Hey Orris, can you tell me the exact diagnostic workup and treatment protocol for a child in whom we are suspecting the endemic type of Burkitt lymphoma?
Reading File
Finding Sources
Searching PubMed
"Burkitt lymphoma" AND child AND treatment
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Searching PubMed
"Burkitt lymphoma" AND "endemic" AND "children" AND diagnosis
Reading Article
PMID: 36522349
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have all the key information needed. Let me compile a comprehensive, well-structured answer.
Endemic Burkitt Lymphoma in a Child: Diagnostic Workup and Treatment Protocol
Background and Clinical Context
Endemic (African) Burkitt lymphoma (BL) is the prototypic form first described by Dennis Burkitt in 1958 in African children. It is the most rapidly proliferating human tumor (doubling time <24 hours) and a pediatric emergency. It accounts for roughly 30-50% of all childhood lymphomas and is predominantly a tumor of children in equatorial Africa, where it is tightly linked to both EBV (>90% positivity) and holoendemic Plasmodium falciparum malaria. Male predominance is noted and peak age is 4-7 years.
Step 1: Recognizing the Clinical Presentation
In a child, endemic BL most commonly presents as:
- Jaw/facial bone mass - the hallmark of the endemic form; produces the "floating tooth sign" on jaw X-ray due to destruction of tooth crypts
- Orbital mass causing proptosis
- Abdominal masses - involvement of kidneys, ovaries, and adrenal glands
- Paraspinal/epidural disease - presenting as paraplegia in up to 15%
- Rapid onset - symptoms progress over days to weeks
Unlike sporadic BL, which favors the ileocaecal region, endemic BL most characteristically involves the head and neck (jaw, orbit) and then spreads to abdominal viscera, kidneys, ovaries, and meninges. Bone marrow involvement is actually less common in endemic versus sporadic cases.
Red flag: Spontaneous tumor lysis syndrome (TLS) can occur even before chemotherapy due to the extraordinarily high proliferative rate.
Step 2: Initial Assessment and Blood Tests
Urgent bloods (to do simultaneously with biopsy planning):
| Test | Rationale |
|---|---|
| CBC with differential | Cytopenias, circulating tumor cells |
| Peripheral blood smear | Burkitt leukemia cells - medium-sized, deep blue vacuolated cytoplasm on Wright stain |
| LDH | Critical tumor burden marker and prognostic factor |
| Uric acid, phosphate, potassium, calcium, creatinine | Pre-treatment TLS screen (mandatory) |
| Urea, electrolytes, LFTs | Baseline organ function before chemotherapy |
| Serum immunoglobulins | |
| HIV serology | Exclude immunodeficiency-associated BL |
| EBV serology | High antibody titers to VCA and EBNA antigens expected; EBV DNA PCR |
| Malaria smear | In endemic areas |
| Coagulation profile | |
| Bone profile (calcium, phosphate, ALP) | Bone involvement |
Step 3: Definitive Tissue Diagnosis (Biopsy)
Biopsy is mandatory - excisional or incisional biopsy of the accessible mass (jaw, lymph node, or abdominal mass). Fine needle aspiration may be used for initial rapid cytology in resource-limited settings but is not sufficient for full classification.
Histology (H&E)
The pathognomonic appearance is the "starry sky" pattern:
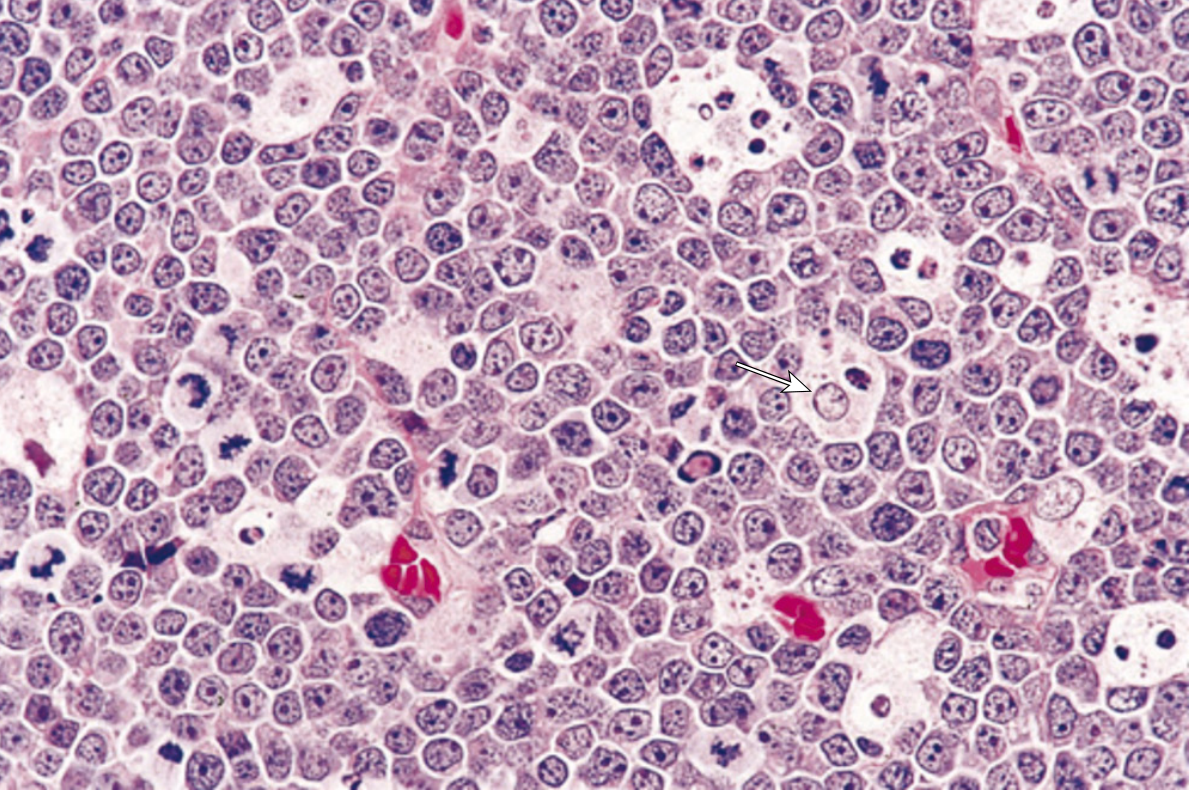
Burkitt lymphoma showing pale tangible body macrophages (arrow) giving the "starry sky" appearance. Tumor cells are monotonous medium-sized lymphocytes with multiple small nucleoli, coarse chromatin, and a very high mitotic index. (Robbins, Cotran & Kumar Pathologic Basis of Disease)
Key histologic features:
- Diffuse infiltrate of intermediate-sized monomorphic cells (10-25 µm)
- Round or oval nuclei with coarse chromatin and 3-5 prominent nucleoli in relatively clear parachromatin
- Moderate basophilic cytoplasm that "squares off" between adjacent cells
- Lipid-containing cytoplasmic vacuoles visible on imprints
- Near 100% mitotic rate (among the highest of any human tumor)
- Numerous apoptotic cells ingested by benign macrophages = the "starry sky" pattern
Immunophenotype (IHC Panel)
| Marker | Result | Significance |
|---|---|---|
| CD19, CD20, CD22, CD79a | Positive | Mature B-cell origin |
| CD10 | Positive | Germinal center origin |
| BCL6 | Positive | Germinal center origin |
| Surface Ig (sIg) | Positive, light chain restricted | Monoclonal B cell |
| Ki67 (MIB-1) | >90-100% | Near-100% proliferation rate |
| BCL2 | Negative | Critical - distinguishes from DLBCL |
| TdT | Negative | Distinguishes from lymphoblastic lymphoma |
| CD34, CD5, CD23 | Negative | |
| MYC | Positive (by IHC, >40% cut-off) | Reflects MYC translocation |
Cytogenetics/FISH (Mandatory)
- t(8;14)(q24;q32) in ~80% - MYC with IGH locus
- t(2;8) in ~15% - MYC with kappa light chain
- t(8;22) in ~5% - MYC with lambda light chain
MYC translocation by FISH is essentially required to confirm the diagnosis. The breakpoints in endemic BL are within the 5' V(D)J sequences (versus switch regions in sporadic BL).
Important note: If FISH shows MYC plus BCL2 and/or BCL6 rearrangements = "double-hit" or "triple-hit" lymphoma - a different, more refractory entity requiring different treatment.
In Touch Imprints/CSF Cytology
- Burkitt cells in peripheral blood or bone marrow aspirate: medium-sized cells with deep blue vacuolated cytoplasm on Wright stain (characteristic)
Step 4: Staging Workup
Use the International Pediatric Non-Hodgkin Lymphoma Staging System (Murphy/St. Jude staging modified for pediatrics - now called IPNHLSS):
| Stage | Definition |
|---|---|
| Stage I | Single tumor; excludes mediastinum and abdomen |
| Stage II | Single extranodal tumor with regional nodes, or 2+ nodal areas same side of diaphragm, or resectable primary GI tract tumor |
| Stage III | 2+ extranodal tumors above and/or below diaphragm; intra-abdominal/retroperitoneal disease including liver/spleen/kidney/ovary; paraspinal/epidural tumor; single bone lesion with extranodal involvement |
| Stage IV | Any above + CNS or bone marrow involvement |
Imaging:
| Investigation | Purpose |
|---|---|
| CT chest/abdomen/pelvis with contrast | Assess nodal and extranodal disease, abdominal masses |
| MRI abdomen (preferred over CT in children when available) | Better soft tissue delineation; renal, ovarian, adrenal involvement |
| FDG-PET scan | Increasingly used; assesses full metabolic disease extent and response |
| Plain jaw X-ray | "Floating tooth sign" in endemic BL |
| Skull X-ray / orbital CT | If orbital involvement suspected |
| MRI spine | If paraspinal/epidural disease or neurological symptoms |
Bone marrow biopsy:
- Bilateral iliac crest trephine biopsy is mandatory
-
25% blast replacement = reclassified as Burkitt leukemia
CSF examination (lumbar puncture):
- Mandatory for all patients
- Cell count, protein, cytospin cytology
- CSF involvement = Stage IV disease, requires intensified CNS-directed therapy
Step 5: Pre-Treatment Risk Stratification
Before initiating chemotherapy, formally assess:
- Tumor lysis syndrome risk - virtually all endemic BL children are high-risk given bulky disease
- Performance status and organ function
- CNS involvement (LP result)
- Bone marrow involvement
Initiate TLS prophylaxis immediately:
- IV hydration (3 L/m²/day without potassium or phosphate)
- Allopurinol (xanthine oxidase inhibitor); rasburicase preferred if already elevated uric acid
- Close monitoring of electrolytes every 6-8 hours
Step 6: Treatment Protocol
Treatment must be initiated urgently - BL doubles in <24 hours and is one of the few oncologic emergencies where delay by even days significantly worsens prognosis.
Preferred Regimens for Pediatric Endemic BL
1. LMB (Lymphome Malins B) Protocol - French Society of Pediatric Oncology (SFOP) - the most widely validated pediatric regimen:
The LMB regimen (also called COPAD/COPADM/CYM/CYVE depending on phase) is the global standard for pediatric BL:
- COPAD (pre-phase): Cyclophosphamide + Vincristine + Prednisone + Doxorubicin
- COPADM (induction): Above + high-dose Methotrexate (3 g/m²)
- CYM or CYVE (consolidation): Cytarabine + Etoposide (for CNS disease)
- Intrathecal therapy (IT) with methotrexate + cytarabine ± hydrocortisone is given with each cycle
- Duration: ~4-6 months total
Risk groups determine intensity:
- Group A (Stage I/II, completely resected): 2 cycles COPAD
- Group B (Stage I/IV, non-resected, no CNS/BM): COPADM x2 + CYM x2
- Group C (CNS or BM involvement): COPADM + CYVE + BM consolidation
2. Modified Magrath Regimen (CODOX-M/IVAC):
- CODOX-M: Cyclophosphamide + Vincristine + Doxorubicin + high-dose Methotrexate
- IVAC: Ifosfamide + Etoposide + high-dose Cytarabine (alternating cycles)
- Widely used internationally; excellent results in children and adults
- All regimens incorporate CNS prophylaxis - intrathecal methotrexate ± systemic high-dose methotrexate
3. DA-EPOCH-R (dose-adjusted EPOCH + Rituximab):
- Etoposide + Vincristine + Doxorubicin (continuous infusion) + Cyclophosphamide + Prednisone + Rituximab
- Emerging strong data in adolescents and adults; used at major centers
- Less data in young children
Rituximab note: All modern regimens now incorporate rituximab (anti-CD20) in children ≥2 years with adequate CD20 expression (essentially all BL). It significantly improves outcomes.
CNS-Directed Therapy (Mandatory for ALL Patients)
- Intrathecal chemotherapy with methotrexate ± cytarabine ± hydrocortisone given at every cycle
- High-dose systemic methotrexate (3-8 g/m² with leucovorin rescue) penetrates the blood-brain barrier
- Cranial radiation is generally avoided in pediatric patients due to neurocognitive late effects; it is reserved for frank CNS relapse
Tumor Lysis Syndrome Management During Treatment
- Must be anticipated before every cycle
- Hyperhydration, rasburicase, electrolyte monitoring, cardiac monitoring
- ICU admission may be required for severe TLS
Expected Outcomes
| Setting | Cure Rate |
|---|---|
| Pediatric BL in high-income settings | 80-90% |
| Endemic BL in low-income settings (often treated with less-intensive regimens) | Lower, often due to late diagnosis and treatment gaps |
| Relapsed/refractory BL | Very poor prognosis; salvage chemotherapy generally ineffective |
This highlights why early diagnosis and urgent treatment are non-negotiable.
Summary Diagnostic Pathway
Clinical suspicion (jaw mass / abdominal mass in African child)
↓
Urgent bloods: CBC, LDH, uric acid, electrolytes, creatinine, EBV serology, HIV
↓
Tissue biopsy (excisional preferred) → H&E + immunohistochemistry + FISH for MYC
↓
Bone marrow biopsy (bilateral) + LP (CSF cytology)
↓
Imaging: CT chest/abdomen/pelvis ± PET-CT ± MRI
↓
Stage using IPNHLSS (I-IV) → Risk group (A/B/C)
↓
Immediate TLS prophylaxis + urgent initiation of pediatric BL chemotherapy
(LMB protocol or Modified Magrath/CODOX-M IVAC ± rituximab)
↓
Mandatory CNS prophylaxis at every cycle
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease (10th ed.), pp. 563-564
- Harrison's Principles of Internal Medicine 22E (2025), p. 906
- Goldman-Cecil Medicine (International Edition)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2
- Henry's Clinical Diagnosis and Management by Laboratory Methods
- Grainger & Allison's Diagnostic Radiology
- López C et al. "Burkitt lymphoma." Nat Rev Dis Primers 2022. PMID: 36522349
Recent literature note (2022-2026): The 2022 Nature Reviews Disease Primers overview (PMID 36522349) emphasizes subtyping into EBV+ vs EBV- BL may better describe biological heterogeneity than the classic endemic/sporadic/immunodeficiency schema. It also reinforces that outcomes in low- and middle-income countries remain suboptimal due to late diagnosis and less-effective regimens - underscoring the importance of the workup described above even in resource-limited endemic settings.
This is a shared conversation. Sign in to Orris to start your own chat.