Intubation granuloma
Reading File
Finding Sources
Finding Sources
Searching PubMed
"intubation granuloma" larynx treatment
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Intubation Granuloma
Intubation granuloma is a benign inflammatory lesion of the larynx that arises at the vocal process of the arytenoid cartilage following endotracheal intubation. It is considered a subtype of the broader category of vocal process / contact granulomas (also called arytenoid granuloma, contact ulcer, peptic granuloma).
Epidemiology
- May occur after brief or prolonged intubation.
- More common in females when caused by intubation (in contrast to contact/hyperfunctional granulomas, which are more common in men).
- Develops typically 4-6 weeks after intubation.
Pathophysiology
The endotracheal tube causes mucosal injury and injury to the arytenoid perichondrium at the vocal process - the thinnest, most vulnerable part of the laryngeal mucosa. The resulting reparative process produces an exuberant granulation tissue response that may become:
- Sessile initially, later forming a large pedunculated lesion
- Unilateral or bilateral (frequently bilateral)
- Associated with sclerosis of the arytenoid (visible on CT scan)
In cases of prolonged intubation, additional findings may include:
- Tissue loss with posterior glottic incompetence
- Partial or complete fixation of one or both arytenoid cartilages
- Interarytenoid synechia
Histologically, these are proliferations of granulation tissue with epithelial hyperplasia. Extraoesophageal reflux is recognized as an important co-factor - either predisposing to the injury or impairing mucosal healing.
Clinical Features
| Feature | Detail |
|---|---|
| Voice change | Dysphonia or vocal fatigue; voice may sound normal if membranous vocal folds are unaffected (granuloma sits above/below vocal process during phonation) |
| Discomfort | Tickling, pain/discomfort in the posterior larynx, worse on phonation, coughing, throat clearing |
| Referred otalgia | Pain may radiate to the ear |
| Stridor | In severe cases with large obstructing lesions |
| History | Recent endotracheal intubation or direct laryngeal instrumentation |
Endoscopic Appearance
Lesions range from a nodular thickening over the vocal process to large pedunculated, exophytic masses obscuring the posterior glottis. The images below show the endoscopic appearance:
Arytenoid granuloma (laryngoscopic view):

Vocal cord lesions including intubation granuloma (panel F = intubation granuloma):
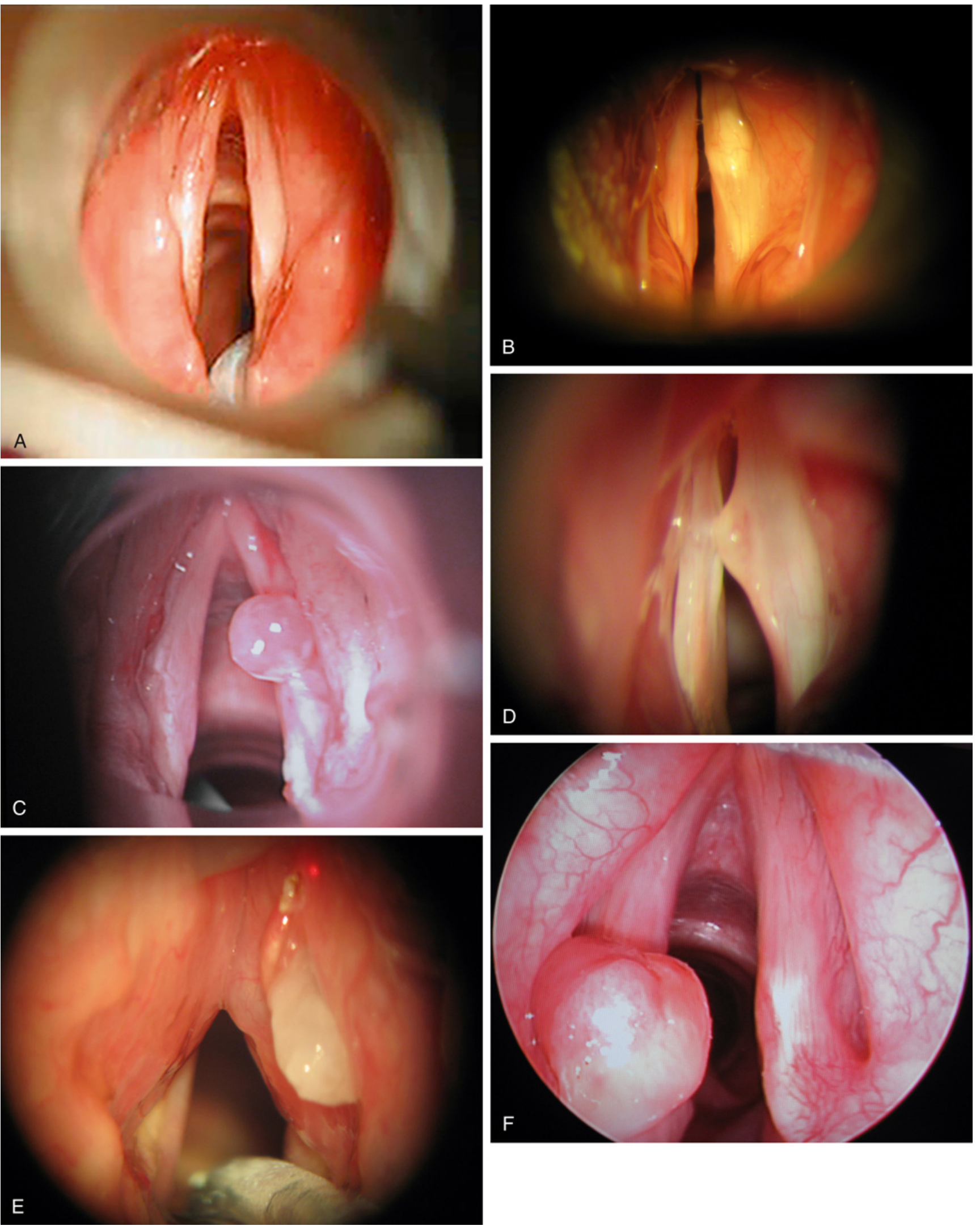
(Panel F shows the characteristic pedunculated intubation granuloma at the posterior glottis - Miller's Anesthesia)
Diagnosis
- History - recent intubation or laryngeal instrumentation
- Laryngoscopy / videostroboscopy - visual diagnosis is usually sufficient; biopsy generally not needed unless diagnosis is uncertain, carcinoma must be excluded, or the lesion is atypical
- Vocal Capability Battery - speaking voice may be surprisingly normal as the membranous vocal folds can vibrate unimpeded
- CT scan - may show arytenoid sclerosis; useful in assessing for arytenoid fixation in prolonged intubation cases
- Assessment of vocal fold motion - mandatory for recent injuries to guide management intensity
Management
Management is stratified by whether vocal fold motion is impaired:
Normal vocal fold motion (conservative approach)
- Antireflux therapy (PPIs/H2 blockers) - treats the co-factor impairing healing
- Inhaled corticosteroids - reduce inflammation
- Voice therapy - reduce hyperfunctional behaviors, throat clearing
- Smoking cessation, vocal hygiene
- Voice rest (relative)
- Watchful waiting - the lesion is best thought of as an exuberant healing response; spontaneous maturation and detachment can occur
Impaired vocal fold motion (more aggressive)
- Direct microlaryngoscopy + excision of granuloma
- Intralesional steroid injection at the time of surgery
- Surgery is a last resort because:
- Postoperative recurrence is predictable
- Spontaneous resolution is expected
- Excision should be limited, leaving the base/pedicle undisturbed
Adjunct / refractory options
- Botulinum toxin injection - reduces mechanical trauma by temporarily weakening the ipsilateral thyroarytenoid muscle
- Antibiotics (if secondary infection)
- Systemic corticosteroids
Key Differentials
| Condition | Distinguishing Feature |
|---|---|
| Contact/hyperfunctional granuloma | No intubation history; habitual low-pitched, hyperfunctional voice use; male predominance |
| Laryngeal carcinoma | Irregular, firm; persists despite conservative treatment; biopsy required |
| Laryngeal papilloma | Multiple warty lesions, HPV-related |
| Arytenoid dislocation | Sudden-onset post-intubation; arytenoid malpositioning on imaging |
| Posterior glottic stenosis | Dense scarring, bilateral arytenoid fixation |
Sources
- Cummings Otolaryngology Head and Neck Surgery, Chapter 60 (Benign Vocal Fold Mucosal Disorders)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Chapter 63 (Specific Inflammatory Conditions)
- Fishman's Pulmonary Diseases and Disorders, Chapter 47 (Endotracheal Tube-Related Trauma)
- Miller's Anesthesia, 10th ed., Chapter 66
Contact granuloma
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Searching PubMed
"contact granuloma" larynx botulinum treatment
Excellent - I have comprehensive content from Cummings and KJ Lee's, plus two key clinical image panels. I have everything needed for a thorough answer.
Contact Granuloma (Contact Ulcer / Vocal Process Granuloma)
Contact granuloma is a benign inflammatory lesion arising from the vocal process of the arytenoid cartilage, caused by repeated mechanical trauma to the thin mucoperichondrium of the posterior (cartilaginous) glottis. It overlaps with several synonymous terms:
- Contact ulcer / contact granuloma
- Vocal process granuloma
- Peptic granuloma
- Intubation granuloma (when caused by endotracheal tube)
- Contact pachydermia
Epidemiology
- Primarily affects men (in contrast to intubation granuloma, which is more common in women)
- Associated with demanding vocal occupations (clergy, teachers, lawyers, salespeople)
- Strong association with laryngopharyngeal reflux (LPR) / gastroesophageal reflux
- Psychological stress and conflict have also been suggested as contributing factors
Aetiology / Causes
| Cause | Mechanism |
|---|---|
| Vocal hyperfuntion | Habitual low-pitched, glottally-attacked, pressed phonation; "held-back" vocal quality |
| Throat clearing / chronic cough | Repeated forceful arytenoid apposition |
| LPR / GERD | Acid bathes the posterior larynx during sleep; impairs mucosal healing; perpetuates inflammation |
| Endotracheal intubation | Direct mucosal/perichondrial injury (see intubation granuloma) |
| Glottal incompetence | Vocal fold atrophy leads to compensatory hyperfunction during phonation |
| Post-surgical | Granuloma can form on the free edge of the vocal fold after laryngeal surgery |
Pathophysiology
The vocal process of the arytenoid is covered by exceptionally thin mucoperichondrium. With forceful or habitual arytenoid slamming (glottal stroke), this thin covering ulcerates and triggers a reparative response. Rather than healing cleanly, the tissue produces heaped-up granulation tissue with epithelial hyperplasia - the granuloma. LPR maintains the inflammatory milieu that prevents resolution and promotes recurrence.
Clinical Features
Symptoms:
- Unilateral discomfort or pain over the mid-thyroid cartilage, often with referred otalgia (to the ipsilateral ear)
- Foreign body sensation ("something stuck in the throat")
- Frequent throat clearing and/or chronic cough
- Voice changes - may be subtle; habitual low-pitched, monotone, or gravelly voice
- Hoarseness when the lesion becomes large
- Symptoms of LPR: morning sore throat with sour taste, acid eructations, low gravelly morning voice
Voice: May sound surprisingly normal or only slightly husky - the membranous (vibrating) portion of the vocal fold is often unaffected; the granuloma sits posterior to or above/below the plane of phonation.
Laryngoscopic Appearance
Fig. 60.26 - Contact granuloma, right posterior vocal fold. (A) Bilobed granuloma with surrounding erythema. (B) At phonatory contact, the left arytenoid fits into the cleft of the bilobed lesion.
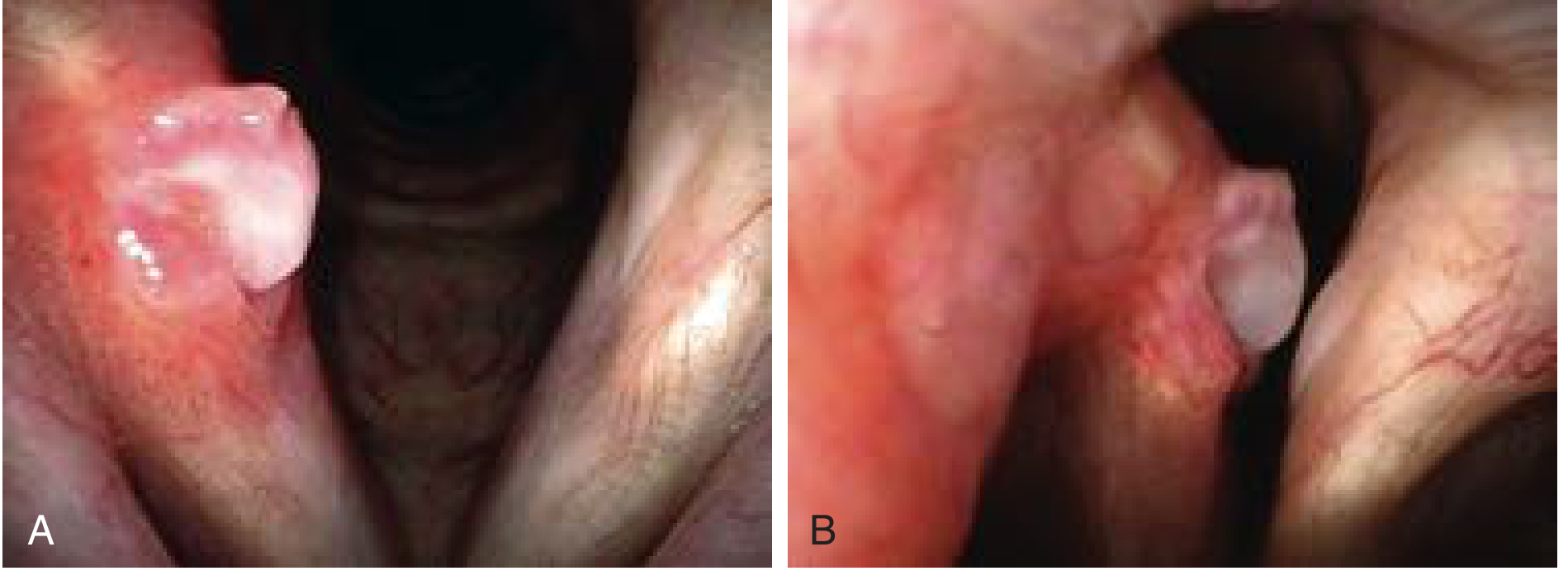
Fig. 60.27 - Natural history of spontaneous granuloma maturation and detachment. (A) Large bilobed pedunculated granuloma. (B) Months later - inferior lobe detached, single pedunculated mass remains. (C) Final detachment leaving a characteristic bruise at the base.

Key laryngoscopic features:
- Depressed, ulcerated area with whitish exudate or a bilobed, heaped-up lesion at the vocal process
- Surrounding erythema extending up the medial arytenoid surface
- Contralateral vocal process fits into the cleft of a bilobed granuloma during phonation (characteristic)
- Mature lesion: pedunculated, flips above and below the vocal fold plane with breathing/phonation
- Stroboscopy useful to identify glottal incompetence as a contributing factor
Diagnosis
- History - behavioral patterns (caffeine, alcohol, late-night eating), LPR symptoms, voice use habits, stress
- Laryngoscopy - visual diagnosis is usually sufficient; biopsy is generally not required for a classic-appearing lesion
- Rigid telescope or distal-chip camera - may be needed to detect ulcers
- Stroboscopy - identifies glottal incompetence contributing to compensatory hyperfunction
- pH monitoring / barium swallow - role remains controversial; empiric antireflux treatment is the standard approach
Management
Management is stepwise and conservative-first. Surgery is a last resort.
1. Antireflux therapy (first-line, empiric)
- PPIs (e.g., omeprazole, lansoprazole twice daily) - started empirically even without reflux symptoms
- Lifestyle modifications: avoid late meals, caffeine, alcohol, spicy foods, elevate head of bed
- Effective even in patients without overt GERD symptoms
2. Voice therapy
- Address hyperfunctional behaviors: eliminate throat clearing, raise average speaking pitch, reduce glottal attack
- Role is somewhat indeterminate given high rate of spontaneous resolution, but worthwhile in patients with clear vocal abuse patterns
3. Corticosteroids
- Intralesional depot corticosteroid injection (e.g., triamcinolone) - can be done in the office/videoendoscopy suite; lesions tend to diminish in size and symptoms resolve
- Inhaled corticosteroids (triamcinolone, mometasone) - effective alternative that avoids systemic side effects
- Patients reassessed every 6-8 weeks; treatment continued if there is size reduction and symptom improvement
4. Watchful waiting
- Spontaneous maturation and detachment occurs in 3-6 months in many cases
- The natural history shown in the image sequence above is not uncommon
5. Botulinum toxin injection (refractory cases)
- Injection into the thyroarytenoid-lateral cricoarytenoid muscle complex
- Reduces the mechanical force of arytenoid apposition
- Should be considered for refractory cases or as an adjunct to surgical removal
- Patients must be counselled that significant (temporary) dysphonia results from the injection
6. Surgery - last resort only
- Indicated for: symptomatic lesions failing conservative therapy, or when malignancy cannot be excluded
- Microlaryngoscopy with excision - removal should be limited, leaving the base/pedicle undisturbed
- Surgery alone carries a very high recurrence rate; recurrent lesions are often more recalcitrant than the original
- Postoperative recurrence of the ulcer or granuloma is predictable if underlying causes are not addressed
- Biopsy is justified if the lesion persists despite adequate conservative management (to exclude carcinoma)
Comparison: Contact Granuloma vs. Intubation Granuloma
| Feature | Contact Granuloma | Intubation Granuloma |
|---|---|---|
| Sex predominance | Men | Women |
| Aetiology | Vocal hyperfunction, LPR, throat clearing | Endotracheal tube trauma |
| Laterality | Often unilateral | Often bilateral |
| Onset | Gradual / insidious | 4-6 weeks post-extubation |
| Associated findings | Low-pitched habitual voice | Possible arytenoid fixation, posterior commissure scarring |
| Vocal fold motion | Normal | May be impaired in prolonged intubation |
Differential Diagnosis
| Condition | Distinguishing Point |
|---|---|
| Laryngeal carcinoma | Irregular, firm; does not resolve; requires biopsy |
| Laryngeal papillomatosis | Multiple warty lesions; HPV-related |
| Reinke's edema | Diffuse bilateral subepithelial gelatinous swelling; smokers |
| Arytenoid dislocation | Sudden post-intubation; malpositioning on imaging |
| Laryngeal tuberculosis | Systemic TB signs; granulomatous histology |
Sources: Cummings Otolaryngology Head and Neck Surgery, Ch. 60; KJ Lee's Essential Otolaryngology, Ch. 5; Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Ch. 63; Fishman's Pulmonary Diseases and Disorders, Ch. 47.
Contact granuloma
I just covered contact granuloma in detail in my previous response. Here's a concise summary, and let me know if you'd like me to go deeper on any specific aspect:
Contact Granuloma - Summary
Definition: Benign inflammatory lesion at the vocal process of the arytenoid cartilage, caused by repeated mechanical trauma to the thin mucoperichondrium of the posterior (cartilaginous) glottis.
Synonyms: Contact ulcer, vocal process granuloma, peptic granuloma, intubation granuloma (when ETT-related).
Key Points
| Domain | Details |
|---|---|
| Who | Primarily men; vocally demanding occupations |
| Causes | Vocal hyperfunction, LPR/GERD, chronic throat clearing, intubation |
| Location | Vocal process of arytenoid (posterior glottis) |
| Histology | Granulation tissue + epithelial hyperplasia |
| Symptoms | Odynophonia, referred otalgia, foreign body sensation, throat clearing, mild hoarseness |
| Voice | Often surprisingly normal (membranous folds unaffected) |
| Appearance | Bilobed/pedunculated mass at vocal process; surrounding erythema; contralateral arytenoid fits into the cleft at phonation |
Management (stepwise)
- PPIs - empiric antireflux therapy (even without overt reflux symptoms)
- Voice therapy - eliminate throat clearing, raise pitch, reduce glottal attack
- Inhaled / intralesional corticosteroids - triamcinolone or mometasone
- Watchful waiting - spontaneous maturation and detachment in 3-6 months is common
- Botulinum toxin (thyroarytenoid-LA muscle complex) - for refractory cases; causes temporary dysphonia
- Surgery - last resort only; high recurrence rate; leave base/pedicle undisturbed; biopsy if carcinoma cannot be excluded
Is there a specific aspect you'd like expanded - pathophysiology, LPR relationship, botulinum toxin technique, differential diagnosis, or something else?
Tuning fork tests for malingering
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
I now have comprehensive content. Let me compile the full answer, focusing specifically on tuning fork tests for malingering/pseudohypacusis.
Tuning Fork Tests for Malingering (Pseudohypacusis)
Pseudohypacusis (also called functional, nonorganic, or feigned hearing loss) refers to hearing behaviors discrepant with objective audiologic findings - either an exaggeration of a genuine hearing loss or a completely feigned one. Tuning forks provide some of the most elegant bedside tests to detect this, as they expose internal contradictions in the patient's responses.
Terminology
| Term | Meaning |
|---|---|
| Malingering | Deliberate feigning for external gain (compensation, litigation, avoiding duty) |
| Factitious disorder | Deliberate feigning for internal gain (sick role, attention) - common in children |
| Conversion disorder | Unintentional/unconscious hearing loss - no organic basis |
| Pseudohypacusis | Umbrella term covering all the above - avoids premature labelling |
Why Tuning Fork Tests Catch Malingerers
A malingerer must actively suppress their true hearing ability and give deliberately wrong responses. Tuning fork tests exploit two principles:
- Biophysics of bone conduction - sound transmitted via the skull reaches both cochleas simultaneously; a claimed "dead" ear still receives bone-conducted sound
- The Stenger principle - when two identical tones differ only in intensity, perception is referred entirely to the louder ear
Tuning Fork Tests for Malingering
1. Chimani-Moos Test (Modified Weber)
For: Unilateral claimed total deafness (dead ear)
Principle: In the standard Weber test, a bone-conducted vibrating tuning fork placed on the midline is lateralised to the better ear in unilateral sensorineural loss, or to the poorer ear in unilateral conductive loss. A malingerer claiming total unilateral deafness will lateralise the Weber to the "good" ear - but this is exploited by moving the fork.
Technique:
- Place the vibrating tuning fork on the vertex (midline)
- The malingerer claims to hear it only in the "good" ear
- Now occlude the good ear (external canal) with a finger
- Normal response / true deafness: Sound still heard only in the good (occluded) ear or disappears
- Malingerer's response: They now report hearing the tone - revealing the "deaf" ear can in fact hear bone-conducted sound that is now louder on that side
Alternatively: Place the tuning fork directly on the mastoid of the "deaf" ear
- True total SNHL: No response (cochlea genuinely dead)
- Malingerer: Either responds (revealing the ear hears) or gives an exaggerated "no" that is itself inconsistent with normal audiometry
2. Stenger Tuning Fork Test
For: Unilateral or significantly asymmetric feigned hearing loss (interaural difference ≥ 30 dB)
Principle (Stenger Effect): When two identical tones of different intensities are presented simultaneously to both ears, the listener perceives sound only in the ear receiving the louder tone - they cannot consciously hear both at once.
Technique:
- Hold one vibrating tuning fork close to the "good" ear (suprathreshold, clearly audible)
- Hold a second identical vibrating tuning fork farther away from the "bad" ear (below the patient's claimed threshold but above their true threshold)
- Negative Stenger (genuine loss): Patient responds - they hear the tone in the good ear; the tone at the bad ear is genuinely below threshold and does not interfere
- Positive Stenger (malingering): Patient does NOT respond - the tone at the "bad" ear is actually audible to them and, being the dominant signal, cancels out perception of the good-ear tone. Because the patient doesn't want to admit hearing in the bad ear, they choose silence - but silence proves the bad ear heard the louder tone
Positive Stenger = the patient heard the "bad" ear tone = feigned loss confirmed
The audiometric (pure-tone) Stenger test is the formal version of this bedside tuning fork test and is the gold standard behavioral test for unilateral pseudohypacusis.
3. Absolute Bone Conduction (ABC) Test / Schwabach Comparison
For: Claimed unilateral total deafness
Technique:
- Place a vibrating tuning fork on the mastoid of the examiner (who has known normal hearing)
- When the examiner can no longer hear it, immediately transfer it to the mastoid of the claimed "deaf" ear
- True deafness: Patient cannot hear it
- Malingering: Patient perceives the tone (because bone-conducted vibration still reaches a functioning cochlea), revealing the ear is not dead
4. Forehead/Vertex Weber Paradox
For: Claimed bilateral deafness or gross exaggeration
- In a malingerer claiming bilateral total deafness, the vibrating fork placed on the forehead/vertex should not be heard at all - but patients frequently instinctively respond, revealing intact bone conduction
5. Transcranial Bone Conduction (Dead Ear) Test
For: Claimed unilateral total sensorineural deafness
Principle: Bone-conducted sound crosses the skull with only ~0 dB of interaural attenuation (virtually none). This means a very loud bone-conducted signal placed on the skull of a "dead" ear will still reach the opposite, good cochlea.
Conversely: A tuning fork placed on the mastoid of the good ear, at a level audible to that ear, also stimulates the "dead" ear's cochlea transcranially.
- If the patient truly has a dead ear, bone-conduction thresholds on the "dead" side should match the true bone-conduction threshold of the good ear (within 5-10 dB)
- If claimed bone-conduction loss on the bad side greatly exceeds the actual bone-conduction threshold of the good ear, pseudohypacusis is unmasked
Summary of Key Tests
| Test | Principle Used | Best For | Positive Finding |
|---|---|---|---|
| Chimani-Moos (modified Weber) | Bone conduction crosses skull; occluding good ear shifts lateralisation | Claimed unilateral total deafness | Patient hears via "dead" ear when good ear occluded |
| Stenger (tuning fork) | Louder of two simultaneous identical tones dominates perception | Unilateral feigned loss (≥30 dB asymmetry) | No response when suprathreshold tone placed at "deaf" ear |
| Absolute Bone Conduction (Schwabach variant) | Residual BC transmitted to good cochlea | Claimed unilateral deafness | Patient hears fork on "deaf" mastoid |
| Vertex/forehead Weber | Instinctive response to bone-conducted vibration | Claimed bilateral total deafness | Patient responds to fork they "should not" hear |
| Transcranial BC | Interaural attenuation for BC is ~0 dB | Claimed dead ear with intact opposite cochlea | "Dead" ear BC threshold matches good ear BC |
Supporting (Non-Tuning Fork) Behavioral Clues to Malingering
- PTA-SRT discrepancy >10 dB (the two should agree within 5-10 dB) - one of the most common inconsistencies
- Poor test-retest reliability (>5 dB variation)
- Lombard test: Patient's voice gets louder when masking noise is played (proves they hear the noise)
- Delayed Auditory Feedback (DAF): Patient shows speech disturbances when hearing own voice with a delay, proving auditory self-monitoring
- Acoustic reflexes present with audiometric air-bone gaps that should have prevented them
- Good word recognition at claimed SRT level (should be impossible)
Objective Confirmation
When behavioral tests are inconclusive, objective tests provide definitive evidence:
- Otoacoustic Emissions (OAEs) - present = cochlear function is intact, regardless of claimed thresholds
- Auditory Brainstem Response (ABR) - objective threshold estimation not dependent on voluntary cooperation
- Acoustic reflexes (stapedial reflex) - present at levels below the claimed hearing threshold = functional loss
Sources: KJ Lee's Essential Otolaryngology, Ch. 2 (Behavioral Tests); Shambaugh Surgery of the Ear, Ch. 2 (Audiologic Assessment); Cummings Otolaryngology, Ch. 134 (Evaluation of Functional Hearing Loss)
This is a shared conversation. Sign in to Orris to start your own chat.