
IMG_4555.jpeg
Analyze the ecg.What’s the diagnosis
Reading File
Finding Sources
Finding Sources
Loading Image
I have a clear view of the ECG. Here is my full systematic analysis:
ECG Analysis - Abdul Motin, Male, 51 Years
Patient & Technical Details
- Name: Abdul Motin | Age: 51 years | Sex: Male
- Date/Time: 25-05-2026, 9:32:14 AM
- Machine: GE MAC2000
- Settings: 25 mm/s paper speed, 10 mm/mV gain, 12-lead standard
Measured Parameters (from machine)
| Parameter | Value | Normal |
|---|---|---|
| Heart Rate | 83 bpm | 60-100 bpm ✓ |
| QRS duration | 78 ms | <120 ms ✓ |
| PR interval | 152 ms | 120-200 ms ✓ |
| QT / QTc (Bazett) | 382 / 448 ms | QTc borderline (≤440 ms in males) |
| RR / PP | 722 / 722 ms | Regular ✓ |
| P / QRS / T axis | 54 / 36 / 23 degrees | Normal axis ✓ |
Systematic Lead-by-Lead Analysis
Rhythm:
- Regular rhythm, rate 83 bpm. P waves present and upright in leads I and II - Normal Sinus Rhythm
P waves:
- Normal morphology, normal axis (+54°), duration appears normal. No evidence of atrial enlargement.
PR interval: 152 ms - normal, no heart block.
QRS complexes:
- Duration 78 ms - narrow, no bundle branch block
- Normal axis +36°
- No pathological Q waves identifiable in the visible leads
- No left or right ventricular hypertrophy pattern
ST segments / T waves (the key finding):
- There are nonspecific ST-T wave changes visible across multiple leads
- The T waves appear flattened or with mild morphological changes, consistent with a nonspecific ST-T abnormality
- No clear ST elevation or horizontal/downsloping ST depression that would indicate STEMI or NSTEMI
- No deep symmetric T-wave inversions
QTc: 448 ms - borderline prolonged (upper limit of normal for males is 440 ms; some guidelines use 450 ms). This warrants attention.
Machine Interpretation (confirmed on strip)
Normal sinus rhythm Nonspecific ST abnormality Abnormal ECG
Clinical Interpretation
Primary Diagnosis: Abnormal ECG with Nonspecific ST-T Wave Changes
The machine (GE MAC2000 auto-analysis) and the visual findings agree on:
- Normal sinus rhythm at 83 bpm - no arrhythmia
- Nonspecific ST-T abnormality - this is a non-diagnostic finding that can be caused by multiple conditions:
| Possible Cause | Notes |
|---|---|
| Myocardial ischemia / ACS | Must be ruled out first given age 51, male |
| Hypertensive heart disease | Very common in this age group |
| Electrolyte imbalance (hypokalemia, hypomagnesemia) | Flattened T waves |
| Left ventricular hypertrophy with strain | Review voltage criteria |
| Digoxin or other drug effect | Check medication history |
| Early repolarization variant | Benign, but diagnosis of exclusion |
| Cardiomyopathy | Less common |
- Borderline QTc of 448 ms - check for medications that prolong QT, electrolyte disturbances
What This ECG Does NOT Show
- No ST elevation (no acute STEMI pattern)
- No new LBBB
- No pathological Q waves suggesting prior infarct
- No complete heart block or significant conduction abnormality
- No atrial fibrillation or flutter
Clinical Recommendations
Given this is a 51-year-old male with an abnormal ECG (nonspecific ST-T changes + borderline QTc):
- Correlate clinically - Is the patient symptomatic? Chest pain, dyspnoea, palpitations?
- Troponin I/T - to exclude acute myocardial injury
- Electrolytes (K+, Mg2+, Ca2+) - for QTc and T-wave changes
- Previous ECG comparison - Are these changes new or old? Nonspecific ST changes have far greater significance if new.
- 2D Echocardiogram - assess wall motion, LV function, LVH
- Stress test / Holter if ischemia is clinically suspected
- Review medications for QT-prolonging drugs
Important: This ECG analysis is for educational/informational purposes. Clinical decisions must be made by the treating physician with full clinical context, history, and examination findings. An "Abnormal ECG" with nonspecific changes in a 51-year-old male requires active clinical evaluation to rule out ischemic heart disease.
He is hypertensive,he has sudden chest pain,sweating
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
⚠️ High Suspicion: ACUTE CORONARY SYNDROME (ACS) - Likely NSTEMI / Unstable Angina
With the clinical context now provided - 51-year-old hypertensive male, sudden chest pain, diaphoresis (sweating) - this ECG takes on much greater urgency.
Clinical Picture Synthesis
| Finding | Significance |
|---|---|
| Age 51, Male | High-risk demographic for ACS |
| Hypertension | Major CAD risk factor |
| Sudden chest pain | Classic ischemic symptom |
| Diaphoresis (sweating) | Autonomic activation - hallmark of myocardial infarction |
| Nonspecific ST-T changes on ECG | Consistent with NSTEMI / UA |
| Borderline QTc 448 ms | Reflects myocardial stress/ischemia |
| No ST elevation | Rules out STEMI on this tracing - but NSTEMI cannot be excluded |
Sudden chest pain + sweating + abnormal ECG in a hypertensive 51-year-old male = NSTEMI / Unstable Angina until proven otherwise.
Why NOT STEMI (yet)?
- No ST elevation seen on this ECG
- No new LBBB
- However: a normal or nonspecific ECG does NOT exclude ACS - up to 6% of evolving ACS cases have a normal initial ECG. Serial ECGs are mandatory. (Sabiston Textbook of Surgery)
Differential Diagnoses to Consider
- NSTEMI - most likely given triad of symptoms + ECG changes
- Unstable Angina - if troponins return negative
- Aortic Dissection - must be considered in a hypertensive patient with sudden severe chest pain (requires CXR + CT aorta to exclude)
- STEMI equivalent - repeat ECG in 15-30 min, early changes may evolve
TIMI Risk Score (for NSTEMI/UA)
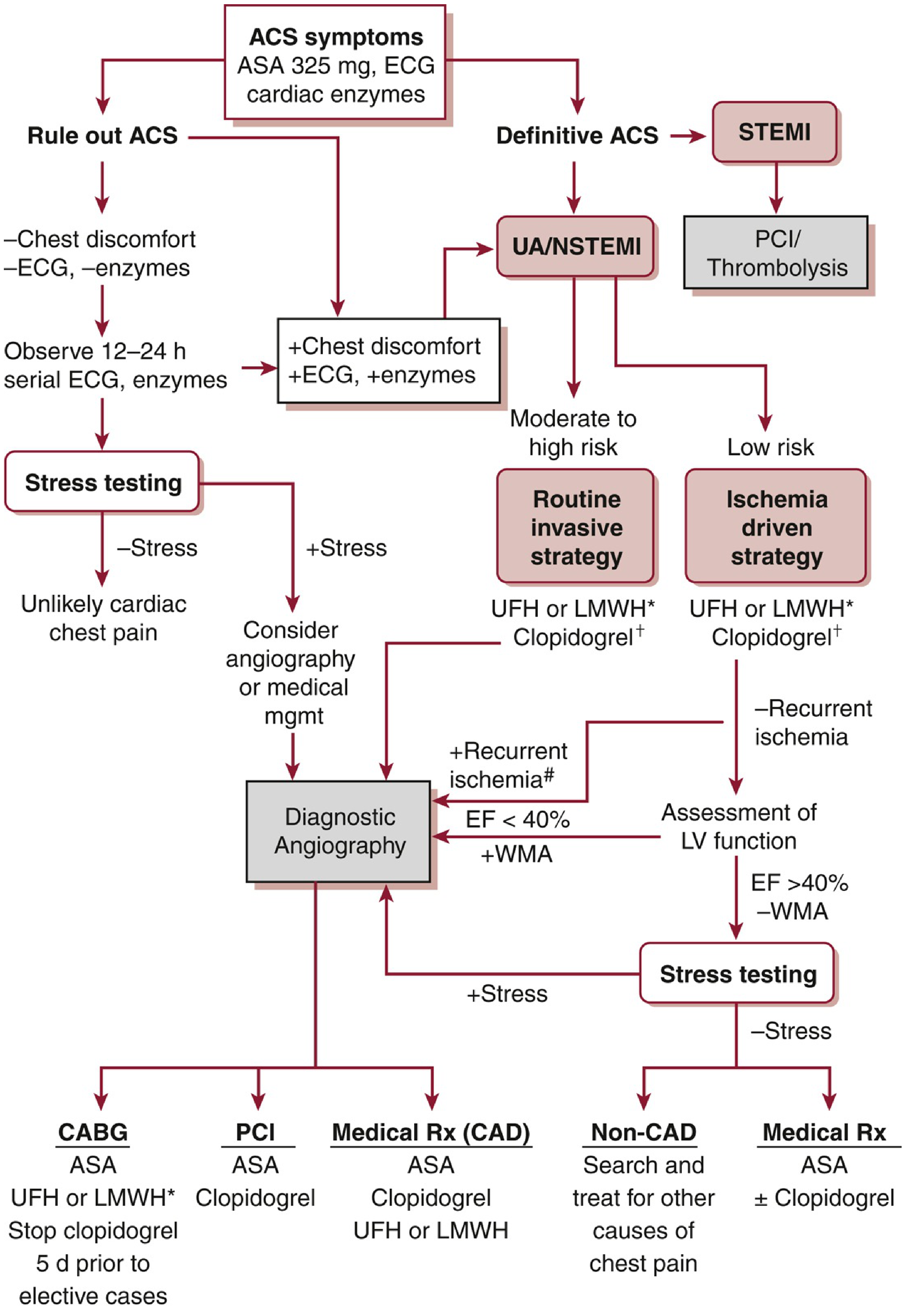
This patient scores high based on: age >45, hypertension as CAD risk factor, chest pain, ST-T changes on ECG = Moderate-High Risk → indicating Routine Invasive Strategy is appropriate.
Immediate Management Protocol
Following the ACS pathway (Washington Manual of Medical Therapeutics):
Right now - ACUTE ACTIONS:
| Priority | Action |
|---|---|
| 🔴 IMMEDIATE | IV access + continuous cardiac monitoring + pulse oximetry |
| 🔴 IMMEDIATE | 12-lead ECG repeat in 15-30 min; compare for dynamic changes |
| 🔴 IMMEDIATE | Aspirin 325 mg (loading dose, chew and swallow) |
| 🔴 IMMEDIATE | Sublingual nitroglycerin if BP allows (SBP >90 mmHg) |
| 🔴 IMMEDIATE | Troponin I or T (high-sensitivity if available) - draw now and at 3-6 hours |
| 🟠 URGENT | Dual antiplatelet therapy - add Clopidogrel 300-600 mg OR Ticagrelor 180 mg loading |
| 🟠 URGENT | Anticoagulation - LMWH (Enoxaparin) or UFH |
| 🟠 URGENT | Beta-blocker (oral, if no contraindication - HR >60, no acute HF, no bronchospasm) |
| 🟡 SOON | CXR - assess cardiac size, pulmonary congestion, mediastinum width |
| 🟡 SOON | Electrolytes, RFT, CBC, blood glucose, lipid profile |
| 🟡 SOON | 2D Echo - wall motion abnormalities |
| 🟡 SOON | Cardiology consultation for consideration of coronary angiography |
⚠️ Do NOT Miss
- If sweating + pain is very severe and blood pressure is markedly elevated or unequal in both arms → rule out Aortic Dissection (CT aortogram) before giving anticoagulants
- Monitor for arrhythmias - ischemia can precipitate VT/VF
- Do not discharge this patient without ruling out ACS with serial ECGs + troponins
This patient requires emergency hospital admission and cardiology evaluation immediately. This ECG analysis is clinical decision support - the treating physician must manage the patient based on full examination and investigations.
This is a shared conversation. Sign in to Orris to start your own chat.