DIC complete guide from Harrison, tintinaali and other updates for emergency physician
Reading File
Finding Sources
Searching PubMed
"disseminated intravascular coagulation" AND management
Searching the Web
DIC disseminated intravascular coagulation emergency management guidelines 2024 2025
Reading File
Finding Sources
Reading Article
Reading Web Page
DIC emergency management diagnosis treatment
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading Article
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from all major sources. I have enough to write a complete, authoritative guide. Let me compile the final answer.
Disseminated Intravascular Coagulation (DIC): Complete Emergency Medicine Guide
Sources: Harrison's Principles of Internal Medicine 22E (2025), Tintinalli's Emergency Medicine 9E, Rosen's Emergency Medicine 9E, Robbins & Kumar Basic Pathology, Henry's Clinical Diagnosis & Management, ISTH 2025 criteria, Japan DIC Guidelines 2024/2025
1. DEFINITION
DIC is an acquired syndrome characterized by inappropriate, widespread intravascular activation of coagulation with loss of localization, arising from diverse underlying diseases, resulting in simultaneous:
- Systemic thrombin generation
- Fibrin deposition in the microcirculation
- Consumption of clotting factors and platelets
- Secondary fibrinolysis
The net clinical consequence is paradoxical coexistence of thrombosis AND bleeding. - Harrison's 22E, p. 977
ISTH 2025 Update: DIC is now classified into a phase-based framework:
- Pre-DIC - laboratory abnormalities without clinical symptoms
- Early-phase / Subclinical DIC - compensated; lab changes precede symptoms (detected by Sepsis-Induced Coagulopathy [SIC] score)
- Overt DIC - advanced; frank coagulopathy + organ failure
Two phenotypes are also recognized: Thrombotic DIC (microvascular thrombosis, organ failure) and Hemorrhagic DIC (consumption coagulopathy, bleeding).
2. PATHOPHYSIOLOGY
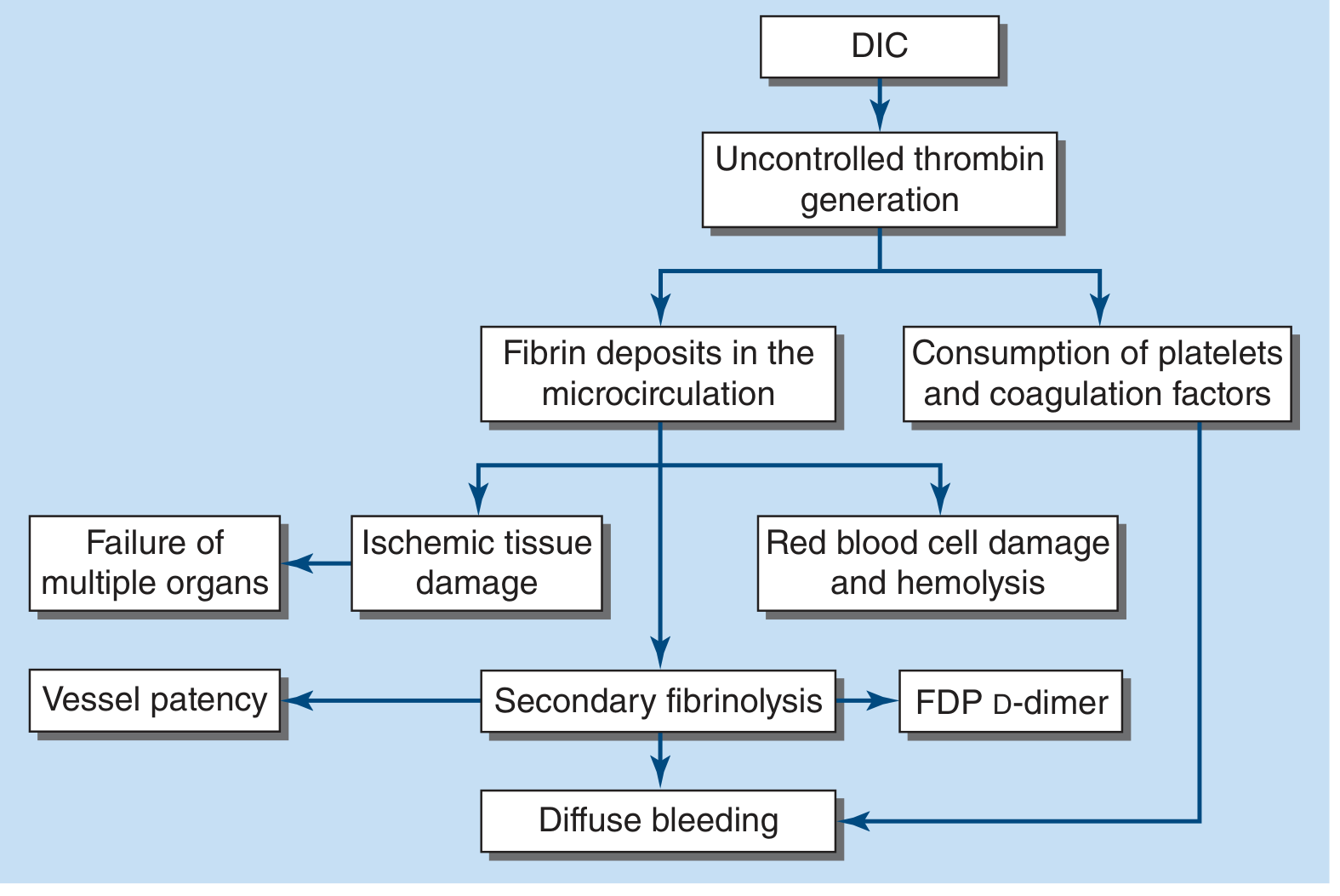
Figure: DIC pathophysiology from Harrison's 22E - uncontrolled thrombin generation leads to fibrin deposits, consumption of clotting factors/platelets, secondary fibrinolysis, and diffuse bleeding.
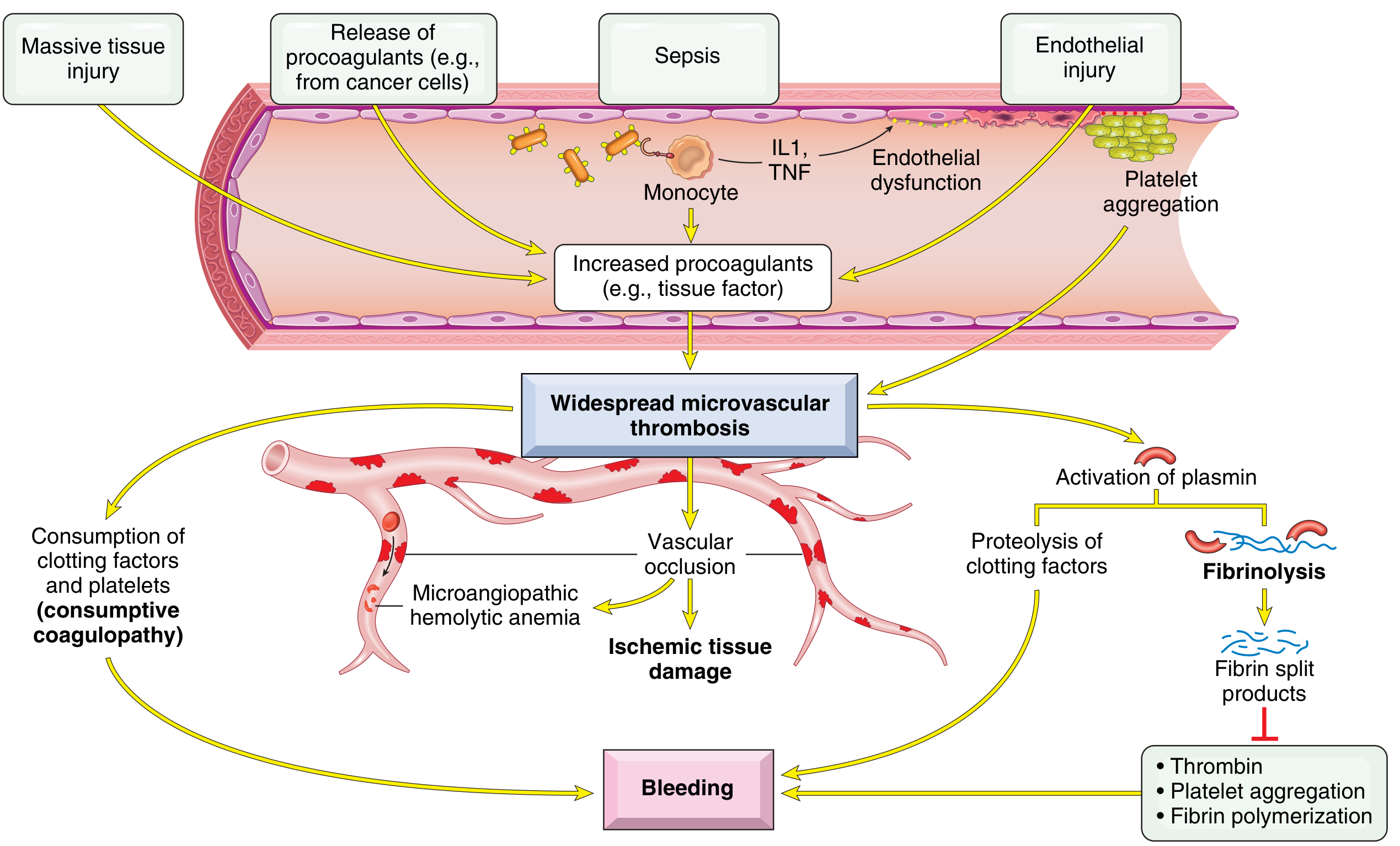
Figure: Robbins Basic Pathology - triggers (sepsis, tissue injury, endothelial damage) lead to increased tissue factor, microvascular thrombosis, fibrinolysis, and bleeding.
Molecular Cascade
Trigger 1 - Tissue Factor (TF) Release:
- Bacterial endotoxins/exotoxins stimulate monocytes to express TF
- IL-1 and TNF from activated monocytes stimulate TF on endothelial cells AND simultaneously downregulate thrombomodulin (reducing protein C activation)
- Cancer cells (especially APL, adenocarcinoma) release TF and proteolytic enzymes directly
Trigger 2 - Endothelial Injury:
- Sepsis, burns, heat stroke, immune complex deposition, meningococcemia, rickettsiae
- Exposes subendothelial collagen + vWF, releases TF, downregulates thrombomodulin
Downstream Events:
- Uncontrolled thrombin generation (thrombo-inflammation via neutrophil extracellular traps, polyphosphates)
- Fibrin deposited in small and midsize vessels → organ ischemia (lung, kidney, liver, CNS)
- Consumption of platelets + factors V, VIII, XIII, fibrinogen
- Consumption of natural anticoagulants: antithrombin III, protein C, TFPI
- Secondary fibrinolysis by plasmin → FDPs released → inhibit fibrin polymerization and platelet function → worsens bleeding
- Harrison's 22E, p. 977; Robbins Basic Pathology p. 426-427; Rosen's p. 2476
3. CAUSES / PRECIPITATING CONDITIONS
| Category | Key Examples (ED-Relevant) |
|---|---|
| Sepsis (most common) | Gram-negative (endotoxin), gram-positive, fungal; 10-20% of gram-negative sepsis develops DIC; asplenic/cirrhotic patients at higher risk |
| Trauma | Brain injury, burns, crush injury, rhabdomyolysis, hypothermia, fat embolism |
| Obstetric | Abruptio placentae, amniotic fluid embolism, septic abortion, dead fetus syndrome, HELLP syndrome |
| Malignancy | APL (bleeding > thrombosis), adenocarcinomas prostate/pancreas (Trousseau), lymphoma |
| Organ injury | Acute hepatic failure (TF released from hepatocytes), acute pancreatitis |
| Vascular | Large aortic aneurysm (chronic DIC), giant hemangioma (Kasabach-Merritt) |
| Immunologic | Acute hemolytic transfusion reaction, graft-vs-host disease |
| Envenomation | Rattlesnake/viper bites (bleeding less severe than labs suggest) |
| Miscellaneous | Massive transfusion, ARDS (20% of DIC develops ALI, 20% of ALI develops DIC), shock |
| Drugs | Fibrinolytics, amphetamines, warfarin in neonates with protein C deficiency |
- Tintinalli Table 233-6; Harrison's Table 121-2
4. CLINICAL FEATURES
Hemorrhagic Manifestations
- Oozing from IV/venipuncture sites (classic early sign)
- Petechiae, purpura, ecchymoses
- Mucosal bleeding (gingival, nasal)
- GI hemorrhage, hematuria
- Intracranial hemorrhage (severe)
- Surgical wound oozing
Thrombotic Manifestations (often under-recognized)
- Skin: acral cyanosis, digital ischemia, purpura fulminans
- Renal failure (glomerular fibrin deposition)
- Hepatic dysfunction
- ARDS (pulmonary microvascular thrombosis)
- Altered mental status, focal neurologic deficits (CNS microvascular thrombosis)
Purpura Fulminans
A severe DIC variant with extensive skin thrombosis - seen in young children after viral/bacterial infection, in protein C-deficient patients. Requires urgent heparin + protein C replacement.
Key ED Pearls
- Septic patients more often present with thrombosis than bleeding
- APL and obstetric DIC present with dominant bleeding
- Cancer-associated DIC is often chronic and compensated
- Hemodynamic instability and shock are common in acute DIC (mortality 30-80%)
- Harrison's 22E, p. 977; Tintinalli p. 1513; Rosen's p. 2476
5. DIAGNOSIS
ED Rule: DIC is a Clinical + Laboratory Diagnosis
Always require an identifiable predisposing condition before using scoring systems.
Laboratory Abnormalities
| Test | Finding | Mechanism |
|---|---|---|
| Platelet count | LOW (<100,000/mm³), or falling | Consumption in clotting |
| PT | Prolonged | Factors II, V consumed |
| aPTT | Usually prolonged | Factors II, V, VIII consumed |
| Thrombin time | Prolonged | Low fibrinogen + FDPs in circulation |
| Fibrinogen | Low (<100 mg/dL = severe DIC); may be falsely normal early (acute phase reactant) | Consumed; fibrinogen is an APR so may start elevated |
| D-dimer / FDPs | Elevated | Secondary fibrinolysis |
| Peripheral smear | Schistocytes, helmet cells (MAHA) | RBC fragmentation on fibrin strands |
| Factor VII | Low early (shortest half-life) | Consumed via extrinsic pathway |
| Factor VIII | Variable (also an APR) | - |
| Creatinine / urinalysis | May be abnormal | Renal microvascular fibrin deposition |
Fibrinogen <100 mg/dL correlates with severe DIC. Factor VII falls earliest. Fibrinogen may initially be normal or even elevated.
- Tintinalli Table 233-7; Rosen's Table 111.8; Henry's p. 954
ISTH Overt DIC Scoring System (Score ≥5 = Overt DIC)
| Parameter | Value | Points |
|---|---|---|
| Platelets | >100 × 10⁹/L | 0 |
| 50-100 × 10⁹/L | 1 | |
| <50 × 10⁹/L | 2 | |
| D-Dimer | Normal | 0 |
| Moderate increase | 2 | |
| Severe increase (>7× ULN) | 3 | |
| PT prolonged | <3 sec | 0 |
| 3-6 sec | 1 | |
| >6 sec | 2 | |
| Fibrinogen | >1 g/L (>100 mg/dL) | 0 |
| <1 g/L (<100 mg/dL) | 1 |
Score ≥5: Overt DIC - repeat daily
Score <5: Non-overt / pre-DIC - repeat every 1-2 days
2025 ISTH Update on D-dimer thresholds: Levels >3× ULN = 2 points; >7× ULN = 3 points (revised from previous criteria).
Note: Do NOT use in pregnant patients (separate pregnancy scoring system exists).
- Harrison's Table 121-3; Tintinalli Table 233-8; Henry's p. 954
Sepsis-Induced Coagulopathy (SIC) Score
Used for early-phase DIC detection in septic patients:
- Platelet count: >150=0, 100-150=1, <100=2
- INR: <1.2=0, 1.2-1.4=1, >1.4=2
- SOFA score: 0=0, 1=1, ≥2=2
- SIC score ≥4 = positive (ISTH 2025 now formally endorses SIC as an early DIC detection tool)
Differential Diagnosis
| Condition | Key Distinguishing Feature |
|---|---|
| Severe liver disease | Lab parameters stable (not rapidly worsening); clinical jaundice, splenomegaly |
| TTP | Normal PT/aPTT, ADAMTS13 inhibitor present, neurologic symptoms dominant |
| HUS | Renal failure dominant, Shiga toxin-producing E. coli history |
| ITP | Isolated thrombocytopenia, normal coagulation studies |
| Primary fibrinolysis | Rare; platelets/factor V/VIII preserved (low-normal); no thrombosis |
| HELLP | Obstetric context; hemolysis, elevated LFTs, thrombocytopenia - can coexist with DIC |
Key differentiator: In DIC, labs worsen rapidly (repeat q6-8h in critically ill). In liver disease, changes are slow. D-dimer is usually normal/minimally elevated in primary fibrinolysis and liver disease, but significantly elevated in DIC.
6. EMERGENCY MANAGEMENT
Step 1: Treat the Underlying Cause (MOST IMPORTANT)
This is the definitive treatment. All specific DIC interventions are supportive until the trigger is controlled.
- Sepsis: Broad-spectrum antibiotics + source control + fluids/vasopressors (Surviving Sepsis)
- Obstetric: Delivery, uterotonic agents (amniotic fluid embolism, abruption)
- Trauma: Damage control resuscitation, hemorrhage control
- APL: Urgent all-trans retinoic acid (ATRA) + arsenic trioxide (dramatic DIC reversal)
- Heat stroke: Active external cooling
Many episodes of DIC are self-limited (e.g., transfusion reaction) or compensated (tumor-related) and need only supportive care. - Rosen's p. 2477
Step 2: Blood Product Replacement (For ACTIVE BLEEDING Only)
CRITICAL PRINCIPLE: Do not transfuse solely to correct mildly/moderately abnormal labs. Transfuse when there is active bleeding OR planned invasive procedure OR high bleeding risk.
Platelets
- Actively bleeding: transfuse when platelets <50,000/mm³
- Prophylactic/high-risk (e.g., chemotherapy-associated DIC): transfuse when <20,000-30,000/mm³
- Target during active bleeding: >50,000/mm³
Fresh Frozen Plasma (FFP)
- Indications: active bleeding + PT/aPTT >1.5-2× normal OR fibrinogen <100 mg/dL
- Dose: 15 mL/kg (consider 30 mL/kg if volume overload not a concern)
- Replaces all clotting factors including natural anticoagulants (protein C, antithrombin)
Cryoprecipitate / Fibrinogen Concentrate
- Use when hypofibrinogenemia persists despite FFP
- Cryoprecipitate: each unit raises fibrinogen ~5-10 mg/dL; pool of 10 units typical
- Fibrinogen concentrate: when cryoprecipitate insufficient or volume is a concern
- Target fibrinogen: >150 mg/dL (Harrison's) or >100 mg/dL (Tintinalli)
Vitamin K
- Give parenterally when PT is prolonged (repletes vitamin K-dependent factors II, VII, IX, X)
Monitoring Response
-
Slowing of bleeding
-
Decrease in FDPs/D-dimer
-
Rise in platelet count and fibrinogen
-
Normalization of clotting times (this occurs later - less useful for initial monitoring)
-
Reassess frequently; repeat labs q6-8h in critically ill
-
Harrison's 22E p. 977; Tintinalli Table 233-9; Rosen's p. 2477
Step 3: Anticoagulation - Selective Use
Heparin - When to Use
- Low-grade DIC with solid tumors or APL when thrombosis dominates
- Purpura fulminans (heparin + protein C replacement)
- Recognized arterial/venous thromboembolism complicating DIC
- Acral ischemia or skin necrosis
Dosing: Low-dose continuous infusion UFH 5-10 U/kg/h (not therapeutic anticoagulation doses)
LMWH is an alternative.
Heparin - When NOT to Use
- Active hemorrhagic DIC (will aggravate bleeding)
- Meningococcemia, abruptio placentae, severe liver disease, trauma
- Heparin use in severe DIC improves coagulation parameters but has no proven survival benefit
DVT Prophylaxis
- LMWH recommended in DIC patients when bleeding is absent and platelets >30,000/mm³
Tranexamic Acid (TXA)
-
Generally avoid in DIC (risk of pathological thrombosis by blocking fibrinolysis)
-
Exception: trauma-associated DIC - TXA reduces mortality (give within 3 hours of injury)
-
Harrison's 22E p. 977-978; Tintinalli p. 1515; Rosen's p. 2477
Step 4: Other Agents (Limited/Investigational)
| Agent | Evidence | Note |
|---|---|---|
| Antithrombin III concentrate | GRADE 1B (Japan 2024 guidelines for sepsis-DIC) | Post-hoc analyses suggest survival advantage in confirmed DIC-sepsis; not standard in Western guidelines |
| Recombinant thrombomodulin | GRADE 1B (Japan 2024 guidelines) | Reduces DIC score in sepsis; approval limited to Japan |
| Activated protein C | Withdrawn from market | No benefit; increased bleeding risk |
| Recombinant factor VIIa | No proven benefit | Risk of worsening thrombosis |
| Prothrombin complex concentrate (PCC) | No proven benefit in DIC | Thrombosis risk |
| Protein C concentrate | Used in purpura fulminans, neonatal protein C deficiency | Not routine |
| Plasma exchange | Insufficient evidence to support routine use |
Japan 2024 Guidelines note: Antithrombin and recombinant thrombomodulin are recommended (GRADE 1B) for sepsis-associated DIC. Heparin and serine protease inhibitors (nafamostat) lack sufficient evidence for clear recommendation.
7. SPECIAL SITUATIONS
Obstetric DIC (ED Perspective)
- Notify obstetrics team immediately
- Delivery/evacuation of uterus is often the definitive treatment
- Amniotic fluid embolism: sudden cardiovascular collapse + DIC + bronchospasm
- HELLP: may coexist with DIC; deliver if >34 weeks or hemodynamically unstable
- Dead fetus syndrome: chronic/prothrombotic DIC (NOT hemorrhagic)
Trauma-Associated DIC
- Early coagulopathy present in 25-35% of major trauma patients on arrival
- Damage control resuscitation: balanced blood product ratio (1:1:1 PRBC:FFP:Platelets)
- TXA: give within 3 hours of injury (CRASH-2 trial)
- Avoid dilutional coagulopathy (limit crystalloids)
- Hypothermia, acidosis, hypocalcemia worsen coagulopathy ("lethal triad")
- Correct calcium (ionized Ca²⁺) - often depleted with massive transfusion
Sepsis-Associated DIC
- Most common cause of DIC globally
- 42% pooled mortality (ISTH systematic review, PMID 40383152)
- Gram-negative > gram-positive, but both can cause DIC
- Use SIC score for early detection
- Source control + antibiotics are the cornerstone
Purpura Fulminans
- Extensive skin thrombosis - limb- and life-threatening
- Therapeutic UFH infusion (if possible)
- Protein C concentrate (Ceprotin) is the preferred specific treatment
- Kcentra (4-factor PCC) or FFP if protein C concentrate unavailable
- Consider early surgical/dermatology consultation
- Stress-dose steroids for adrenal insufficiency (in meningococcemia)
Cancer-Associated DIC
- Often chronic, compensated - monitor serial labs
- APL: urgent ATRA (ALL-TRANS retinoic acid) - dramatic DIC reversal; low-dose heparin + blood products while awaiting ATRA effect
- Prostate cancer: tends toward bleeding; adenocarcinomas tend toward thrombosis (Trousseau)
8. ED DISPOSITION
- All patients with confirmed DIC require admission (usually ICU)
- Hematology consult for complex or unclear cases
- Transfer if hematologic expertise not available
- Obstetric DIC: immediate OB involvement; delivery as needed
- Serial monitoring of labs q6-8h during acute phase
9. KEY TAKEAWAYS FOR ED PHYSICIANS
- DIC is always secondary - find and treat the trigger aggressively
- Transfuse for bleeding, not numbers (except in prophylactic settings with very low platelets)
- Fibrinogen is the most specific consumptive marker but can be falsely normal early
- D-dimer alone is insufficient - use the full ISTH score with all 4 parameters
- Heparin for thrombotic DIC (APL, purpura fulminans); avoid in hemorrhagic DIC
- TXA only in trauma DIC - contraindicated in other DIC
- Septic patients get thrombosis more than bleeding - consider anticoagulation early
- LMWH prophylaxis when platelets >30,000 and no active bleeding
- Repeat labs q6-8h in critically ill - rapid worsening is characteristic
- ISTH 2025 introduced phase-based classification and refined D-dimer scoring thresholds
10. RECENT EVIDENCE UPDATES (2023-2025)
-
[ISTH 2025 New DIC Definition] (scholars.duke.edu): Updated definition now emphasizes dynamic, phase-based classification (Pre-DIC → Early-phase → Overt DIC) with thrombotic vs hemorrhagic phenotyping. D-dimer thresholds revised: >3× ULN = 2 pts, >7× ULN = 3 pts.
-
[PMID 40383152] (ISTH SSC Meta-Analysis, 2025): Pooled mortality of DIC is very high and heterogeneous - 42% in sepsis, 36% in trauma, 32% in heat stroke, 28% in leukemia. Odds ratio for mortality: 3.15 in sepsis, 4.80 in trauma. No clear improvement trend over years.
-
[PMID 39676120] (Japan DIC Guidelines 2024 - Sepsis): Recommends antithrombin (GRADE 1B) and recombinant thrombomodulin (GRADE 1B) for sepsis-associated DIC. Heparin and serine protease inhibitors lack sufficient evidence.
-
[PMID 36695377] (ISTH SSC 2023 - Sepsis-Induced Coagulopathy): SIC is now formally endorsed as the preferred tool for early DIC detection in septic patients.
Sources consulted: Harrison's Principles of Internal Medicine 22E (2025), Tintinalli's Emergency Medicine 9E, Rosen's Emergency Medicine 9E, Robbins & Kumar Basic Pathology, Henry's Clinical Diagnosis and Management by Laboratory Methods, ISTH SSC Communications, Japan DIC Clinical Practice Guidelines 2024/2025
This is a shared conversation. Sign in to Orris to start your own chat.