Creatine production pathway
Reading File
Finding Sources
Finding Sources
Searching the Web
creatine biosynthesis pathway amidinotransferase guanidinoacetate methyltransferase
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple textbooks with excellent pathway diagrams. Here's a complete synthesis:
Creatine Biosynthesis Pathway
Creatine synthesis is a two-step, two-organ process using three amino acid precursors: glycine, arginine, and methionine (as SAM).
Step 1 — Guanidinoacetate formation (Kidneys)
Arginine + Glycine → Guanidinoacetate + Ornithine
Enzyme: Arginine:glycine amidinotransferase (AGAT)
The amidino group (–C(=NH)–NH₂) is transferred from arginine to glycine, producing guanidinoacetate (glycocyamine). Ornithine is released as a byproduct and re-enters the urea cycle. This step occurs primarily in the kidney (and to a lesser extent the pancreas).
Step 2 — Methylation to creatine (Liver)
Guanidinoacetate + SAM → Creatine + S-adenosylhomocysteine
Enzyme: Guanidinoacetate methyltransferase (GAMT)
SAM (S-adenosylmethionine), derived from methionine, donates its methyl group to guanidinoacetate. This reaction occurs in the liver. Creatine is then released into the circulation.
This methylation step consumes ~40% of all SAM-derived methyl groups in the body — making creatine synthesis the single largest consumer of methyl groups in human metabolism.
Pathway Diagram (Harper's Biochemistry)
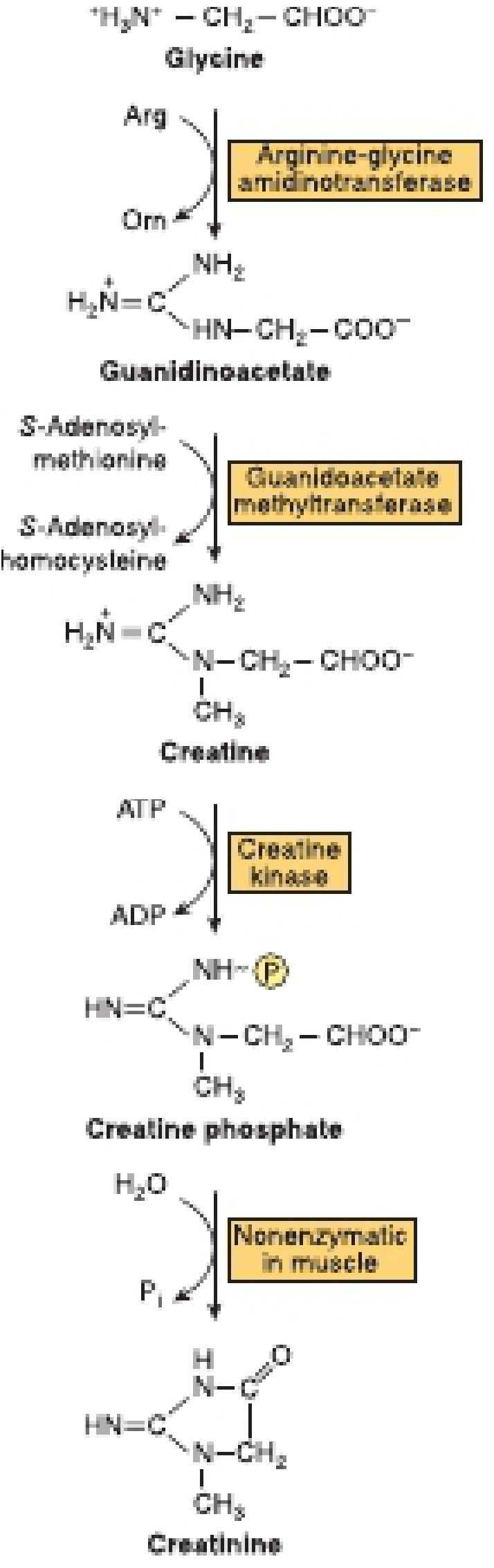
FIGURE 30-12: Biosynthesis of creatine and creatinine — Harper's Illustrated Biochemistry, 32nd Ed.
Downstream: Phosphocreatine & Creatinine
| Step | Reaction | Enzyme/Process |
|---|---|---|
| Transport | Creatine → muscle/brain via bloodstream | Creatine transporter SLC6A8 (Na⁺/Cl⁻-dependent) |
| Phosphorylation | Creatine + ATP → Creatine phosphate + ADP | Creatine kinase (CK) |
| Degradation | Creatine phosphate → Creatinine + Pᵢ | Nonenzymatic, irreversible, in muscle |
Creatinine is excreted in urine at a rate proportional to total muscle mass (~1–2 g/day in adult males), making it a clinical marker for muscle mass and renal clearance.
Organ Compartmentalization
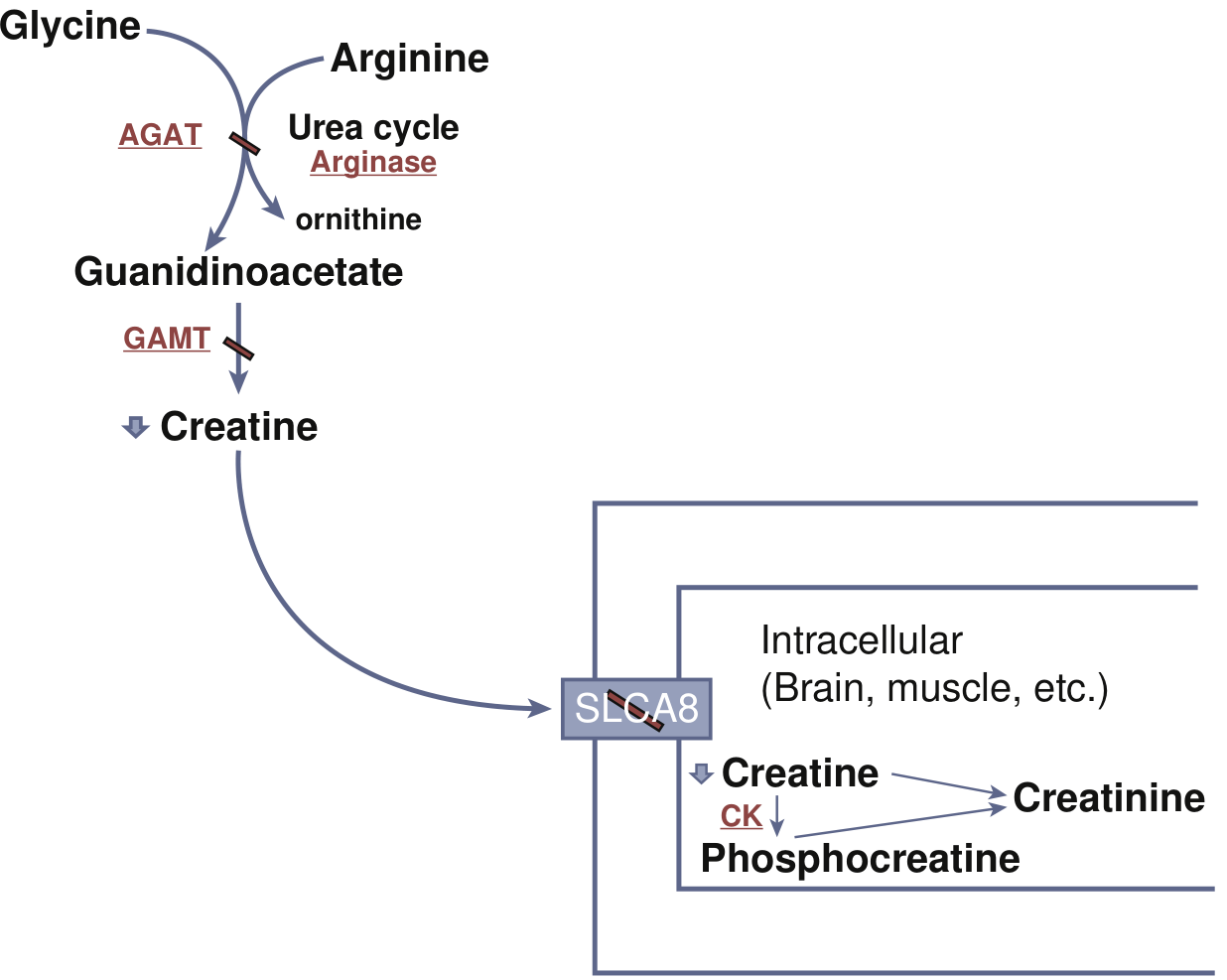
Fig. 91.11: AGAT (kidney) → guanidinoacetate → GAMT (liver) → creatine → SLC6A8 transporter → muscle/brain → CK → phosphocreatine — Bradley & Daroff's Neurology in Clinical Practice
| Organ | Role |
|---|---|
| Kidney | AGAT reaction (Step 1) |
| Liver | GAMT reaction (Step 2) |
| Muscle/Brain | Uptake via SLC6A8, phosphorylation by CK, energy buffering |
Clinical Relevance: Creatine Deficiency Syndromes
Defects in either synthetic enzyme or the transporter cause primary creatine deficiency, presenting with:
- Intellectual disability and speech/language delay
- Autistic behavior
- Epilepsy
- Hypotonia
| Defect | GAA level | Treatment |
|---|---|---|
| AGAT deficiency | ↓ GAA | Oral creatine supplementation |
| GAMT deficiency | ↑ GAA | Oral creatine supplementation |
| SLC6A8 deficiency (transporter) | Normal GAA | Poor response to supplementation |
MRS (proton magnetic resonance spectroscopy) reveals absent or markedly reduced creatine/phosphocreatine peak in all three.
Sources: Harper's Illustrated Biochemistry, 32nd Ed., p. 323 | Lippincott's Biochemistry, 8th Ed., p. 812–813 | Bradley & Daroff's Neurology in Clinical Practice, p. 1958–1959
This is a shared conversation. Sign in to Orris to start your own chat.