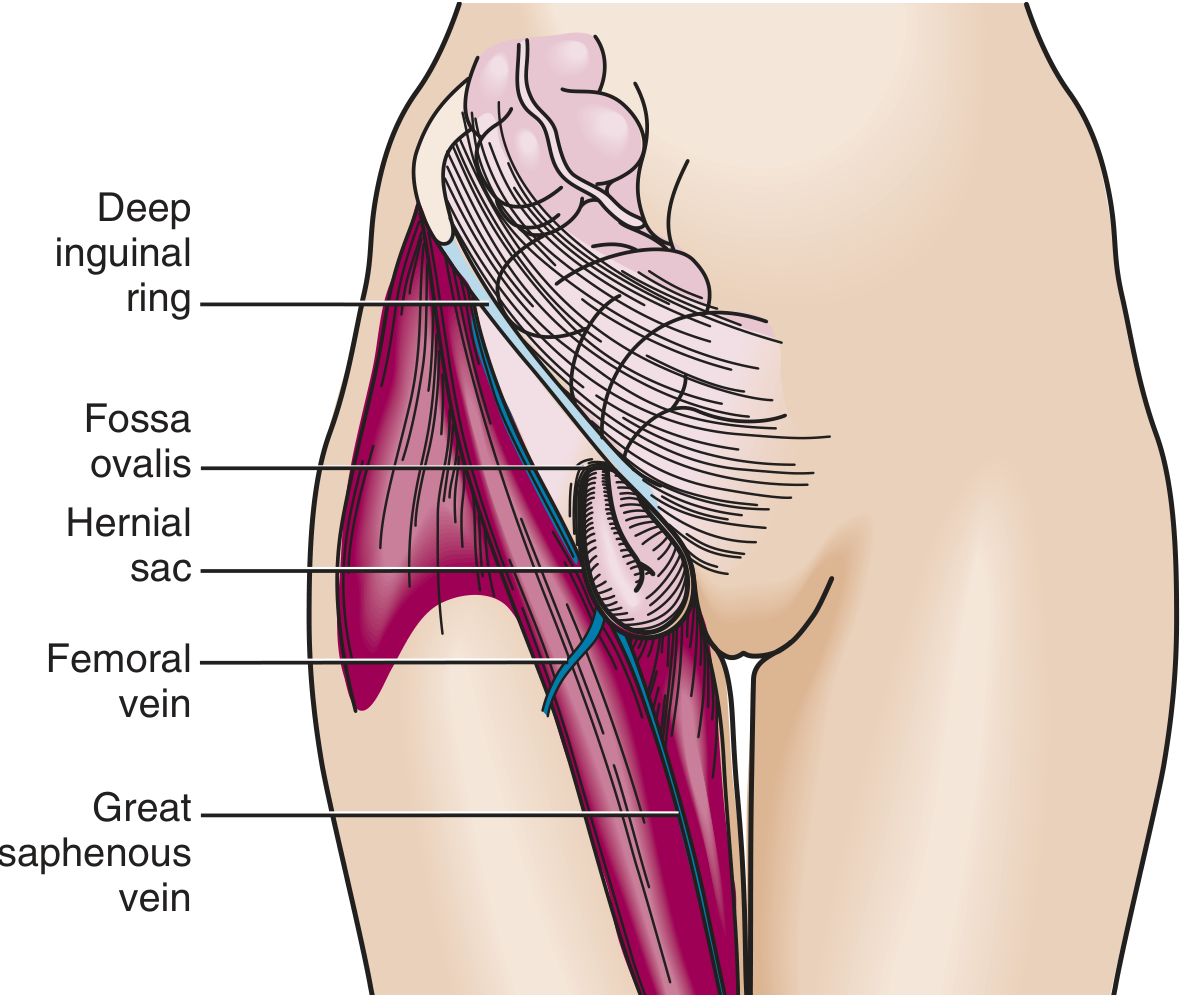
- Occurs inferior to the inguinal ligament through a defect in the transversalis fascia
- Contents protrude into the femoral canal: medial to the femoral vein, lateral to the lacunar ligament
- Borders of the femoral ring: iliopubic tract and inguinal ligament (anterior), Cooper's ligament (posterior), lacunar ligament (medial), femoral vein (lateral)
- Appears as a medial thigh mass below where direct and indirect hernias are found
- Incarceration risk up to 45% due to the small, rigid fascial defect
- More common in women; uncommon in children
- Roberts and Hedges'; Schwartz's Principles of Surgery, 11e
3. Ventral Hernias
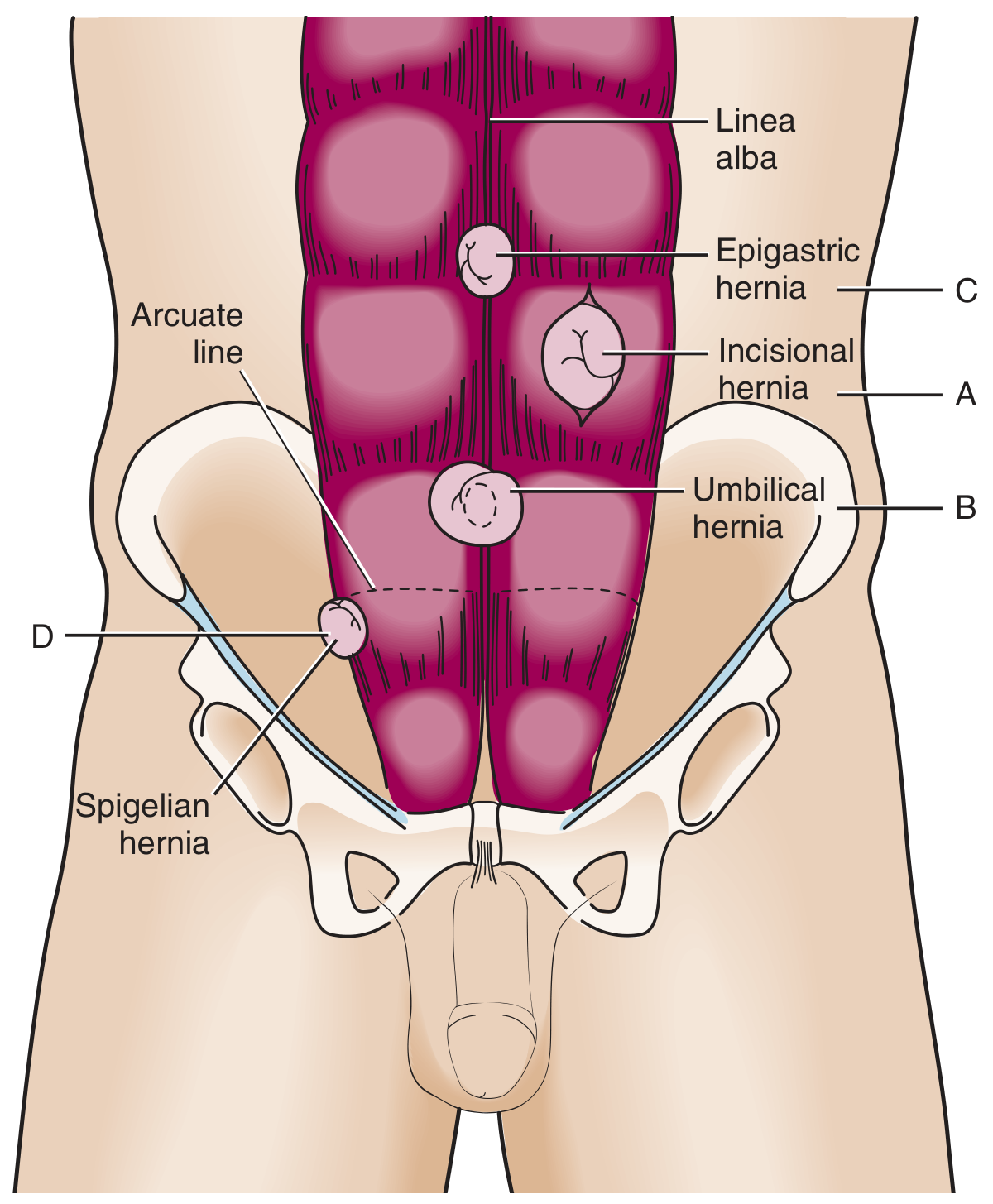
A - Incisional Hernia (Surgical Hernia)
Occurs at a previous surgical wound site. Incisional hernias develop in up to 20% of patients following abdominal surgery. Recurrence rates after repair are 20-50%. The midline is the most common location since most incisions traverse the linea alba.
Risk factors:
- Patient factors: obesity, diabetes, active smoking, old age, female gender, prior laparotomy, collagen dysfunction
- Operative factors: emergent surgery, high wound class, significant blood loss, delayed fascial closure, laparoscopic port site enlargement
- Postoperative factors: surgical site infection (SSI), wound dehiscence
Paramedian and transverse incisions carry a lower hernia risk than midline incisions. Port-site hernias after laparoscopy occur in 1.5-1.8% of cases.
- Fischer's Mastery of Surgery, 8e
B - Umbilical Hernia
- Traverses the fibromuscular ring of the umbilicus
- Most common in infants/children (congenital, often resolves by age 5)
- Acquired adult umbilical hernias are associated with obesity, ascites, or pregnancy
- Adults have higher incarceration and strangulation risk than children
C - Epigastric Hernia
- Through the linea alba between the xiphoid and umbilicus
- Usually small, containing preperitoneal fat in adults
D - Spigelian Hernia
- At the lateral edge of the rectus muscle at the semilunar line, most commonly below the arcuate line
- Incidence 0.12-2.4% of all abdominal wall hernias
- Often a partial-thickness/intraparietal hernia (external oblique remains intact); the hernia penetrates only the transversus abdominis and internal oblique
- Acquired, not congenital; may be confused with port-site incisional hernias
Clinical Diagnosis
- Patients typically present with a palpable lump, often painless or causing a heavy ache
- Sharp/intermittent pain suggests tissue pinching at the neck; severe pain suggests strangulation
- Expansile cough impulse on palpation is characteristic (absent with tight or femoral hernias)
- Examine with patient lying, then standing; use Valsalva maneuver
- Contralateral occult hernias are present in up to 20% of groin hernia patients
- Key questions: Is the hernia primary, recurrent, or incisional? Is it reducible?
- Bailey and Love's Short Practice of Surgery, 28e
Incisional Hernia: Surgical Anatomy and Prevention
The strongest layer of the abdominal wall for closure is the linea alba - a tendinous/fibrous structure formed by the fusion of bilateral anterior and posterior rectus sheath collagenous layers. The oblique abdominal muscles generate forces perpendicular to the healing linea alba, increasing wound dehiscence and hernia risk after midline laparotomy.
Key surgical principles:
- Drains and ostomies should not exit through the midline incision
- Suture material and technique are the most important modifiable determinants of hernia risk
- Prophylactic mesh augmentation (PMA) of fascial closure can be considered for high-risk patients
- Fischer's Mastery of Surgery, 8e
Surgical Treatment
General principles:
- Contaminated cases (e.g., bowel necrosis from strangulation) preclude mesh repair; tissue-based repair is used instead
- Mesh-based repair is recommended for adult inguinal hernias
- The Lichtenstein flat-mesh technique is the gold standard for open anterior repair
- Shouldice technique is preferred when mesh is not used
- Minimally invasive (MI) techniques (TEP - totally extraperitoneal, or TAPP - transabdominal preperitoneal) are preferred for bilateral hernias, femoral hernias, and in females (due to higher femoral hernia incidence)
- For recurrent hernias, the approach should be from the opposite side (posterior after failed anterior, and vice versa)
Complications of hernia repair:
-
Seroma/hematoma (overall complication rate 5-10%)
-
Surgical site infection
-
Chronic pain
-
Recurrence
-
Sabiston Textbook of Surgery; Fischer's Mastery of Surgery, 8e
Complications of Untreated Hernia
Hernia accident (obstruction or strangulation) - historically used to justify prophylactic repair. However, randomized controlled trials have shown that watchful waiting is safe for asymptomatic inguinal hernias in men.
For reduction of an acutely incarcerated hernia, the maneuver of taxis is used: grasp the neck with one hand and apply intermittent gentle pressure on the distal hernia with the other to elongate the neck and guide contents back. Trendelenburg position aids reduction of groin hernias. Taxis should NOT be done with suspected strangulation (risk of reducing gangrenous bowel into the abdomen).
- Mulholland and Greenfield's Surgery, 7e
Summary Table
| Hernia Type | Location | Relation to Epigastric Vessels | Common in | Key Risk |
|---|---|---|---|---|
| Indirect inguinal | Deep inguinal ring | Lateral | Young males | Patent processus vaginalis |
| Direct inguinal | Hesselbach's triangle | Medial | Older males | Acquired weakness |
| Femoral | Femoral canal (below inguinal lig.) | - | Women | 45% incarceration rate |
| Incisional | Prior surgical wound | - | Post-surgery patients | Up to 20% of laparotomies |
| Umbilical | Umbilical ring | - | Infants, obese adults | Strangulation (adults) |
| Epigastric | Linea alba (xiphoid to umbilicus) | - | Adults | Usually small/fat-containing |
| Spigelian | Semilunar line below arcuate line | - | Adults | Missed diagnosis (intraparietal) |
Blood transfusion and it complications related to surgery
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive material from multiple textbooks. Here is the full structured response:
Blood Transfusion and Its Complications in Surgery
Definition and Overview
Blood transfusion is the administration of blood or blood components to restore circulating volume, correct anemia, or reverse coagulopathy in the surgical patient. While life-saving in acute hemorrhage, transfusion carries significant risks that must be weighed carefully against its benefits.
- Bailey and Love's Short Practice of Surgery, 28e
Blood Products Used in Surgery
| Product | Description | Key Use |
|---|---|---|
| Packed Red Blood Cells (PRBCs) | Whole blood minus plasma; Hct 55-65%; shelf life 42 days | Restore O₂-carrying capacity |
| Fresh Frozen Plasma (FFP) | Acellular plasma; contains all clotting factors | Coagulopathy, warfarin reversal, INR >1.5 |
| Platelets | Stored at room temperature; shortest shelf life | Bleeding with platelets <50,000/μL (or <100,000/μL for neurologic hemorrhage) |
| Cryoprecipitate | Rich in fibrinogen, factor VIII, vWF | Low fibrinogen, DIC |
| Whole Blood | Standard in trauma/military; refrigerated up to 35 days | Hemorrhagic shock with hemorrhage control |
Over 90% of all transfusions use blood components rather than whole blood. Each unit of PRBC is leukoreduced (LR-PRBC) in most hospitals - donor leukocytes have been linked to acute and chronic complications including immunosuppression and infection.
- Fischer's Mastery of Surgery, 8e
Indications for Transfusion
- Acute blood loss - to replace circulating volume and maintain oxygen delivery
- Perioperative anemia - to ensure adequate oxygen delivery during the perioperative phase
- Symptomatic chronic anemia - without hemorrhage or impending surgery
Transfusion Trigger (Hemoglobin Threshold)
The historical threshold of Hb >10 g/dL has been abandoned. A restrictive transfusion strategy is now standard:
| Hemoglobin (g/dL) | Recommendation |
|---|---|
| < 6 | Probably will benefit from transfusion |
| 6 - 8 | Unlikely to benefit in absence of bleeding or impending surgery |
| > 8 | No indication in absence of other risk factors |
- For patients with coronary artery disease (CAD): transfuse to maintain Hb ≥ 9 g/dL
- For neurologic hemorrhage: maintain platelets >100,000/μL
- Bailey and Love's Short Practice of Surgery, 28e; Rosen's Emergency Medicine
Blood Groups and Cross-Matching
ABO System
| Phenotype | Antigens | Antibodies | Frequency |
|---|---|---|---|
| O | O | Anti-A, Anti-B | 46% |
| A | A | Anti-B | 42% |
| B | B | Anti-A | 9% |
| AB | AB | None | 3% |
- Group O is the universal donor (no antigens to provoke a reaction)
- Group AB is the universal recipient (no circulating antibodies)
- Group O- is given to females in emergency; O+ to males
Rhesus (Rh) System
- The Rh(D) antigen is present in ~85% of the UK population
- Anti-D antibodies are not naturally present but are formed after transfusion of Rh+ blood
- In Rh(D)-negative pregnant women, anti-D antibodies can cross the placenta and cause hydrops fetalis in a Rh(D)-positive fetus
Cross-Matching Time
- Full cross-match: up to 45 minutes
- Type-specific (ABO/Rh only): 10-15 minutes
- Emergency: uncross-matched O-negative (females) or O-positive (males)
Two healthcare personnel must always verify patient identity and donor blood details before administration to prevent ABO incompatibility errors.
- Bailey and Love's Short Practice of Surgery, 28e
Complications of Blood Transfusion
A. Complications from a Single Transfusion
1. Acute Hemolytic Transfusion Reaction (AHTR)
- Most severe immunologic complication
- Caused by ABO incompatibility - recipient antibodies activate complement and cause intravascular hemolysis
- Risk: ~1:110,000 transfusions
- Can occur after as little as 10-15 mL of incompatible blood
- Symptoms: fever, chills, chest pain, hypotension, flank pain, hemoglobinuria, bleeding diathesis - occurring during or immediately after transfusion
- Consequences: renal failure, DIC, multiple organ failure, death
- Management: Stop transfusion immediately; fluid resuscitation; alkalinize urine (prevents renal tubular hemoglobin precipitation); notify blood bank; send blood samples for re-crossmatch and direct Coombs test
- Goldman-Cecil Medicine; Campbell-Walsh Urology
2. Delayed Hemolytic Transfusion Reaction (DHTR)
- Risk: ~1:32,000 transfusions
- Due to recipient antibodies against minor blood group antigens (non-ABO)
- Occurs days to weeks after transfusion
- Usually milder, self-limiting
3. Febrile Non-Hemolytic Transfusion Reaction (FNHTR)
- Most common transfusion reaction: ~1:1,100
- Caused by cytokines from donor leukocytes (graft-vs-host response)
- Symptoms: fever, chills, rigors during or up to 1-2 hours post-transfusion
- Management: Stop transfusion; rule out hemolytic reaction; antipyretics
- Rare with leukodepleted (leukoreduced) blood
4. Allergic/Anaphylactic Reaction
- Allergic: ~1:1,200; severe (anaphylactic): ~1:15,500
- Due to IgE-mediated reaction to donor plasma proteins
- Ranges from urticaria/pruritis to full anaphylaxis (bronchospasm, hypotension)
- Management: Stop transfusion; antihistamines; epinephrine for anaphylaxis
5. Transfusion-Related Acute Lung Injury (TRALI)
- Incidence: ~1:140,000 transfusions
- Most common cause of transfusion-related fatality (accounted for 55% of transfusion mortality 2005-2007)
- Definition: rapid onset of acute lung injury (ALI) within 6 hours of transfusion
- Mechanism: traditionally attributed to donor leukocyte antibodies against recipient leukocytes; the true mechanism remains uncertain
- Features: non-cardiogenic pulmonary edema, severe hypoxemia, new bilateral infiltrates on CXR; may have transient leukopenia and thrombocytopenia
- Management: Immediately stop transfusion; notify blood bank; supplemental O₂; supportive care - most recover without sequelae
- Differentiated from TACO: TRALI = pulmonary permeability edema (inflammatory); TACO = hydrostatic edema (volume overload)
- Fischer's Mastery of Surgery, 8e; Campbell-Walsh Urology
6. Transfusion-Associated Circulatory Overload (TACO)
- Incidence: ~1:9,000
- Hydrostatic pulmonary edema from volume overload within 6 hours of transfusion
- Risk factors: prior hemorrhagic shock, heart failure, chronic renal failure, positive fluid balance
- Features: respiratory distress, lung crackles, elevated BNP, pulmonary capillary wedge pressure elevation
- Management: Slow/stop transfusion; diuretics (cautiously in ongoing hemorrhagic shock)
- Barash Clinical Anesthesia, 9e
7. Infectious Complications
| Pathogen | Current Risk per Unit (US) | Notes |
|---|---|---|
| HIV | ~1:1,800,000 | Screened by NAT + antibody |
| Hepatitis C | ~1:1,600,000 | Screened by NAT + anti-HCV |
| Hepatitis B | ~1:1,500,000 | Screened by HBsAg + anti-HBc + HBV NAT |
| HTLV | ~1:3,300,000 | Screened by anti-HTLV-I/II |
| Bacterial | ~1:200,000 (platelets most at risk: 1:5,000) | Platelets stored at room temp - highest bacterial contamination risk |
Screening programs using nucleic acid amplification technology (PCR, transcription-mediated amplification) have dramatically reduced viral transmission risks from the unacceptably high rates seen in the 1970s-1980s. Additional platelet mitigation strategies (diversion pouch, bacterial screening, pathogen reduction) have reduced septic reactions by ~two-thirds.
- Goldman-Cecil Medicine; Campbell-Walsh Urology
8. Air Embolism and Thrombophlebitis
- Air embolism: rare with modern closed systems
- Thrombophlebitis at the infusion site
- Bailey and Love's Short Practice of Surgery, 28e
B. Complications from Massive Transfusion
A massive transfusion is generally defined as replacement of >10 units of PRBCs in 24 hours (approximately one blood volume).
| Complication | Mechanism | Management |
|---|---|---|
| Coagulopathy | Dilution of clotting factors and platelets; hyperfibrinolysis | 1:1:1 ratio (RBC:FFP:platelets); tranexamic acid; cryoprecipitate for low fibrinogen |
| Hypocalcemia | Citrate in blood preservative chelates ionized calcium; most significant in liver failure | IV calcium gluconate/chloride; monitor ionized Ca²⁺ |
| Hyperkalemia | Potassium leaks from stored RBCs over time (storage lesion) | Cardiac monitoring; treat as needed |
| Hypokalemia | As cells recover post-transfusion, K⁺ re-enters cells | Monitor electrolytes |
| Hypothermia | Cold stored blood (4°C) reduces core temperature | Blood warmers; forced-air warming; warm IV fluids |
| Iron overload | Repeated transfusions over time (each unit contains ~250 mg elemental iron) | Iron chelation therapy (e.g., deferoxamine) in chronic transfusion recipients |
Management of Coagulopathy in Massive Hemorrhage
Damage Control Resuscitation (DCR):
- Deliver 1:1:1 ratio of RBCs : FFP : platelets (approximates whole blood)
- Avoid crystalloids and colloids
- Give tranexamic acid (TXA) empirically as early as possible (antifibrinolytic - inhibits fibrinolysis by binding plasminogen)
- Give cryoprecipitate for low fibrinogen (essential for clot formation and stabilization)
- Guide therapy by point-of-care viscoelastic testing (TEG/ROTEM) and laboratory values (INR, PTT, fibrinogen)
The Massive Transfusion Protocol (MTP) is triggered when >10 units of PRBCs/24h are anticipated. It mobilizes blood bank and hospital resources for rapid balanced product delivery.
The CRASH-2 trial showed a mortality benefit with TXA in hemorrhagic shock, but without a reduction in actual transfusion numbers. Current guidance recommends TXA when point-of-care testing demonstrates hyperfibrinolysis - indiscriminate use may be harmful.
- Bailey and Love's Short Practice of Surgery, 28e; Fischer's Mastery of Surgery, 8e; Rosen's Emergency Medicine
Transfusion-Related Immunosuppression (TRIM)
TRIM was first described in 1973 when pre-operative transfusion improved renal allograft survival. Mechanistically, donor allogeneic leukocytes suppress recipient immunity.
Surgical consequences:
- Increased postoperative bacterial infection
- Increased short-term mortality after surgical procedures
- Increased risk of cancer recurrence after resection of malignancy
Why leukoreduction matters: Universal leukoreduction of PRBCs has been mandatory in most US hospitals for the past two decades. Over 90% of PRBCs now transfused are leukoreduced, which substantially reduces TRIM.
- Fischer's Mastery of Surgery, 8e
Transfusion-Associated Graft-Versus-Host Disease (TA-GvHD)
- Extremely rare: <1:10,000,000
- Donor T-lymphocytes attack recipient tissues
- More common in immunocompromised patients
- Prevented by irradiating blood products for at-risk patients (e.g., stem cell transplant recipients, severe combined immunodeficiency)
Autologous Transfusion Strategies (Blood Conservation)
To minimize the risks of allogeneic transfusion in elective surgery:
| Strategy | Method | Notes |
|---|---|---|
| Preoperative Autologous Donation (PAD) | Patient donates own blood weeks before surgery; stored and re-transfused intraoperatively | Indicated for rare blood types or patients refusing allogeneic blood (e.g., Jehovah's Witnesses); wastage rate up to 45%; risk of preoperative anemia |
| Acute Normovolemic Hemodilution (ANH) | Blood withdrawn immediately preoperatively; replaced with crystalloid; retransfused when needed | Provides fresh whole blood with viable platelets and clotting factors |
| Intraoperative Blood Salvage (Cell Saver) | Blood collected from surgical field, washed and filtered, re-infused as leukoreduced RBCs | Most effective blood conservation technique; cannot be used in contaminated fields (cancer, infection) |
Note: Even autologous blood is not entirely without risk - recipients remain susceptible to TACO, clerical error, bacterial contamination, metabolic derangements, and TRIM.
- Barash Clinical Anesthesia, 9e; Bailey and Love's Short Practice of Surgery, 28e
Risk Summary Table (Non-Infectious Transfusion Events, US)
| Adverse Event | Risk per Unit |
|---|---|
| Febrile non-hemolytic reaction | ~1:1,100 |
| Allergic reaction | ~1:1,200 |
| TACO | ~1:9,000 |
| Hypotensive reaction | ~1:32,000 |
| Delayed hemolytic reaction | ~1:32,000 |
| Acute hemolytic reaction | ~1:110,000 |
| TRALI | ~1:140,000 |
| TA-GvHD | <1:10,000,000 |
- Goldman-Cecil Medicine, International Edition
Key Clinical Principles for Surgeons
- Restrictive transfusion (trigger Hb <7-8 g/dL) reduces morbidity and mortality vs. liberal strategies
- Always verify patient identity and blood product with two personnel before transfusion
- In active hemorrhage: activate MTP early; use 1:1:1 balanced resuscitation; give TXA early
- Stop any transfusion at the first sign of a suspected reaction and initiate workup
- Leukoreduced and irradiated products reduce immune complications
- Overtransfusion is harmful - do not transfuse autologous blood simply to avoid wastage
This is a shared conversation. Sign in to Orris to start your own chat.