Explain aortic regurgitation
Reading File
Finding Sources
Finding Sources
Searching PubMed
"aortic regurgitation"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
aortic regurgitation echocardiography color Doppler
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Aortic Regurgitation (AR)
Aortic regurgitation (also called aortic insufficiency, AI) is the retrograde flow of blood from the aorta back into the left ventricle (LV) during diastole due to an incompetent aortic valve. It is a significant form of valvular heart disease that imposes a chronic volume overload on the LV.
1. Etiology
AR can arise from leaflet abnormalities or aortic root disease:
Valvular/leaflet causes:
- Bicuspid aortic valve (most common congenital cause; inadequately supported cusps develop progressive AR)
- Infective endocarditis (acute AR; vegetation prolapsing into LVOT)
- Rheumatic heart disease
- Myxomatous degeneration
- Systemic diseases: ankylosing spondylitis, systemic lupus erythematosus, rheumatoid arthritis, psoriatic arthritis
- Drug-related: dopamine receptor agonists and serotonin receptor agonists
Aortic root causes (functional/secondary — >50% of patients requiring AVR):
- Marfan syndrome and related connective tissue disorders (Loeys-Dietz, cystic medial necrosis)
- Hypertension-induced annuloaortic ectasia
- Aortic dissection (acute AR)
- Syphilitic aortitis
- Degenerative aortic aneurysm (sinotubular junction dilatation prevents proper leaflet coaptation)
Acute AR is most often due to infective endocarditis or aortic dissection and represents a medical/surgical emergency.
— Goldman-Cecil Medicine, p. 694; Fuster and Hurst's The Heart, p. 879
2. Pathophysiology
Chronic AR
Chronic AR imposes a combined volume and pressure overload — a feature unique among valvular lesions:
- The LV must pump both the normal forward stroke volume AND the regurgitant volume returning through the incompetent valve.
- Compensation: The LV develops eccentric hypertrophy (Laplace's law) — dilation increases end-diastolic volume (preload), allowing a greater total stroke volume while maintaining forward output. Wall thickness-to-cavity ratio remains roughly normal in the compensated phase.
- Because the increased stroke volume raises systolic pressure, there is also a degree of concentric hypertrophy (afterload excess) — distinguishing AR from pure mitral regurgitation.
- Patients with severe chronic AR have the largest LV end-diastolic volumes of any valvular disease.
- Coronary ischemia results from two mechanisms: (1) increased oxygen demand from LV hypertrophy/dilation, and (2) reduced coronary perfusion pressure — diastolic aortic pressure falls while LV diastolic pressure rises, narrowing the coronary perfusion gradient.
- Over time, adaptive mechanisms fail: EF falls, end-systolic volume rises, filling pressure rises → symptomatic heart failure. LV dysfunction may precede symptoms.
Acute AR
- The LV has no time to hypertrophy. A normal-sized LV suddenly receives a massive volume load.
- LV end-diastolic pressure rises abruptly → forward stroke volume falls → cardiogenic shock and pulmonary edema.
- Reflex vasoconstriction increases peripheral resistance (unlike chronic AR where resistance is reduced).
- Early mitral valve closure occurs from the high LV diastolic pressure (mitral valve "preclosure"), softening S1.
- Presentation: profound hypotension, tachycardia, severe dyspnea — a medical emergency requiring urgent surgery.
— Fuster and Hurst's The Heart, p. 879–880; Goldman-Cecil Medicine, p. 694; Guyton & Hall Medical Physiology, p. 293
3. Clinical Manifestations
Symptoms
Chronic AR is characteristically asymptomatic for many years — patients may tolerate a LV stroke volume twice normal before symptoms emerge:
- Dyspnea on exertion, orthopnea, fatigue (left-sided heart failure symptoms)
- Angina (less common than in AS) — may be accompanied by flushing
- Awareness of heartbeat (palpitations), carotid artery discomfort
- Once HF develops, survival without surgery is ~2 years in older patients
Acute AR presents with rapid deterioration: acute pulmonary edema, hypotension, and shock.
Physical Examination — Classic Signs of Chronic AR
The hyperdynamic circulation of chronic AR generates a remarkable constellation of signs:
| Sign | Description |
|---|---|
| Corrigan pulse (water-hammer) | Sharp upstroke and rapid collapse of the carotid pulse |
| de Musset sign | Head bobbing with each heartbeat |
| Duroziez sign | Combined systolic + diastolic bruits on femoral artery compression |
| Quincke pulse | Systolic plethora and diastolic blanching under the nail |
| Hill sign | Femoral systolic BP ≥40 mmHg higher than brachial — most reliable sign of severity |
| Displaced apex | Hyperdynamic, displaced downward and leftward |
Auscultation:
- Diastolic blowing murmur — high-pitched, decrescendo; heard best at the lower left sternal border (valvular disease) or upper right sternal border (aortic root disease), with patient sitting upright and leaning forward
- Longer murmur = more severe regurgitation
- Austin Flint murmur — a low-pitched mid-diastolic rumble at the apex, caused by the regurgitant jet impinging on the mitral valve, mimicking mitral stenosis
Acute AR is subtler — a short diastolic murmur and soft S1 (from mitral preclosure). The dramatic signs of chronic AR are absent because eccentric hypertrophy has not developed.
— Goldman-Cecil Medicine, p. 694
4. Diagnosis
ECG
Non-specific; almost always shows LV hypertrophy.
Chest X-ray
Enlarged cardiac silhouette (cardiomegaly); uncoiling and dilatation of the aortic root.
Echocardiography (Primary Diagnostic Tool)
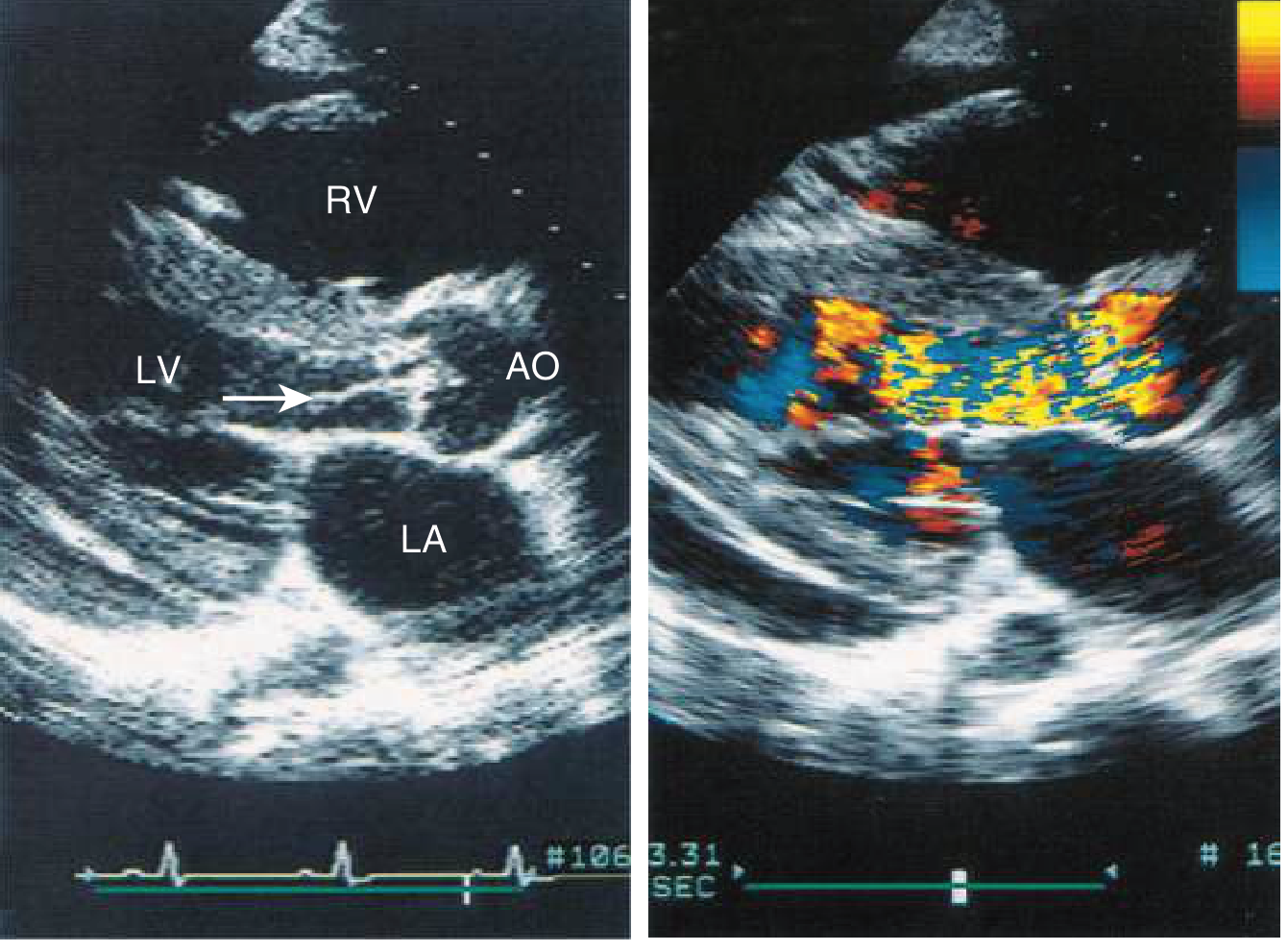
Echo quantifies:
- Regurgitant jet width/LVOT ratio (qualitative severity)
- Pressure half-time (PHT) — shorter PHT (<200 ms) = more severe AR (rapid pressure equilibration)
- Vena contracta and effective regurgitant orifice area (EROA)
- LV dimensions and EF — critical for surgical timing
- Aortic root diameter
- Holodiastolic flow reversal in the descending aorta on pulsed Doppler = severe AR
Cardiac MRI
Gold standard for precise quantification of regurgitant fraction and LV volumes, especially when echo is suboptimal.
— Goldman-Cecil Medicine, p. 694; Braunwald's Heart Disease
5. Grading Severity
| Parameter | Mild | Moderate | Severe |
|---|---|---|---|
| PHT | >500 ms | 200–500 ms | <200 ms |
| Vena contracta | <3 mm | 3–6 mm | >6 mm |
| Regurgitant volume | <30 mL | 30–59 mL | ≥60 mL |
| Regurgitant fraction | <30% | 30–49% | ≥50% |
| EROA | <0.10 cm² | 0.10–0.29 cm² | ≥0.30 cm² |
6. Natural History
- Most patients remain asymptomatic for 10+ years (chronic AR)
- Annual rate of symptom onset or LV dysfunction in asymptomatic patients with normal LV function: ~4–6%/year
- Once significant symptoms develop, expected survival without valve replacement is ~5 years
- Older individuals with HF: life expectancy without surgery is ~2 years
- LV dilation (LVESD >4.5 cm), reduced EF (<50%), and moderate or greater pulmonary hypertension predict higher mortality
- LV dysfunction may be irreversible if AVR is delayed too long
— Morgan & Mikhail's Clinical Anesthesiology; Braunwald's Heart Disease
7. Management
Medical Therapy
- Vasodilators (ACE inhibitors, ARBs, nifedipine, hydralazine) — reduce afterload and regurgitant fraction; used in chronic severe AR when surgery is not yet indicated, or in patients with hypertension; not a substitute for timely surgery
- Diuretics for volume overload/HF symptoms
- Beta-blockers: use with caution — slowing heart rate prolongs diastole, which increases the regurgitant time per beat
- Treat underlying cause (e.g., antibiotics for endocarditis)
- Acute AR: Nitroprusside ± inotropes; bridge to urgent surgical repair. IABP is contraindicated (worsens regurgitation by augmenting diastolic pressure)
Surgical Management (Aortic Valve Replacement — AVR)
Indications per ESC/EACTS and AHA/ACC guidelines:
| Indication | Class | Evidence |
|---|---|---|
| Symptomatic severe AR | I | B |
| Asymptomatic severe AR + LVEF ≤50% (ESC) or ≤55% (ACC/AHA) | I | B |
| Severe AR + undergoing other cardiac surgery (CABG, aortic repair) | I | C |
| Asymptomatic severe AR + normal EF but severe LV dilation | IIa | B |
| Progressive severe LV dilation (LVEDD >65 mm) or declining EF (55–60% on 3 serial echoes) if surgical risk low | IIb | B |
Valve repair (rather than replacement) may be preferred in bicuspid valve disease and aortic root aneurysms — especially at experienced centers.
TAVR for AR: Historically, moderate-to-severe AR has been a contraindication for TAVR (no annular calcium to anchor the device). However, newer dedicated TAVR devices and small series have shown success; TAVR may become a reliable alternative in high-risk patients.
— Fuster and Hurst's The Heart, p. 885, 910–911; Braunwald's Heart Disease
8. Acute vs. Chronic AR — Summary Comparison
| Feature | Chronic AR | Acute AR |
|---|---|---|
| LV size | Markedly enlarged | Normal |
| Pulse pressure | Wide | Narrow/normal |
| Diastolic murmur | Long, loud | Short, soft |
| Austin Flint murmur | Present in severe disease | Often absent |
| S1 intensity | Normal | Soft (mitral preclosure) |
| Peripheral signs | Present (Corrigan, Quincke, etc.) | Absent |
| Hemodynamics | Compensated → gradual decompensation | Rapid cardiogenic shock |
| Treatment urgency | Elective surgery when criteria met | Emergency surgery |
Key Teaching Points:
- AR = combined preload and afterload excess → eccentric + modest concentric hypertrophy
- The LV tolerates chronic AR well for years; symptoms herald LV dysfunction
- Surgery is indicated before irreversible LV dysfunction — don't wait for severe symptoms
- Acute AR is a surgical emergency — the clinical signs are deceptively subtle
- The Austin Flint murmur mimics mitral stenosis but disappears with nitrites (vasodilators increase forward flow, removing the jet that causes it)
This is a shared conversation. Sign in to Orris to start your own chat.