Embryology of implantation anatomy
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer:
Embryology of Implantation - Anatomy
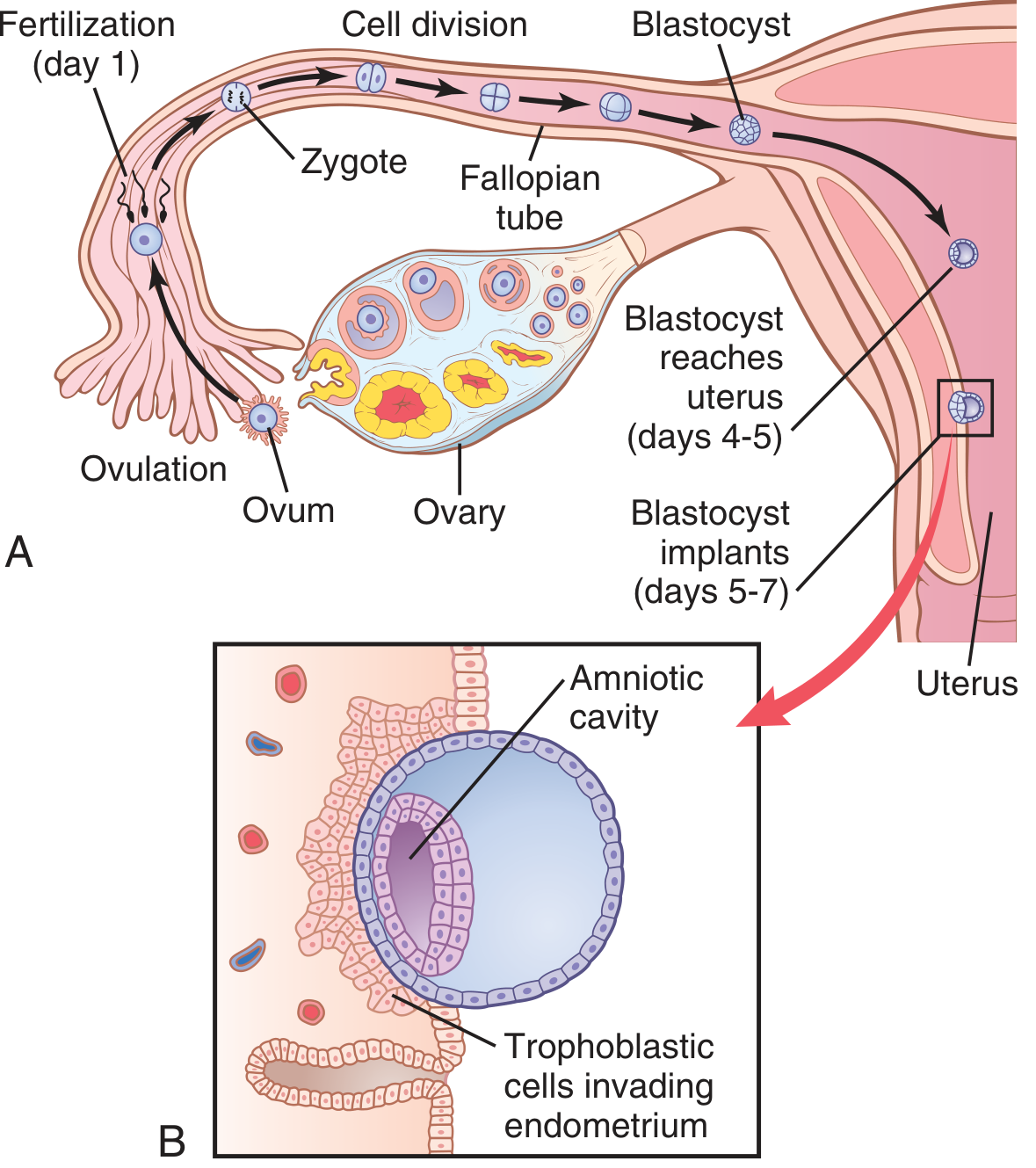
Figure: Ovulation → fertilization → cleavage stages in the fallopian tube → blastocyst reaches uterus (days 4-5) → implants (days 5-7). Inset shows trophoblastic cells invading the endometrium. (Guyton & Hall)
1. Overview - Timeline
| Event | Day (post-ovulation) |
|---|---|
| Fertilization | Day 1 |
| 2-cell → morula (16 cells) | Days 1-3 |
| Morula enters uterine cavity | Day 3-4 |
| Blastocyst forms; zona pellucida shed | Day 4-5 |
| Implantation begins (apposition) | Day 5-6 |
| Blastocyst fully embedded | Day 11 |
| Implantation window closes | Day 10 (post-LH surge) |
2. Pre-implantation Development
Cleavage & Morula
After fertilization in the ampulla of the fallopian tube, the zygote undergoes mitotic cleavage divisions. The cells (blastomeres) divide but do not grow, remaining enclosed within the zona pellucida. By day 3, the embryo has 12-16 cells and resembles a mulberry - hence the name morula (L. morum = mulberry). At the 8-cell stage, cells are still omnipotent (splitting produces identical twins).
The morula differentiates into two cell populations:
-
Embryoblast (inner cell mass/ICM): gives rise to the embryo proper
-
Trophoblast (outer cell mass): gives rise to placenta and extraembryonic membranes
-
Color Atlas of Human Anatomy Vol. 2, Internal Organs
Transport Through the Fallopian Tube
Transport takes 3-5 days, achieved by:
- Ciliated epithelium (cilia beat toward uterus)
- Fluid current from epithelial secretion
- Weak smooth muscle contractions
The isthmus of the tube stays spastically contracted for ~3 days post-ovulation. Progesterone from the corpus luteum then relaxes it, allowing entry into the uterus. This delay allows cell division to ~100 cells (blastocyst stage) before reaching the uterus. Fallopian tube secretory cells provide nutrition ("tubal milk") during this transit.
- Guyton & Hall Textbook of Medical Physiology
Blastocyst Formation
Fluid enters through the zona pellucida, forming the blastocyst cavity (blastocoele). The embryo is now a blastocyst - a hollow sphere ~100 cells. The zona pellucida then disappears, "activating" the blastocyst for implantation.
3. Anatomical Site of Normal Implantation
- Normally occurs on the posterior wall of the uterine body (most common), or the anterior wall
- Within the body of the uterus, in the functional layer of the endometrium
- The implantation pole is the embryonic pole (where the ICM lies) - polar trophoblast
The endometrium has been prepared by:
-
Estrogen → proliferative phase → thickening, increased vascularity
-
Progesterone (from corpus luteum) → secretory phase → glands enlarge, become tortuous, stroma becomes edematous
-
Gray's Anatomy for Students; Color Atlas of Human Anatomy
4. Phases of Implantation (Nidation)
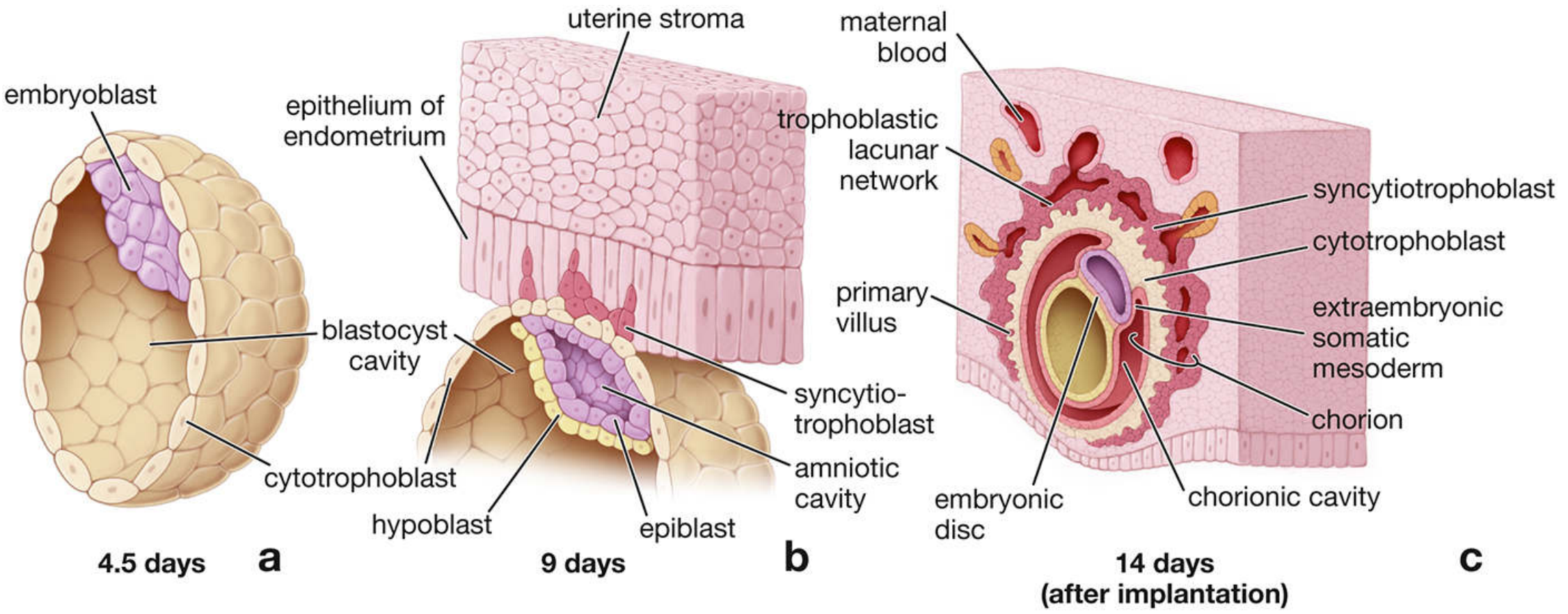
Figure: (a) 4.5 days - blastocyst with embryoblast, cytotrophoblast, blastocyst cavity. (b) 9 days - trophoblast beginning invasion of endometrial epithelium, syncytiotrophoblast forming, amniotic cavity forming. (c) 14 days - fully embedded with lacunar network, primary villi, chorionic cavity. (Histology: A Text and Atlas)
Implantation involves three sequential phases:
Phase 1 - Apposition
The blastocyst comes into loose, unstable contact with the uterine epithelium at its embryonic pole (also called the implantation pole). The embryo must be correctly oriented with the ICM facing the endometrium.
Embryo-maternal dialogue begins: The viable embryo secretes Preimplantation Factor (PIF), a 15-amino acid peptide that promotes adhesion of the embryo and later stimulates trophoblast invasion into the decidua basalis.
Phase 2 - Adhesion (The Implantation Window)
Adhesion requires specific adhesion molecules that are only available for a 24-hour window - the Window of Implantation, occurring from day 6-10 post-LH surge in humans.
Key molecular mediators:
- HB-EGF (heparin-binding epidermal growth factor-like growth factor): Most important factor. Expressed in soluble and membrane-bound forms by endometrial epithelium pinopodia. Its receptors ErbB1 and ErbB4 are on the polar trophoblast. This HB-EGF/receptor binding is the critical event in blastocyst attachment.
- LIF (Leukemia inhibitory factor): Expressed in endometrial epithelium; signals to blastocyst and epithelium for uterine receptivity.
- HOXA10 / HOXA11: Endometrial epithelial transcription factors regulating receptivity
- WNT signaling: Canonical WNT pathway in the endometrial epithelium
- Both estrogen (E2) and progesterone (P4) are necessary for HB-EGF/receptor expression
Antiprogestins (e.g., mifepristone/RU-486) block progesterone receptors in the endometrium, preventing implantation by closing this window.
- Creasy & Resnik's Maternal-Fetal Medicine; Histology: A Text and Atlas
Phase 3 - Invasion
The polar trophoblast proliferates aggressively and erodes the uterine epithelium, burrowing into the endometrial stroma. During invasion, trophoblast differentiates into two distinct layers:
5. Trophoblast Differentiation
Cytotrophoblast (CTB)
- Mitotically active inner layer of cuboidal epithelial cells
- Acts as the stem/progenitor cell layer
- Produces cells that fuse with the overlying syncytiotrophoblast
- This fusion may be triggered by programmed cell death (apoptosis)
Syncytiotrophoblast (STB)
- Outer, non-mitotically active, multinucleate cytoplasmic mass (no identifiable cell boundaries)
- Actively and aggressively invades the endometrial epithelium and underlying stroma
- Secretes proteolytic enzymes that digest and liquefy adjacent endometrial cells
- The liberated fluid and nutrients are actively transported into the blastocyst (nutrition for the early embryo)
- Contains well-developed Golgi complexes, abundant sER/rER, and mitochondria - consistent with its secretory functions
- Secretes: progesterone, estrogens, hCG, and lactogens
By approximately day 11, the blastocyst is entirely embedded within the endometrium and the endometrial epithelium closes over it.
- Histology: A Text and Atlas; Creasy & Resnik's MFM
6. Post-implantation Trophoblast Differentiation
The CTB progenitor differentiates into two lineages:
Syncytiotrophoblast (villous trophoblast)
- Multinucleated, non-invasive cells covering chorionic villi
- Serve transport and endocrine functions throughout pregnancy
Extravillous Cytotrophoblast (EVT)
- Forms within anchoring villi at the uterine junction
- Two types:
- Invasive EVT (iEVT): Invades the maternal decidua
- Endovascular EVT (eEVT): Remodels spiral arteries, converting muscular high-resistance vessels into wide, low-resistance channels to provide adequate blood flow to the placenta
- EVT express HLA-G (a key marker of invasive extravillous cytotrophoblast)
- EVT differentiation occurs under physiologic hypoxia (<30 mmHg O₂), regulated by HIF (hypoxia-inducible factor) and ASCL2
Primitive Syncytium
-
A specialized multinucleated invasive cell type (distinct from true STB)
-
Secretes enzymes breaking down decidual cells and matrix → forms lacunae (intervillous spaces)
-
Lacunae fill with endometrial glandular secretions → histiotrophic nutrition for the early embryo
-
Expresses hCG and cytokeratin 7, but NOT HLA-G
-
Creasy & Resnik's Maternal-Fetal Medicine
7. Decidualization
After implantation, the endometrium undergoes decidualization:
- The entire endometrium (except the deepest layer) becomes the decidua (decidua graviditatis) - shed with the placenta at delivery
- Stromal cells differentiate into large, rounded decidual cells (under elevated progesterone)
- Uterine glands enlarge and become coiled early, then flatten as the fetus grows
Three anatomical regions of the decidua:
| Region | Location |
|---|---|
| Decidua basalis | Between implantation site and myometrium; forms maternal part of placenta |
| Decidua capsularis | Covers the implanted embryo (superficial layer) |
| Decidua parietalis | Rest of the uterine lining not associated with implantation site |
- Histology: A Text and Atlas
8. Hormonal Support
- hCG (secreted by syncytiotrophoblast from day ~8) maintains the corpus luteum, preventing luteolysis and endometrial shedding (menstruation)
- The corpus luteum continues secreting progesterone and estrogens until the placenta takes over (~weeks 8-10)
- Without implantation: corpus luteum degenerates → progesterone/estrogen fall → menstruation
9. Abnormal Implantation
Ectopic Pregnancy
Implantation outside the uterine cavity:
- Fallopian tube (most common, ~90%) - particularly the ampulla (~78% of all ectopics)
- Ovary, abdominal cavity
- Isthmus of the tube → placenta previa if implants at the cervicouterine isthmus region of the uterus
Risk factors: prior tubal infection (50% of cases), anatomic abnormalities of the tubes, assisted reproduction (multiple embryo transfers), abnormal endometrium
Tubal implantation erodes maternal vessels → life-threatening hemorrhage.
Placenta Previa
Implantation in the lower uterine segment/isthmus → placenta obstructs the birth canal at delivery.
- Color Atlas of Human Anatomy Vol. 2; Robbins Pathology; Rosen's Emergency Medicine
Summary Diagram (Key Steps)
Ovulation (Day 0)
↓
Fertilization in ampulla of tube (Day 1)
↓
Cleavage → 2-cell → 4-cell → morula (16 cells, Day 3)
↓
Zona pellucida sheds → Blastocyst (~100 cells, Day 4-5)
↓
Blastocyst enters uterus (Day 4-5); floats free 1-3 days
↓
Apposition → Adhesion (implantation window: Day 6-10)
↓
Invasion by trophoblast (Day 6 onward)
↓
Fully embedded in endometrium (Day 11)
↓
hCG secretion → maintains corpus luteum
↓
Decidualization → primary villi → intervillous space
Sources: Guyton & Hall Textbook of Medical Physiology | Histology: A Text and Atlas (Ross & Pawlina) | Creasy & Resnik's Maternal-Fetal Medicine | Color Atlas of Human Anatomy Vol. 2 (Thieme) | Gray's Anatomy for Students
This is a shared conversation. Sign in to Orris to start your own chat.