Short note exam oriented Malaria with diagnosis and treatment plain
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a thorough, exam-oriented short note on malaria. Let me compose the full answer.
MALARIA - Short Note (Exam Oriented)
1. Definition & Epidemiology
Malaria is a protozoan infection caused by Plasmodium species, transmitted by the bite of infected female Anopheles mosquitoes. Humans are the only natural reservoir. Globally, >200 million cases occur annually with >600,000 deaths, predominantly in sub-Saharan Africa. It remains among the top 5 causes of death in children under 5 years.
Five species infect humans:
| Species | Fever Cycle | Key Features |
|---|---|---|
| P. falciparum | 48 h (tertian) | Most dangerous; drug resistance common |
| P. vivax | 48 h (benign tertian) | Hypnozoites; relapses |
| P. ovale | 48 h | Hypnozoites; relapses |
| P. malariae | 72 h (quartan) | Recrudescence (no hypnozoites) |
| P. knowlesi | 24 h (quotidian) | Zoonotic; SE Asia |
2. Life Cycle
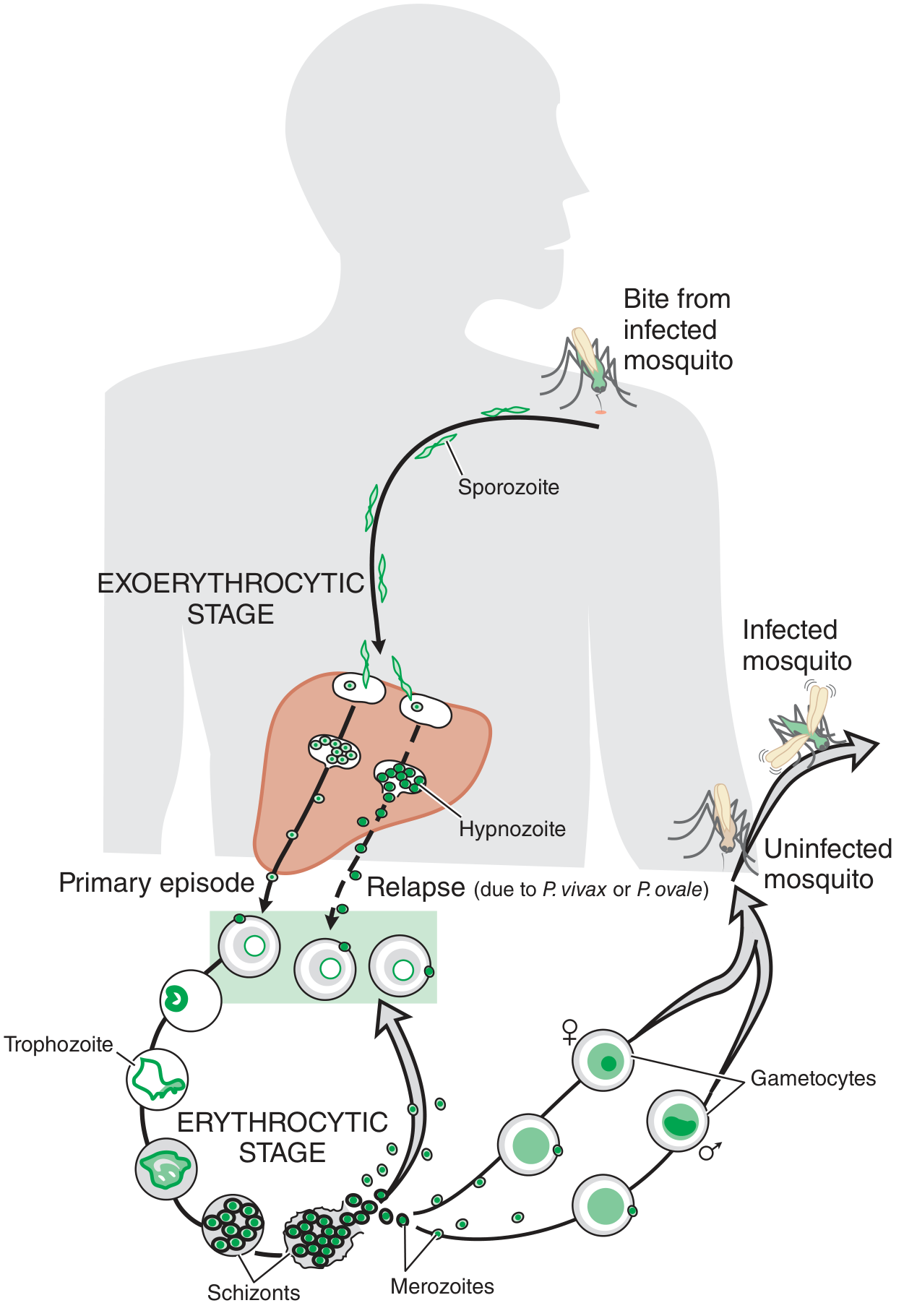
Fig. 66-2: Life cycle of malaria parasites - Goodman & Gilman's
Stages:
-
Exoerythrocytic (hepatic) stage: Sporozoites injected → travel to liver → infect hepatocytes via thrombospondin-related adhesive protein and circumsporozoite protein → develop into hepatic schizonts → release merozoites into blood (1-4 weeks incubation; asymptomatic). P. vivax and P. ovale form hypnozoites (dormant liver stage responsible for relapse).
-
Erythrocytic stage: Merozoites bind glycophorin on RBCs (via lectin-like molecule) → enter RBC → develop into ring trophozoites → schizonts → merozoites (lysis of RBC, cycle repeats every 24-72 h). Some trophozoites become gametocytes (infective to mosquito).

Fig. 10.8: P. falciparum life cycle detail - Robbins & Kumar Basic Pathology
3. Pathogenesis
- Hemolytic anemia from RBC destruction; releases hematin (malarial pigment) - discolors spleen, liver, lymph nodes, bone marrow.
- Splenomegaly (massive) and occasional hepatomegaly from mononuclear phagocyte hyperplasia.
- Cytoadherence (P. falciparum specific): PfEMP1 on knob-like extensions of infected RBCs binds endothelial adhesion molecules (ICAM-1, VCAM-1, CD36) → RBC sequestration in capillaries → cerebral malaria.
- Blackwater fever (P. falciparum): massive intravascular hemolysis → hemoglobinemia, hemoglobinuria, jaundice, acute renal failure.
4. Clinical Features
- Classic malarial paroxysm: Cold stage (rigors/chills) → Hot stage (high fever 40-41°C) → Sweating stage (drenching sweats, defervescence)
- Periodicity: Every 48 h for P. vivax/ovale/falciparum, every 72 h for P. malariae, every 24 h for P. knowlesi
- Headache, myalgia, malaise, nausea, vomiting
- Splenomegaly, anemia, jaundice
Severe/Complicated Malaria (P. falciparum):
- Cerebral malaria: altered consciousness, convulsions, coma
- Severe anemia (Hb <5 g/dL)
- Respiratory distress (pulmonary edema, ARDS)
- Hypoglycemia
- Blackwater fever (hemoglobinuria + renal failure)
- Circulatory collapse/algid malaria
- Hyperparasitemia (>5% RBCs parasitized)
5. Diagnosis
A. Microscopy (Gold Standard)
- Peripheral blood smear (thick + thin smear), Giemsa-stained
- Thick smear - for detection (more sensitive, concentrates parasites)
- Thin smear - for species identification and parasite density
- Each species has characteristic morphology (ring forms, schizonts, gametocytes)
- Should be examined every 12-24 hours if initially negative (3 negative smears before ruling out)
B. Rapid Diagnostic Tests (RDTs)
- Monovalent RDT: Detects P. falciparum HRP-2 antigen
- Bivalent RDT: Detects both P. falciparum and non-falciparum species
- Quick (~20 min), suitable where microscopy not available within 24 h
- Limitation: Cannot quantify parasitemia; false negatives with gene deletion variants
C. Other Methods
- QBC (Quantitative Buffy Coat): Fluorescent staining, detects parasites in buffy coat
- PCR: Most sensitive/specific; useful for mixed infections, low parasitemia, species confirmation; not routine
- Serology (ELISA/IFA): Indicates past exposure, not useful for acute diagnosis
- Antigen tests (pLDH, aldolase): Can detect all species; pLDH-based RDTs
6. Treatment
UNCOMPLICATED VIVAX MALARIA
| Drug | Dose | Duration |
|---|---|---|
| Chloroquine | 10 mg/kg day 1, 10 mg/kg day 2, 5 mg/kg day 3 (total 25 mg/kg) | 3 days |
| Primaquine | 0.25 mg/kg/day | 14 days |
- Primaquine eradicates hypnozoites (prevents relapse)
- Primaquine CONTRAINDICATED in: Infants, pregnant women, G6PD deficiency (causes hemolysis)
UNCOMPLICATED FALCIPARUM MALARIA
ACT (Artemisinin-Based Combination Therapy) - First Line:
| Setting | Regimen |
|---|---|
| India (non-NE states) | ACT-SP: Artesunate (50 mg) x 3 days + Sulfadoxine-Pyrimethamine (single dose on day 1) + Primaquine single dose day 2 |
| NE states (resistance) | ACT-AL: Artemether-Lumefantrine x 3 days + Primaquine single dose |
- Primaquine (single dose) given as gametocytocidal agent in falciparum (not for relapse prevention as no hypnozoites)
- Rationale for ACT: Artemisinins are fast-acting but rapidly cleared; partner drug (SP, lumefantrine) eliminates residual parasites; prevents resistance
Other effective ACTs: Artesunate + amodiaquine, Artesunate + mefloquine, Dihydroartemisinin + piperaquine
SEVERE/COMPLICATED FALCIPARUM MALARIA
Parenteral therapy - FIRST LINE:
- IV Artesunate (preferred): 2.4 mg/kg IV at 0, 12, 24 h then daily
- IV Quinine (alternative): Loading dose 20 mg/kg over 4 hours, then 10 mg/kg every 8 h (with doxycycline or clindamycin); monitor for hypoglycemia, QTc prolongation
Switch to oral ACT as soon as patient can tolerate.
CHEMOPROPHYLAXIS (Travelers)
| Drug | Dose | Timing |
|---|---|---|
| Chloroquine | 300 mg base weekly | Start 1 week before, continue 4 weeks after |
| Mefloquine | 250 mg weekly | Start 2-3 weeks before, continue 4 weeks after |
| Atovaquone-Proguanil | 250/100 mg daily | 1-2 days before, continue 7 days after |
| Doxycycline | 100 mg daily | 1-2 days before, continue 4 weeks after |
TREATMENT IN PREGNANCY
- P. vivax: Chloroquine safe; withhold primaquine (give after delivery)
- P. falciparum (uncomplicated): Quinine + clindamycin (1st trimester); ACT (2nd/3rd trimester)
- Severe malaria in pregnancy: IV artesunate or IV quinine regardless of trimester
- Avoid: Tetracyclines, doxycycline, atovaquone-proguanil, primaquine
7. Drug Resistance
- P. falciparum has developed resistance to chloroquine, mefloquine, quinine, sulfadoxine-pyrimethamine, and partially to artemisinins (Southeast Asia - kelch13 mutation)
- Mechanism: genetic mutation allowing parasite survival despite drug; propagated by sub-therapeutic dosing, incomplete courses
- Artemisinin partial resistance (K13 mutation): longer time to parasite clearance; partner drug activity preserved in most cases
8. Prevention
- Vector control: Insecticide-treated bed nets (ITNs/LLINs), indoor residual spraying
- Personal protection: Repellents (DEET), protective clothing
- Larval source management: Elimination of stagnant water bodies
- Chemoprophylaxis for travelers/non-immune individuals
- RTS,S/AS01 vaccine (Mosquirix): Partial protection (~30-50%) against P. falciparum; recommended by WHO for children in high-transmission areas in Africa
Quick Recall Summary
| P. vivax | P. falciparum | |
|---|---|---|
| Fever cycle | 48 h (benign tertian) | 48 h (malignant tertian) |
| Relapse | Yes (hypnozoites) | No (recrudescence only) |
| Drug of choice | Chloroquine + Primaquine x14 days | ACT (Artesunate-based) |
| Severe form | Rare | Cerebral malaria, blackwater fever |
| Gametocytocidal | Primaquine (for P. vivax) | Single dose primaquine |
| Resistance | CQ resistance emerging | Multi-drug resistance |
Sources: Robbins & Kumar Basic Pathology 10e, p.392 | Goodman & Gilman's Pharmacological Basis of Therapeutics 14e, Ch.66 | Park's Textbook of Preventive & Social Medicine, pp.307-310
Give me common treatment
Here is the common treatment for malaria, pulled directly from the previous detailed note:
Common Treatment of Malaria
P. VIVAX (Benign Tertian)
| Drug | Dose | Duration |
|---|---|---|
| Chloroquine | 10 mg/kg on day 1, 10 mg/kg on day 2, 5 mg/kg on day 3 (total 25 mg/kg) | 3 days |
| Primaquine | 0.25 mg/kg/day | 14 days |
- Primaquine kills hypnozoites in the liver (prevents relapse)
- Do NOT give Primaquine in: pregnancy, infants under 1 year, G6PD deficiency
P. FALCIPARUM (Malignant Tertian) - Uncomplicated
First Line: ACT (Artemisinin-Based Combination Therapy)
| India Region | Regimen |
|---|---|
| Non-NE states | Artesunate x 3 days + Sulfadoxine-Pyrimethamine (single dose, day 1) = ACT-SP |
| NE states | Artemether + Lumefantrine x 3 days = ACT-AL |
- Add single dose Primaquine on day 2 as gametocytocidal agent
- All tablets taken together with food and water
SEVERE / COMPLICATED FALCIPARUM
| Drug | Dose |
|---|---|
| IV Artesunate (preferred) | 2.4 mg/kg IV at 0, 12, 24 h then once daily |
| IV Quinine (if artesunate unavailable) | Loading 20 mg/kg over 4 h, then 10 mg/kg every 8 h |
- Switch to oral ACT as soon as patient can swallow
- Quinine: always combine with doxycycline or clindamycin; monitor blood sugar (hypoglycemia risk)
MIXED INFECTION (Falciparum + Vivax)
- Treat as falciparum first (ACT-SP or ACT-AL)
- Add Primaquine 0.25 mg/kg/day x 14 days to cover vivax hypnozoites
SPECIAL SITUATIONS
| Situation | Treatment |
|---|---|
| Pregnancy (vivax) | Chloroquine only; withhold primaquine until after delivery |
| Pregnancy (falciparum, uncomplicated) | 1st trimester: Quinine + Clindamycin; 2nd/3rd trimester: ACT |
| Pregnancy (severe) | IV Artesunate regardless of trimester |
| Children | Same drugs, weight-based dosing; avoid tetracyclines <8 yrs |
| G6PD deficiency | Avoid Primaquine entirely |
DRUGS TO REMEMBER AT A GLANCE
| Drug | Acts Against | Notes |
|---|---|---|
| Chloroquine | Blood schizonts (vivax) | Resistance in falciparum |
| Artesunate / Artemether | Blood schizonts (all species) | Fast-acting; always pair with partner drug |
| Primaquine | Hypnozoites + gametocytes | Radical cure for vivax; G6PD check before use |
| Quinine | Blood schizonts | Severe malaria backup; narrow safety margin |
| Sulfadoxine-Pyrimethamine | Blood schizonts | Partner drug in ACT-SP |
| Lumefantrine | Blood schizonts | Partner drug in ACT-AL |
Key exam point: ACT is the cornerstone of falciparum treatment. Primaquine is mandatory for vivax (14 days) and added as a single dose in falciparum (gametocytocidal). IV Artesunate is first choice for severe malaria.
This is a shared conversation. Sign in to Orris to start your own chat.